
Abstract
In order to understand the health outcomes for distinct sub-groups of the population or across different geographies, it is advantageous to be able to build bespoke groupings from individual level data. Individuals possess distinct characteristics, exhibit distinct behaviours and accumulate their own unique history of exposure or experiences. However, in most disciplines, not least public health, there is a lack of individual level data available outside of secure settings, especially covering large portions of the population. This paper provides detail on the creation of a synthetic micro dataset for individuals in Great Britain who have detailed attributes which can be used to model a wide range of health and other outcomes. These attributes are constructed from a range of sources including the United Kingdom Census, survey and administrative datasets. It provides a rationale for the need for this synthetic population, discusses methods for creating this dataset and provides some example results of different attribute distributions for distinct sub-population groups and over different geographical areas.
Measurement(s) | Health Disparity Populations • socio-economic outcomes |
Technology Type(s) | computational modeling technique • digital curation |
Factor Type(s) | geographical area |
Sample Characteristic - Location | Great Britain |
Similar content being viewed by others
Background & Summary
One of the central issues that researchers and policy makers face when modelling outcomes in a public health context is access to spatially representative individual-level data. Access to this data would enable researchers to examine bespoke spatial and sub-group effects of interventions and policy scenarios, thereby assessing their equability and implications within a wider policy making context. However, access to such individual level data are understandably restricted, owing to their sensitive nature. This presents a major barrier to the development of models that can inform spatially relevant interventions in a timely fashion. One way of dealing with this is the creation of synthetic data that are representative of the relationships contained within the real population.
A well established method for creating such synthetic datasets is microsimulation. In brief, microsimulation uses attribute-rich individual-level sample data to estimate the characteristics of a larger population1,2. An extension of this approach that explicitly accounts for spatial distributions is often termed spatial microsimulation3. In both microsimulation and spatial microsimulation, the resulting synthetic population dataset can be used to simulate impacts of interventions or evaluation of policy changes at an individual level which can then be aggregated over population sub-groups or geographies to calculate the overall impact of the policy scenario4.
Typically, a synthetic population generated using microsimulation has a census or other large scale coverage survey as its backbone. Depending on the focus of the research agenda being addressed, this base population can be further enriched from other data sources. There are numerous examples of this approach being successfully applied to answer key policy questions which have a spatial dimension. These include the assessment of consumer expenditure patterns5, estimating local area infrastructure demand6 and health care planning in relation to the spatial distribution of morbidities7.
Normally, the micro component of microsimulation represents units such as individuals, households or firms, which are simulated via a process of assigning attributes to those microunits from other data sources2. Spatial microsimulation adds geographical constraints and allows for the synthesis of individuals within defined geographical zones8. This combines the advantages of non-spatial attribute-rich microdata with geographically aggregated data to synthesise a population of individuals containing characteristics from both sources. It has been widely applied in many fields such as population projections (e.g.9,10), health studies (e.g.11,12), transport analysis (e.g.13,14), policy evaluation (e.g.15,16) and assessment of deprivation and inequality (e.g.17,18).
In practice, spatial microsimulation models can be either static or dynamic. Whilst a static microsimulation provides a way of generating an estimated population of individuals by synthesising data, a dynamic microsimulation is able to model changes of individual units over time and ‘age’ the static population2. Synthetic population data have been used as an input for dynamic microsimulation19 and agent based models20. They would also lend themselves to analysis using Bayesian simulations21.
In this paper, we present the rationale for, and microsimulation methods used to construct a synthetic population used by the SIPHER (Systems Science in Public Health and Health Economics Research) consortium, a collaboration of researchers from seven universities, three government partners and 12 practice partners. SIPHER’s vision is a shift from health policy to healthy public policy22 One focus area for SIPHER is to understand whether a move to an inclusive economy would benefit health and social outcomes and reduce inequalities, and if so what kinds of strategic actions decision-makers could consider. Data produced in this paper will be used as an input to models geared towards assessing relationships within a systems map of an inclusive economy and the impacts of policy interventions on a range of health and social outcomes.
