
Abstract
Whole-body vibration (WBV) and resistive vibration exercise (RVE) are utilized as countermeasures against bone loss, muscle wasting, and physical deconditioning. The safety of the interventions, in terms of the risk of inducing undesired blood clotting and venous thrombosis, is not clear. We therefore performed the present systematic review of the available scientific literature on the issue. The review was conducted following the guidelines by the Space Biomedicine Systematic Review Group, based on Cochrane review guidelines. The relevant context or environment of the studies was “ground-based environment”; space analogs or diseased conditions were not included. The search retrieved 801 studies; 77 articles were selected for further consideration after an initial screening. Thirty-three studies met the inclusion criteria. The main variables related to blood markers involved angiogenic and endothelial factors, fibrinolysis and coagulation markers, cytokine levels, inflammatory and plasma oxidative stress markers. Functional and hemodynamic markers involved blood pressure measurements, systemic vascular resistance, blood flow and microvascular and endothelial functions. The available evidence suggests neutral or potentially positive effects of short- and long-term interventions with WBV and RVE on variables related to blood coagulation, fibrinolysis, inflammatory status, oxidative stress, cardiovascular, microvascular and endothelial functions. No significant warning signs towards an increased risk of undesired clotting and venous thrombosis were identified. If confirmed by further studies, WBV and RVE could be part of the countermeasures aimed at preventing or attenuating the muscular and cardiovascular deconditioning associated with spaceflights, permanence on planetary habitats and ground-based simulations of microgravity.
Similar content being viewed by others
Introduction
Whole-body vibration (WBV) is frequently used as a training and/or rehabilitative approach. This modality has been utilized in subjects or patients who cannot do other forms of exercise, such as children, patients with spinal cord injury, patients with very limited aerobic performance and patients with limited compliance due to physical or behavioral limitations1,2,3. In WBV, mechanical oscillations are transferred to the human body by standing on a vibrating plate. In healthy and patient groups WBV has been shown to obtain varying degrees of improvement of neuromuscular function, bone density, muscle mass, muscle strength, and power4.
Resistive exercise can be combined with WBV. Because of the synergistic effects, this combination appears to offer multiple beneficial advantages such as increased muscle activity and neuromuscular feedback5,6. WBV and resistive vibration exercise (RVE) have been used as countermeasures to prevent the impairments of skeletal muscle function, the loss of muscle mass, muscle force and bone mass described in terrestrial spaceflight analogs, such as bed rest studies7,8,9. Exposure to microgravity and the space environment results in profound multi-system adaptations/impairments, characterized by both short- and long-term changes, including an enhanced coagulation state in the cephalad venous system due to changes in venous flow, jugular vain pressure and endothelial damage10, reductions in maximum oxygen uptake (V̇O2max), impairments of endothelial/microvascular11 and mitochondrial function12 and skeletal muscle oxidative metabolism13,14, reduced muscle size and strength and bone mineral density15. RVE was used in the Berlin Bed Rest studies16,17,18, in which the intervention resulted in beneficial effects on bone loss, bone metabolism, muscle mass loss and muscle contractile capacity. In these studies the effects of RVE on cardiovascular deconditioning were not assessed, and were presumed minor. On the other hand, interesting vascular effects were observed: RVE attenuated the diameter decrease of leg conduit arteries19, prevented completely (carotid artery) or partially (superficial femoral artery) the increase in arterial wall thickness20, and abolished the marked increase in flow-mediated dilation and the decrease in baseline diameter of the superficial femoral artery normally associated with prolonged bed rest21,22.
In terms of safety and side effects of WBV and RVE, apart from reports of itching and erythema23,24, studies are lacking. A potential risk could be related to the development of deep vein thrombosis25, a condition which was recently brought to the attention of the space medicine community following an incidental finding of a persistent asymptomatic obstructive left internal jugular venous thrombus in a single crewmember of the International Space Station26. Whereas WBV and RVE could act, as other types of exercise do, in the direction of favoring vascular health and preventing undesired clotting, the question could be asked whether and how vibration interferes with blood flow and in particular with venous return. Clearly, in the presence of an impediment to flow leading to stagnation or even retrograde flow, then this would constitute a cause for concern. Power doppler ultrasound measurements suggest that vibration at frequencies between 10 and 30 Hz increases blood flow velocity, probably to an extent that is commensurate with the metabolic demand or even above it27. Moreover, near-infrared spectroscopy (NIRS) measurements have demonstrated that vibration extrudes venous blood out of the vibrated muscles during a 30–60-s period28, an effect that seems to be depending on the alignment of the main vibration axis and the vessels with the gravity vector29. When this alignment does not occur, and/or when normal vasomotility is impaired, retrograde and disturbed flow patterns may lead to an increased risk of undesired clotting and venous thrombosis. Venous nd arterial flow patterns during RVE and WVB and the potential link to an increased risk of developing venous thrombosis are largely unexplored.
Another potential question to be considered is the magnitude of stresses and strains that are caused by vibration. A biomechanical study that has assessed 4 Hz vibration-induced contractile element length changes has reported 1% elongation of the muscle-tendon complex length, and that half of the absolute elongation occurred within the muscles30. For comparison, the muscle-tendon complex undergoes elongations in the order of 5% and of 10% during squat jumping and hopping, respectively, which are substantially greater strains than those reported for vibration. Another factor to be considered are shear strains and shear stresses exerted between endothelium and blood. As long as the accelerations stay within the “physiological” range (as e.g., in running), one would expect to see the known physiological endothelial reactions. However, vibration platforms are often used with peak accelerations >10 g, and up to twofold resonant amplitude amplification has been reported in the ankle31, suggesting the potential to elicit endothelial shear stresses that are greater than observed during other types of movement or exercise. From this, a potential risk of damage to the vessel wall and endothelium may arise, possibly leading to inflammation, altered redox balance, increased risk of undesired clotting and venous thrombosis. The issue is largely unexplored.
