
Abstract
Chronic granulomatous disease (CGD) is a rare inherited disorder of phagocytic cells1,2. We report the initial results of nine severely affected X-linked CGD (X-CGD) patients who received ex vivo autologous CD34+ hematopoietic stem and progenitor cell-based lentiviral gene therapy following myeloablative conditioning in first-in-human studies (trial registry nos. NCT02234934 and NCT01855685). The primary objectives were to assess the safety and evaluate the efficacy and stability of biochemical and functional reconstitution in the progeny of engrafted cells at 12 months. The secondary objectives included the evaluation of augmented immunity against bacterial and fungal infection, as well as assessment of hematopoietic stem cell transduction and engraftment. Two enrolled patients died within 3 months of treatment from pre-existing comorbidities. At 12 months, six of the seven surviving patients demonstrated stable vector copy numbers (0.4–1.8 copies per neutrophil) and the persistence of 16–46% oxidase-positive neutrophils. There was no molecular evidence of either clonal dysregulation or transgene silencing. Surviving patients have had no new CGD-related infections, and six have been able to discontinue CGD-related antibiotic prophylaxis. The primary objective was met in six of the nine patients at 12 months follow-up, suggesting that autologous gene therapy is a promising approach for CGD patients.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


Data availability
All relevant data are included in the paper. Additional supporting data are available from the corresponding authors on request. All requests for raw and analyzed data and materials will be reviewed by the corresponding authors to verify whether the request is subject to any intellectual property or confidentiality obligations. Patient-related data not included in the paper were generated as part of clinical trials and may be subject to patient confidentiality.
References
Winkelstein, J. A. et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore) 79, 155–169 (2000).
Holland, S. M. Chronic granulomatous disease. Hematol. Oncol. Clin. N. Am. 27, 89–99 (2013).
Gungor, T. et al. Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients with chronic granulomatous disease: a prospective multicentre study. Lancet 383, 436–448 (2014).
Parta, M. et al. Allogeneic reduced-intensity hematopoietic stem cell transplantation for chronic granulomatous disease: a single-center prospective trial. J. Clin. Immunol. 37, 548–558 (2017).
Ott, M. G. et al. Correction of X-linked chronic granulomatous disease by gene therapy, augmented by insertional activation of MDS1-EVI1, PRDM16 or SETBP1. Nat. Med. 12, 401–409 (2006).
Kang, E. M. et al. Retrovirus gene therapy for X-linked chronic granulomatous disease can achieve stable long-term correction of oxidase activity in peripheral blood neutrophils. Blood 115, 783–791 (2010).
Stein, S. et al. Genomic instability and myelodysplasia with monosomy 7 consequent to EVI1 activation after gene therapy for chronic granulomatous disease. Nat. Med. 16, 198–204 (2010).
Santilli, G. et al. Biochemical correction of X-CGD by a novel chimeric promoter regulating high levels of transgene expression in myeloid cells. Mol. Ther. 19, 122–132 (2011).
Brendel, C. et al. Non-clinical efficacy and safety studies on G1XCGD, a lentiviral vector for ex vivo gene therapy of X-linked chronic granulomatous disease. Hum. Gene Ther. Clin. Dev. 29, 69–79 (2018).
Schroder, A. R. et al. HIV-1 integration in the human genome favors active genes and local hotspots. Cell 110, 521–529 (2002).
Berry, C. C. et al. Estimating abundances of retroviral insertion sites from DNA fragment length data. Bioinformatics 28, 755–762 (2012).
Dulamea, A. O. & Lupescu, I. G. Neurological complications of hematopoietic cell transplantation in children and adults. Neural Regen. Res. 13, 945–954 (2018).
Simonis, A. et al. Allogeneic hematopoietic cell transplantation in patients with GATA2 deficiency-a case report and comprehensive review of the literature. Ann. Hematol. 97, 1961–1973 (2018).
Weisser, M. et al. Hyperinflammation in patients with chronic granulomatous disease leads to impairment of hematopoietic stem cell functions. J. Allergy Clin. Immunol. 138, 219–228 e219 (2016).
Grez, M. et al. Gene therapy of chronic granulomatous disease: the engraftment dilemma. Mol. Ther. 19, 28–35 (2011).