For the synthetic population presented in this paper, the SIPHER requirements are (i) the creation of an individual-level population at a fine geographical level for Great Britain (GB); (ii) flexibility to combine the synthetic population with data from other sources; (iii) ability to assess the distributional effects, co-benefits and trade-offs which arise from hypothetical policy interventions; and (iv) ensuring the synthetic data could be used as an input to other dynamic policy models. In this paper we present details of the construction and validation of the synthetic population for GB, and show the population synthesis results for several geographical areas as an example of data: the city region of Greater Manchester (comprising 10 local authority districts), Sheffield local authority district, Glasgow council area and Cardiff local authority district. More specifically, we demonstrate how the SIPHER baseline population is created from the 2011 UK Census, mid-year population estimates, and the Understanding Society survey dataset.
There are many ways to use these synthetic data. In their own right they can be aggregated (to create area level information not available from the original data), cross-tabulated to reveal relationships at a given spatial scale, used to calculate summaries or metrics which provide insight in to the attributes or behaviours of different groups, and “augmented” where additional data sets are attached or integrated. By experimenting on the individual data we can create scenarios, which change the distribution of attributes. These data are also useful as the input to other individual level models. They can be used in dynamic microsimulation models which age on the population and allow for experiments and scenarios to be run which incorporate time. Synthetic data can also be fed in to agent-based models which allow users to experiment with system rules and interactions between the micro-units within the synthetic population.
In the future, using our model, it will be possible to update these data to align with the results of the 2021 UK Census once they are released. Our framework can also be used to create additional microdata using other survey or administrative datasets which contain individual level information.
Methods
This research utilises static spatial microsimulation to produce synthetic population of individuals covering the whole of Great Britain (GB) at Lower Super Output Area (LSOA) scale (administrative areas of 1500 people) for England and Wales and Data Zones (500–1000 people) for Scotland, for the year 2018 (our base year). For these models, input data normally consists of a non-geographical but otherwise attribute-rich individual level dataset, for example a representative survey, and constraint tables containing aggregate counts across a number of attributes for a series of geographical zones (e.g. LSOAs). To calculate the weights allocated to the individuals for each geographical zone, linking variables, which are shared between the individual and aggregate level datasets, are required for setting a spatial microsimulation model8. In this study, two spatial microsimulation (sub-)models are created and run separately for adults (those aged 16 and over) and children (those aged 15 and under). The overall framework and procedures for generating synthetic population and health estimates in this study is shown in Fig. 1. As the source of individual level input data, the Understanding Society survey database is processed to create adult microdata for adult microsimulation model and child microdata for the child model. Corresponding to the linking variables selected and formatted in the two micro-datasets, different geographical constraint tables are formatted based on the source data from the Office for National Statistics (ONS) or National Records of Scotland (NRS) mid-2018 population estimates, and the 2011 UK Census. Both the individual level microdata and constraint data tables are fed into each of the two microsimulation (sub-)models. After each model is run, their population outputs are merged together to generate the full synthetic population and estimates of health situations at the LSOA level are created. The whole process of synthetic data generation is detailed as follows.

Methodological framework of generating synthetic population.
Algorithm
A choice of deterministic reweighting and probabilistic methods exist for the allocation of individuals to spatial zones using microsimulation8,23,24. In this paper we utilise a combinatorial optimisation algorithm called simulated annealing to produce our synthetic dataset. Simulated annealing was compared to other microsimulation approaches by Harland et al.1 and found to outperform the alternatives in terms of total absolute error when comparing the microsimulation output with observed joint distributions for geographical zones.
Simulated annealing selects an optimal configuration from a small sample population (e.g. survey data) constrained by observed aggregate population counts (e.g. population census). It proceeds by randomly selecting individuals from the microdata and considering them for admittance into the population of a small area if they improve the goodness of fit of the population to the benchmark tables (constraint tables)1,25. The aggregation and fit evaluation is repeated, and new individuals replace the old ones in the small area if the fit is improved. Since the weights applied to members of a sample population are either one (if the individual is selected) or zero (if the individual is excluded), the synthetic population generated is a realistic representation of the observed population aligning closely to the constraint tables whilst maintaining the rich attributes provided by the survey sample population26.
Software
There are a variety of ways to build and run microsimulation models. These include using custom software packages and specifying models in a development language. This study applies a Java based application, the Flexible Modelling Framework (FMF) which incorporates a static spatial microsimulation algorithm based on Simulated Annealing27. It also has a Graphical User Interface (GUI) which allows the users to select input data files and specify required linkages, options and outputs. In addition, the FMF includes a model evaluation function that enables internal model validation by calculating goodness-of-fit statistics (e.g. R2, Total Absolute Error, Standard Absolute Error, Standardised Root Mean Square Error) at individual cell, category and overall attribute levels.
Microdata-Understanding society (the UK household longitudinal study)
The microdata (non-geographical individual level data) used for this study are derived from a nationally representative longitudinal household survey-Understanding Society (the UK Household Longitudinal Study)?. The initial household sample size of the first wave (2009-10) was around 40,000, and it collects data from household members aged 10 and above on an annual basis. Sample members are followed when they leave a household, and new individuals join the study as they become part of existing sample member households. The survey fieldwork period is 24 months for each wave, with each individual interviewed at 12-month intervals. The main survey of Understanding Society consists of two components, which include an individual adult survey completed by respondents aged 16 and over and a youth survey completed by young people aged 10-15. We use the adult survey data to create the input microdata for microsimulation process. Base data simulated in this paper uses wave 9 of the survey, conducted in 2018.
Selecting and formatting linking variables in the microdata
Understanding Society’s adult survey collects a range of health and socio-economic information about individuals and a number of these align with the mid-year population estimates data and census data used as the spatial constraints (i.e. geographically aggregated dataset) in our spatial microsimulation. We use eight variables in the adult individual dataset linking to constraints: sex, age, economic activity, highest educational qualification, marital status, ethnic group, composition of household, and housing tenure. Sex and age are combined. Because unified variable classes for the microdata and corresponding constraint dataset are required for the microsimulation process, the original variables in the microdata needs to be re-categorised to generate the appropriate classes which is compatible with constraint variables derived from the mid-year population estimates and census data. These are summarised in Table 1.
Table 2 shows an example extract of the formatted socio-demographic microdata of adults (note these are not real records) from Understanding Society.
Child microdata
The child microdata is newly-formed by extracting the information about the adult respondents’ children (aged 15 and under) recorded in the Understanding Society’s adult survey dataset. Compared to the adult microsimulation model which uses eight variables which map to the 2011 Census data, the child microsimulation model is simpler because the linking variables shared between the Understanding Society survey data and geographically aggregated data are limited. Many of the socio-demographic variables, such as economic activity, highest qualification, and marital status, are not available or applicable for children in both source datasets. A simpler microsimulation model is also deemed appropriate since the information on children’s health provided by the original child microdata is not as rich as the health-related information for adults. In this case, only sex and age variables are selected from the original child dataset to form the sex/age variable with six cross-tabulated categories for microsimulation purpose, including “M_0_4” (male, aged 0–4 years), “M_5_11” (male, aged 5–11 years), “M_12_15” (male, aged 12–15 years), “F_0_4” (female, aged 0–4 years), “F_5_11” (female, aged 5–11 years), and “F_12_ 15” (female, aged 12–15 years).
Formatting geographical constraint variables
Tables which report the total count of individuals for each of the nine variables outlined in Table 1 for each geographical zone are used as constraints in the microsimulation. The source of these constraints are outlined in Table 3.