Kuhns, D. B. et al. Residual NADPH oxidase and survival in chronic granulomatous disease. N. Engl. J. Med. 363, 2600–2610 (2010).
Dinauer, M. C., Gifford, M. A., Pech, N., Li, L. L. & Emshwiller, P. Variable correction of host defense following gene transfer and bone marrow transplantation in murine X-linked chronic granulomatous disease. Blood 97, 3738–3745 (2001).
Marciano, B. E. et al. X-linked carriers of chronic granulomatous disease: illness, lyonization, and stability. J. Allergy Clin. Immunol. 141, 365–371 (2018).
Ribeil, J. A. et al. Gene therapy in a patient with sickle cell disease. N. Engl. J. Med. 376, 848–855 (2017).
Thompson, A. A. et al. Gene therapy in patients with transfusion-dependent beta-thalassemia. N. Engl. J. Med. 378, 1479–1493 (2018).
Zanta-Boussif, M. A. et al. Validation of a mutated PRE sequence allowing high and sustained transgene expression while abrogating WHV-X protein synthesis: application to the gene therapy of WAS. Gene Ther. 16, 605–619 (2009).
Merten, O. W. et al. Large-scale manufacture and characterization of a lentiviral vector produced for clinical ex vivo gene therapy application. Hum. Gene Ther. 22, 343–356 (2011).
Krueger, F. & Andrews, S. R. Bismark: a flexible aligner and methylation caller for Bisulfite-Seq applications. Bioinformatics 27, 1571–1572 (2011).
Langmead, B. et al. Ultrafast and memory-efficient alignment of short DNA sequences to the human genome. Genome Biol. 10, R25 (2009).
Liu, Y. et al. Bis-SNP: combined DNA methylation and SNP calling for Bisulfite-Seq data. Genome Biol. 13, R61 (2012).
McKenna, A. et al. The genome analysis toolkit: a MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 20, 1297–1303 (2010).
DePristo, M. A. et al. A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat. Genet. 43, 491–498 (2011).
Sherman, E. et al. INSPIIRED: a pipeline for quantitative analysis of sites of new DNA integration in cellular genomes. Mol. Ther. Methods Clin. Dev. 4, 39–49 (2017).
Berry, C. C. et al. INSPIIRED: quantification and visualization tools for analyzing integration site distributions. Mol. Ther. Methods Clin. Dev. 4, 17–26 (2017).
Berry, C. et al. Selection of target sites for mobile DNA integration in the human genome. PLoS Comput. Biol. 2, e157 (2006).
Biasco, L. et al. In vivo tracking of human hematopoiesis reveals patterns of clonal dynamics during early and steady-state reconstitution phases. Cell Stem Cell 19, 107–119 (2016).
Scala, S. et al. Dynamics of genetically engineered hematopoietic stem and progenitor cells after autologous transplantation in humans. Nat. Med. 24, 1683–1690 (2018).
Biasco, L. et al. In vivo tracking of T cells in humans unveils decade-long survival and activity of genetically modified T memory stem cells. Sci. Transl. Med. 7, 273ra213 (2015).
Acknowledgements
The authors thank the patients and families of those included in the study, and members of the Net4GCD consortium (https://www.net4CGD.eu) including: Eurofins Genomics Sequencing Europe, Germany (formerly GATC Biotech AG); F. Mavilio, Genethon, France (currently at the University of Modena, Italy, and at Audentes Therapeutics); J. Schwaeble, University Hospital Frankfurt, Germany; J. Reichenbach, University of Zurich, Switzerland; M. Cavazzana, APHP Necker, Paris, France; S. Blanche, APHP Necker, Paris, France; S. Pouillot, Genosafe, Evry, France (currently at Genethon); K. Kühlcke, Europäisches Institut für Forschung und Entwicklung von Transplantationstrategien GmbH (Eufets), Germany; and M. Schmidt, Deutsches Krebforschungszentrum, Heidelberg, Germany. Editorial support was paid for by Orchard Therapeutics, Boston, MA, USA. This work was supported by research grants from the California Institute of Regenerative Medicine (nos. CLIN2-08231 and FA1-00613-1), the Gene Therapy Resource Program from NHLBI, NIH (no. CRB-SSS-S-15-004351 1840), the NIAID Intramural Program, NET4CGD (FP7 EU grant agreement no. 305011) and the Wellcome Trust (no. 104807/Z/14/Z); by funding from the Department of Medicine (now Department of Pediatrics), Boston Children’s Hospital and the National Institute for Health Research Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust/University College London Hospitals NHS Foundation Trust and University College London, and the French Muscular Dystrophy Association (AFM/Telethon). Clinical-grade vector was manufactured by Genethon BioProd/Yposeksi, Evry, France. Some oxidase activity analyses were funded in whole or in part by federal funds from the National Cancer Institute, NIH, under contract no. HHSN261200800001E. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products or organizations imply endorsement by the United States Government. Support was also provided by the Division of Intramural Research, NIAID, NIH.