The sex/age constraints come from the Office for National Statistics (ONS) mid-2018 population estimates for England and Wales and the National Records of Scotland (NRS) mid-2018 population estimates for Scotland. These are formatted to match the age categories in the microdata and an extract from the constraint data can be seen in Table 4. This dataset is then split in to an adult constraint dataset and a child constraint dataset. The child microsimulation model is then run using only age and sex constraints as discussed earlier.
For the adult model, further constraints are derived from 2011 Census data. Because the total number of people in 2011 does not match the total in 2018, the Census tables are scaled to match the age and sex totals reported in the mid-2018 data for each geographical zone. An example of the economic status and educational level constraint can be seen in Table 5, an extract from the marital status and ethnicity constraints in Table 6 and from the household composition and tenure constraint tables in Table 7. The simulated annealing algorithm is applied to these constraints and the microdata as described earlier.
Usage Notes
Once the microsimulation process is complete, the synthetic population data, containing individual personal identifiers and the codes of LSOA zones that each individual is allocated to, are generated. This means that variables that are not otherwise available at a high resolution geography can be made available to researchers. Examples of these variables are provided in Table 8, including subjective wellbeing, physical and mental health conditions, and household income, all of which are reported in original Understanding Society’s adult survey data but not readily available from any existing geographically aggregated data sources. In the original survey data, subjective wellbeing scales run from 0 to 36 for Likert score and 0 to 12 for Caseness score. For either scoring method, a higher score suggests a more distressed situation the individuals are facing. SF-12 Physical or Mental Component Summary is a continuous scale with a range of 0 (low functioning) to 100 (high functioning). A higher score indicates a healthier condition the individuals have.
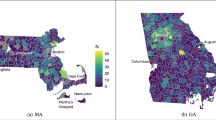
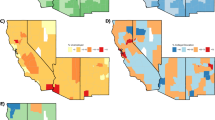
The spatial distributions of these variables (and any other variables within the dataset) can be mapped by joining the geographically aggregated dataset with the 2011 Census geography boundaries. Figure 2 gives an example of the spatial resolution of the data that is deposited across the four different GB city regions.

Examples of aggregated health conditions estimates at LSOA and equivalent level in the four selected city regions.
Data Records
The dataset of aggregated average health conditions and average household income at the LSOA level for the four city regions described above is publicly and freely available through Figshare28. The input datasets for microsimulation model development, Understanding Society29 survey data, can be accessed through the UK Data Service. Accessing datasets from the UK Data Service normally requires online registration if users are in the UK and their organisation is part of the UK Access Management Federation (UKAMF). For users who are not in the UK or their organisation is not on the list of the UKAMF, an online application for username is required before they can register on the UK Data Service (more details are available from: https://beta.ukdataservice.ac.uk/myaccount/login). Meanwhile, the geographically aggregated data used to form constraints can be accessed from the sources listed in Table 3.
Technical Validation
There are a range of methods available for validation of spatial microsimulation models, which can be broadly categorised as internal (in-sample, or endogenous) validation and external (out-of-sample, or exogenous) validation23,30.
Internal validation
Internal validation refers to comparing values from the simulated dataset to the original datasets used in the simulation8. In practice, this process includes model calibration, whereby the model fit is assessed by comparing the observed and simulated values for constraint variables. Although there are a variety of established measures of internal fit that have been used for model validation, no consensus has been reached yet regarding the most meaningful measure to compare simulated and actual values31. Following suggestions from Lovelace and Dumont8, internal validation was performed by calculating the overall values of three commonly-used fit statistics: R2, Standardised Root Mean Square Error (SRMSE), and Relative Error (RE) for each constraint variable (summarised in Table 9). The goodness-of-fit statistics show a good fit between the simulated and original data: correlations are high and relative error is low.
External validation
External validation is the process of comparing the simulated results to a different source of data that is external to the model. If external geo-coded survey data are available, this approach can take place at the individual level. But more commonly, it is performed at the aggregated level8 given that microsimulation models are used to estimate the data that do not otherwise exist or are not accessible. In this study, the simulation results are compared with estimates from external datasets that are available at higher levels of spatial aggregation (Lower and Middle Layer Super Output Areas). Simulated outputs are aggregated up to match the geographical scale.
The Index of Multiple Deprivation 2019 (IMD 2019) (https://www.gov.uk/government/statistics/english-indices-of-deprivation-2019), the Welsh Index of Multiple Deprivation 2019 (WIMD 2019) (https://gov.wales/welsh-index-multiple-deprivation-full-index-update-ranks-2019), and the Scottish Index of Multiple Deprivation 2020 (SIMD 2020) (https://www.gov.scot/collections/scottish-index-of-multiple-deprivation-2020/) are the official measurements of relative deprivation for small areas (LSOAs or Data Zones) in England, Wales, and Scotland. Several studies have examined the relationships between socio-economic status, deprivation and individuals’ health conditions, as well as (personal or household) income. These studies generally suggest that people from more affluent households, less deprived areas or of a higher socio-economic status tend to have higher-level incomes and wellbeing and are in better health (e.g.32,33,34,35,36).
The IMD 2019 is organised across seven distinct domains of deprivation: income deprivation, employment deprivation, health deprivation and disability, education skills and training deprivation, barriers to housing and services, living environment deprivation, and crime. Those domains are combined and weighted appropriately to calculate the IMD which represents an overall measure of multiple deprivation experienced by people living in specific areas (LSOAs). All areas in England are then ranked according to their level of deprivation relative to that of other areas, and a higher rank suggests a more deprived situation. The WIMD 2019 and the SIMD 2020 are organised similarly, though some domains of deprivation are named in slightly different ways. While some of those deprivation domains are similar to the constraints used in our microsimulation model (e.g. employment deprivation, education skills and training deprivation), there are no common datasets between the IMD/WIMD/SIMD and the microsimulation. Moreover, many of the deprivation domains are not included in microsimulation (e.g. barriers to housing and services, living environment deprivation, crime). This minimises the risk of circularity when examining relationships. Spearman’s test of rank correlation was used to examine the relationships between the IMD 2019, WIMD 2019, and SIMD 2020 ranks and our simulated income and health estimates for different city regions, with the results shown in Table 10.
All correlations are significant, and the correlations between the IMD/WIMD/SIMD rank and simulated household income and (physical and mental) health summaries are positive. This suggests that individuals living in more deprived areas (with higher IMD/WIMD/SIMD ranks) tend to have lower incomes and worse health conditions; this is as expected32,33,36. For subjective well-being, a higher score means lower well-being. Negative correlations with IMD/WIMD/SIMD ranks suggest lower well-being in more deprived areas, which is in line with previous research (e.g.34,37). These results suggest that household income and health conditions at the small area level are in line with results from the independent IMD data.
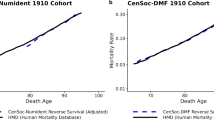
In order to validate the income estimates in our synthetic data we compare results with the 2018 income estimates for small areas (IESA) (https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/earningsandworkinghours/datasets/smallareaincomeestimatesformiddlelayersuperoutputareasenglandandwales) for England and Wales published by ONS (no equivalent is available for Scotland). The 2018 IESA datasets are published at MSOA level and we aggregate the synthetic data outputs for the three English and Welsh cities (Cardiff, Greater Manchester and Sheffield) to match, resulting in 715 MSOAs. We calculate annual net income from monthly net income in our data. The IESA provide a main estimate as well as confidence intervals for each MSOA. Figure 3 provides a summary of this comparison.

Comparison of microsimulation estimates of annual household net income and ONS income estimates at MSOA level.
Red and blue solid lines represent the upper and lower confidence limits of the ONS estimates, while the black dashed line refers to our simulated income estimates. In addition, there is a brown dashed line perpendicular to the x-axis in the diagram (i.e. the “boundary of good fit” line), separating the MSOAs (on the left side of the line) where the simulated estimates fall into the confidence intervals formed by the upper and lower limits of the ONS estimates, from those (on the right side of the line) where the simulated estimates fall out of such intervals. The microsimulation derived income estimates fall within the ONS confidence intervals in 97% of MSOAs assessed (696 out of 715). For the remaining 3% of MSOAs we examined if these areas were spatially correlated with each other, and found that they are randomly distributed within the three city regions without correlations or clustering.