Author information
Authors and Affiliations
Consortia
Contributions
The manuscript was written primarily by D.B. Kohn, A.J.T., D.A.W. and H.L.M. VISA analyses were performed by F.D.B., J.G., H.E.R. and J.K.E. M.G. and G.S. helped to construct the initial vector. G.H. and A.G. provided key resources for the conduct of studies, including clinical-grade vector, preclinical data package for CTA, study monitoring and pharmacovigilance and review of the manuscript. A.G. coordinated the Net4CGD consortium. C.B., E.M.K., S.-Y.P., K.L.S., M.A., K.F.B., U.C., S.S.d.R., M.J.D., C.Y.K., D.L.-R., C.R., N.I., K.G., K.S., J.X-B.D., J.D., E.C.M., D.T., L.D.W., C.A.B., T.P., D.B. Kuhns, L.B., P.E.N. and H.B.G. were involved in manufacture of the drug product, delivering the drug to patients for their respective clinics or performing analyses of patient samples. All authors had full access to all data, statistical reports and tables in the study and can take responsibility for the integrity of the data and accuracy of the data analysis. All authors approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
D.B. Kohn, H.L.M., D.A.W. and A.J.T. are Scientific Advisory Board members, and H.B.G. is Chief Scientific Officer for Orchard Therapeutics. H.B.G. is an employee of and equity/stock holder in Orchard Therapeutics. A.J.T. is an equity/stock holder in Orchard Therapeutics. Orchard Therapeutics has obtained an exclusive option to license from Genethon for the rights and know-how related to the lentiviral vector G1XCGD. C.A.B. and T.P. consult for a sequencing service provider, and C.A.B. consults for Novimmune and SOBI. Eurofins Genomics Sequencing Europe (formerly GATC Biotech AG) is a for-profit company (sequencing service provider). The work performed by Eurofins Genomics Sequencing Europe included in the manuscript is provided to the greater scientific community as a fee-for-service product. E.C.M. reports Advisory Board attendance for Orchard Therapeutics. With regard to interests outside of the submitted work, L.D.W. reports grants from the St. Baldrick’s Foundation, Damon-Runyon Cancer Research Foundation and Alex’s Lemonade Stand Foundation, and personal fees from Magenta Therapeutics. A.J.T. reports Board membership and consultancy with Rocket Pharmaceuticals and Generation Bio, and Board membership with 4BIOCapital. S.-Y.P. reports salary support from Boston Children’s Hospital and a grant from NIH. K.L.S. reports personal fees and non-financial support from Orchard Therapeutics. E.M.K., G.S., M.A., K.F.B., U.C., S.S.d.R., M.J.D., C.Y.K., D.L.-R., C.R., N.I., K.G., K.S., J.D., E.C.M., D.B. Kuhns, J.G., H.R., J.K.E., G.H., P.E.N., F.D.B., M.G., J.X.-B.D. and A.G. declare no competing interests.
Additional information
Peer review information Kate Gao was the primary editor on this article and managed its editorial process and peer review in collaboration with the rest of the editorial team.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Schematic representation of the transfer plasmid pCCL_chimGP91_WPRE_Kana.