In summary, both the internal and external validations results above suggest that the simulated population has captured well the differences in individuals’ health and income situations at the small area level.
Code availability
The Java based FMF software used to create the synthetic microdata is made available for free under a GNU General Public Licence and can be downloaded from: https://github.com/MassAtLeeds/FMF/releases. The R (version 4.0.3; https://www.r-project.org) code developed for generation, aggregation, and validation of the synthetic microdata are publicly and freely accessible through Figshare28. The script is documented to both explain its purpose and guide the user through its customisation.
References
Harland, K., Heppenstall, A., Smith, D. & Birkin, M. Creating realistic synthetic populations at varying spatial scales: A comparative critique of population synthesis techniques. Journal of Artificial Societies and Social Simulation 15, https://jasss.soc.surrey.ac.uk/15/1/1.html (2012).
Lomax, N. & Smith, A. Microsimulation for demography. Australian Population Studies 1, 73–85, https://doi.org/10.37970/aps.v1i1.14 (2017).
Heppenstall, A. & Smith, D. M. Spatial Microsimulation. In Fischer, M. M. & Nijkamp, P. (eds.) Handbook of Regional Science, 1235–1252, https://doi.org/10.1007/978-3-642-23430-9_65 (Springer, Berlin, Heidelberg, 2014).
Ballas, D. & Clarke, G. GIS and microsimulation for local labour market analysis. Computers, Environment and Urban Systems 24, 305–330, https://doi.org/10.1016/S0198-9715(99)00051-4 (2000).
James, W., Lomax, N. & Birkin, M. Local level estimates of food, drink and tobacco expenditure for Great Britain. Scientific data 6, 1–14, https://www.nature.com/articles/s41597-019-0064-z (2019).
Birkin, M., James, W., Lomax, N. & Smith, A. Data linkage and its applications for planning support systems. In Geertman, S. & Stillwell, J. (eds.) Handbook of Planning Support Science https://doi.org/10.4337/9781788971089.00009 (Edward Elgar Publishing Limited, Cheltenham, 2020).
Clark, S., Birkin, M., Heppenstall, A. & Rees, P. Using 2011 census data to estimate future elderly health care demand. In Stillwell, J. (ed.) The Routledge Handbook of Census Resources, Methods and Applications https://doi.org/10.4324/9781315564777 (Routledge, Oxon, 2018).
Lovelace, R. & Dumont, M. Spatial Microsimulation with R https://www.taylorfrancis.com/books/9781315381640 (Chapman and Hall/CRC, 2016).
Ballas, D. et al. SimBritain: a spatial microsimulation approach to population dynamics. Population, Space and Place 11, 13–34, https://doi.org/10.1002/psp.351 (2005).
Häggström Lundevaller, E., Holm, E., Strömgren, M. & Lindgren, U. Spatial dynamic micro-simulation of demographic development http://urn.kb.se/resolve?urn=urn:nbn:se:umu:diva-16033 (2007).
Smith, D. M., Pearce, J. R. & Harland, K. Can a deterministic spatial microsimulation model provide reliable small-area estimates of health behaviours? An example of smoking prevalence in New Zealand. Health & Place 17, 618–624, https://doi.org/10.1016/j.healthplace.2011.01.001 (2011).
Riva, M. & Smith, D. M. Generating small-area prevalence of psychological distress and alcohol consumption: validation of a spatial microsimulation method. Social Psychiatry and Psychiatric Epidemiology 47, 745–755, https://doi.org/10.1007/s00127-011-0376-6 (2012).
Müller, K. & Axhausen, K. W. Population Synthesis for Microsimulation: State of the Art. https://trid.trb.org/view/1092120 (2011).
Lovelace, R., Ballas, D. & Watson, M. A spatial microsimulation approach for the analysis of commuter patterns: from individual to regional levels. Journal of Transport Geography 34, 282–296, https://doi.org/10.1016/j.jtrangeo.2013.07.008 (2014).
Ballas, D., Clarke, G. P. & Wiemers, E. Spatial microsimulation for rural policy analysis in Ireland: The implications of CAP reforms for the national spatial strategy. Journal of Rural Studies 22, 367–378, https://doi.org/10.1016/j.jrurstud.2006.01.002 (2006).
O’Donoghue, C., Ballas, D., Clarke, G., Hynes, S. & Morrissey, K. Spatial Microsimulation for Rural Policy Analysis. (Springer-Verlag, Berlin Heidelberg, 2013). Advances in Spatial Science.
Ballas, D. Simulating trends in poverty and income inequality on the basis of 1991 and 2001 census data: a tale of two cities. Area 36, 146–163, https://doi.org/10.1111/j.0004-0894.2004.00211.x (2004).
Morrissey, K. & O’Donoghue, C. The Spatial Distribution of Labour Force Participation and Market Earnings at the Sub-National Level in Ireland. Review of Economic Analysis 3, 80–101, https://ideas.repec.org/a/ren/journl/v3y2011i1p80-101.html (2011).
Spooner, F. et al. A dynamic microsimulation model for epidemics. Social Science Medicine 291, https://doi.org/10.1016/j.socscimed.2021.114461 (2021).
Zhou, M., Li, J., Basu, R. & Ferreira, J. Creating spatially-detailed heterogeneous synthetic populations for agent-based microsimulation. Computers, Environment and Urban Systems 91, https://doi.org/10.1016/j.compenvurbsys.2021.101717 (2022).
Vuong, Q. H. et al. Bayesian analysis for social data: A step-by-step protocol and interpretation. MethodsX 7, https://doi.org/10.1016/j.mex.2020.100924 (2020).
Meier, P. et al. The sipher consortium: Introducing the new uk hub for systems science in public health and health economic research. Wellcome open research 4, https://doi.org/10.12688/wellcomeopenres.15534.1 (2019).
O’Donoghue, C., Morrissey, K. & Lennon, J. Spatial Microsimulation Modelling: a Review of Applications and Methodological Choices. International Journal of Microsimulation 7, 26–75, http://hdl.handle.net/10871/19964 (2014).
Lomax, N. & Norman, P. Estimating population attribute values in a table:“get me started in” iterative proportional fitting. The Professional Geographer 68, 451–461, https://doi.org/10.1080/00330124.2015.1099449 (2016).
Tanton, R. A Review of Spatial Microsimulation Methods. International Journal of Microsimulation 7, 4–25, https://microsimulation.pub/articles/00092 (2014).
Ma, J., Heppenstall, A., Harland, K. & Mitchell, G. Synthesising carbon emission for mega-cities: A static spatial microsimulation of transport CO2 from urban travel in Beijing. Computers, Environment and Urban Systems 45, 78–88, https://doi.org/10.1016/j.compenvurbsys.2014.02.006 (2014).
Harland, K. Microsimulation Model User Guide (Flexible Modelling Framework). Working Paper, NCRM https://eprints.ncrm.ac.uk/id/eprint/3177 (2013).
Wu, G., Heppenstall, A., Meier, P., Purshouse, R. & Lomax, N. A synthetic population dataset for estimating small area health and socio-economic outcomes in Great Britain. figshare https://doi.org/10.6084/m9.figshare.c.5443359.v2 (2021).
University of Essex, Institute for Social & Economic Research. Understanding Society: Waves 1–11, 2009–2020 and Harmonised BHPS: Waves 1–18, 1991–2009. [data collection]. 14th Edition. UK Data Service https://doi.org/10.5255/UKDA-SN-6614-15 (2021).