Cytomegalovirus (CMV) promoter; R, R region of long terminal repeat (LTR); U5, region unique to the 5’ LTR; Psi, encapsidation sequence; RRE, rev responsive element; cPPT, central polypurine tract; CTSG, cathepsin G 5’ minimal flanking regions; FES, human c-fes; coGP91, codon-optimized sequence CYBB gene which is translated into the cytochrome b-245, beta polypeptide; WPRE, mutated Woodchuck hepatitis virus post-transcriptional regulatory element; PPT, HIV-1 polyadenylated region (post-translational); dU3, region unique to the 3’ LTR (U3) of the HIV-1 LTR, in which a 400-bp deletion was introduced to inactivate the HIV-1 enhancer/promoter region; SV40 ori, Simian Virus 40 origin of replication; KANr, kanamycin resistance gene; COLE1, colicin E1 resistance gene.
Extended Data Fig. 2 Cell products and busulfan conditioning.
Panel a shows the final CD34+ cell products (left-axis) obtained for each patient. Panel b shows the VCN per infused cell post-transduction as determined by quantitative PCR. Transduction was also assessed by analyzing the percentage of vector CFUs PCR-positive for GX1CGD vector detected in the final cell product (Panel c). Vertical bars indicate mean and SD. Panel d displays the total net AUC busulfan exposure obtained by the sum of all pharmacokinetic measurements. Target total exposure of 70,000–75,000 ng ml-1 × h is indicated by the shaded area. AUC, area under the curve; CFU, colony-forming unit; PCR, polymerase chain reaction; SD, standard deviation; VCN, vector copy number.
Extended Data Fig. 3 Neutrophil DHR and VCN 24 months post treatment.
Panel a shows the mean (±SEM) of % DHR neutrophils up to 24 months post-treatment, as measured by a dihydrorhodamine oxidation assay. Panel b shows the mean neutrophil VCN (±SEM) up to 24 months post-treatment. DHR, dihydrorhodamine; SEM, standard error of mean; VCN, vector copy number.
Extended Data Fig. 4 X-CGD lineage VCN.
VCN determined by qPCR in multiple-cell lineages for patients surviving >1 month post-GT at each follow-up, showing stable integration of vector into multiple immune cell types. GT, gene therapy; qPCR, quantitative PCR; VCN, vector copy number.
Extended Data Fig. 5 Longitudinal analysis of inferred minimal population sizes.
Longitudinal analysis of minimal population size estimated using the CHAO1 method. The x axis shows time since cell infusion. D0 indicates the pre-infusion product. The y axis shows the numbers of unique integration sites (log scale). Cell types are color coded (bottom). For a few patients a reduced number of cell types were available for analysis. NK, natural killer; PBMC, peripheral blood mononuclear cell.
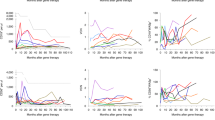
Extended Data Fig. 6 Catalogue of vector integration sites at genes of concern.
Catalogue of cell clones with integration sites within MECOM (MDS/EVI1), PRDM16, and SETBP2. These genes were chosen for analysis because they were targets of integration in expanded cell clones in the first γ-RV-based CGD trial, and were implicated in adverse outcomes. The x axis shows the time point queried, the y axis shows clonal abundance. Cell types queried are color coded (key at the bottom). No cell clones with integration sites near these genes of concern reaches ≥0.3% in abundance, and there is no evidence for longitudinal increases in proportion. CGD, chronic granulomatous disease; γ-RV, gammaretroviral; NK, natural killer; PBMC, peripheral blood mononuclear cell.
Supplementary information
Supplementary Information
Supplementary Tables 1 and 2.
Rights and permissions
About this article

Cite this article
Kohn, D.B., Booth, C., Kang, E.M. et al. Lentiviral gene therapy for X-linked chronic granulomatous disease. Nat Med 26, 200–206 (2020). https://doi.org/10.1038/s41591-019-0735-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-019-0735-5
This article is cited by
-
Successes and challenges in clinical gene therapy
Gene Therapy (2023)
-
Gene therapy for inborn errors of immunity: past, present and future
Nature Reviews Immunology (2023)
-
The transformative potential of HSC gene therapy as a genetic medicine
Gene Therapy (2023)
-
Lentiviral Gene Transfer Corrects Immune Abnormalities in XIAP Deficiency
Journal of Clinical Immunology (2023)