Edwards, K. L. & Tanton, R. Validation of Spatial Microsimulation Models. In Tanton, R. & Edwards, K. (eds.) Spatial Microsimulation: A Reference Guide for Users, Understanding Population Trends and Processes, 249–258, https://doi.org/10.1007/978-94-007-4623-7_15 (Springer Netherlands, Dordrecht, 2012).
Timmins, K. A. & Edwards, K. L. Validation of Spatial Microsimulation Models: a Proposal to Adopt the Bland-Altman Method. International Journal of Microsimulation 9, 106–122 (2016).
Fusco, A., Guio, A.-C. & Marlier, E. Characterising the income poor and the materially deprived in European countries. In Atkinson, A. B. & Marlier, E. (eds.) Income and living conditions in Europe https://statistik.gv.at/web_de/static/income_and_living_conditions_in_europe_072013.pdfpage=135 (Publications Office of the European Union, Luxembourg, 2010).
Graaf, J. P., Ravelli, A. C. J., Haan, M. A. M., Steegers, E. A. P. & Bonsel, G. J. Living in deprived urban districts increases perinatal health inequalities. The Journal of Maternal-Fetal & Neonatal Medicine 26, 473–481, https://doi.org/10.3109/14767058.2012.735722 (2013).
Kearns, A., Whitley, E., Tannahill, C. & Ellaway, A. Loneliness, social relations and health and well-being in deprived communities. Psychology, Health & Medicine 20, 332–344, https://doi.org/10.1080/13548506.2014.940354 (2015).
Fransham, M. Income and Population Dynamics in Deprived Neighbourhoods: Measuring the Poverty Turnover Rate Using Administrative Data. Applied Spatial Analysis and Policy 12, 275–300, https://doi.org/10.1007/s12061-017-9242-6 (2019).
Mireku, M. O. & Rodriguez, A. Family Income Gradients in Adolescent Obesity, Overweight and Adiposity Persist in Extremely Deprived and Extremely Affluent Neighbourhoods but Not in Middle-Class Neighbourhoods: Evidence from the UK Millennium Cohort Study. International Journal of Environmental Research and Public Health 17, 418, https://doi.org/10.3390/ijerph17020418 (2020).
Pedersen, P. V., Grønbæk, M. & Curtis, T. Associations between deprived life circumstances, wellbeing and self-rated health in a socially marginalized population. European Journal of Public Health 22, 647–652, https://doi.org/10.1093/eurpub/ckr128 (2012).
Acknowledgements
This work was supported by the UK Prevention Research Partnership (MR/S037578/1, Meier), which is funded by the British Heart Foundation, Cancer Research UK, Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Health and Social Care Research and Development Division (Welsh Government), Medical Research Council, National Institute for Health Research, Natural Environment Research Council, Public Health Agency (Northern Ireland), The Health Foundation and Wellcome. The authors are also grateful to SIPHER Work Stream 6.1.1 (An Thu Ta, Bert Van Ladegham, and Aki Tsuchiya) for their permission to use their equivalent income estimates in our Case Study, with special thanks to An. Understanding Society is an initiative funded by the Economic and Social Research Council and various Government Departments, with scientific leadership by the Institute for Social and Economic Research, University of Essex, and survey delivery by NatCen Social Research and Kantar Public. The research data are distributed by the UK Data Service.
Author information
Authors and Affiliations
Contributions
G.W. drafted the manuscript, acquired and assembled the raw data, produced the final datasets and technical validation of the synthetic data. A.H. and N.L. aided drafting the manuscript and advised on microsimulation model development. As the principal leads of the SIPHER consortium, P.M. and R.P. secured funds for this research. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver http://creativecommons.org/publicdomain/zero/1.0/ applies to the metadata files associated with this article.
About this article

Cite this article
Wu, G., Heppenstall, A., Meier, P. et al. A synthetic population dataset for estimating small area health and socio-economic outcomes in Great Britain. Sci Data 9, 19 (2022). https://doi.org/10.1038/s41597-022-01124-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41597-022-01124-9