The present systematic review was therefore performed with the aim of identifying and evaluating the effects of RVE and WBV on blood clotting and thrombosis formation in healthy subjects. If proven to be effective and safe, WBV and RVE could be relevant in the future for space explorations, as they could be implemented during spaceflights and/or inside human habitats during sustained planetary missions, in which the operational constraints will be more severe than on the International Space Station32. As pointed out in the “Gap analysis and research recommendations” section in the review by Harris et al.25, an assessment of the effects of WBV and RVE interventions on the risk of undesired clotting and venous thrombosis during spaceflight and in ground-based analogs is a research gap, which the present systematic literature review seeks to fill.
Methods
Identification and protocol
A systematic review of the literature was conducted following the guidelines defined by the Space Biomedicine Systematic Review Group33 and the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Guidelines for Systematic Review34. Initial pre-scoping was performed to determine appropriate search terms that would capture an adequate number of papers to reach knowledge saturation. The members of the ESA Topical Team on Venous Thromboembolism (VTE) contributed with their expertise to ensure that all appropriate terms were included25,35.
Eligibility criteria
An extensive literature search was performed using recognized life science and biomedical electronic databases and by manually searching reference lists of the articles which specifically investigated the effects of WBV or RVE on blood coagulation and related biomarkers, as well as on related variables such as blood vessels, blood flow and endothelial function. No language, publication date, or publication status restrictions were imposed. This search was applied to the following electronic databases: PubMed, Web of Science, Cochrane. The latest search was performed during April 2022.
The Population, Interest, Control, and Outcome (PICO) table used to define the present research criteria is shown in Table 1, along with the keywords. The population to be studied was chosen as “healthy subjects”; studies on diseased populations or animal studies were excluded. The interventions were subdivided into “short-term” (single session) or “long-term” (more than one session) WBV or RVE. The biomarkers and variables directly or indirectly associated with a risk of undesired clotting and thrombi formation, to be evaluated in the analysis, included: blood levels of nitrites, nitrates, prostacyclin (6-keto), von Willebrand factor, endothelin, hyaluronan, syndecan-1; levels of heparan sulfates, heparanase, endocan, prothrombin fragment, thrombin–antithrombin III complex; glycocalyx integrity; fibrinogen synthase rate, clot formation time, clotting time, extrinsic pathway thromboelastometry, fibrinogen thromboelastometry, international normalized ratio, maximal clot firmness, thromboelastometry. The outcomes to be considered were: molecular, hematological, functional and clinical biomarkers of undesired clotting and thrombi formation; symptoms; evidence from imaging or functional studies related to the presence or the risk of undesired clotting and thrombi formation (see Table 1). The relevant context or environment of the studies to be considered was chosen as “ground-based environment”; space analogs or diseased conditions were not included in this review.
Two members of the project team independently conducted the search strategy (L.Z. and G.B.). Participants of any age and sex were included. All retrieved records were screened by title and abstract by two reviewer authors independently (L.Z. and G.B.). The review authors (L.Z. and G.B.) rated each study using the classifications “relevant”, “irrelevant” or “unsure”. Only retrieved records that received the label “relevant” or “unsure” were full-text screened. Selected articles were then classified into two different categories (i.e., blood markers and functional/haemodynamic outcomes). Disagreements between reviewers were resolved via discussion until a consensus was found and all reasons for exclusion from the study were recorded.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Results
Characteristics of included studies
The systematic search retrieved 801 articles which were screened for duplicates and appropriateness using the Rayyan online platform36. After the initial screening, 77 articles were retained, 33 of which were included in the study. The most common reason for papers to be excluded was that vibrations were applied only on small parts of the body and because of wrong outcomes. The full screening flow is shown below in Fig. 1.

*Papers excluded due to lack of adherence to PICO.
Twenty-five papers were categorized as “short-term intervention” WBV or RVE, and 8 as “long-term intervention” WBV or RVE studies. The characteristics of the studies considered eligible for inclusion are summarized in Tables 2 and 3, respectively. All 33 studies included in this review contained original data and were published in English.
All 25 “short-term intervention” studies were published between 2001 and 2020, and included a total of 348 participants (267 males and 81 females with an age range of 20–55 years). Eleven different vibration platforms were utilized; the most common were Galileo Fitness, Novotech (Pforzheim, Germany) which generates vibration by oscillating along the sagittal axis and the vertical sinusoidal device, Power Plate (International Ltd., London, UK) (all vibration platforms utilized in the included studies are reported in Table 2). The frequency and amplitude (peak-to-peak displacement) of the vibration ranged from 5 to 50 Hz and from 1 to 6 mm, respectively (for more details, see Table 2).
Five studies out of 25 investigated the effects of both WBV and RVE. Whole-body vibration studies (n = 12) exposed the participants to vibrations from 1 to 20 min. RVE studies (n = 18) included isometric and dynamic squats, push-ups, and heel raises with a duration between 30 s and 15 min, or exercise series up to 8 × 60 s (see Table 2). Data of circulating blood markers, functional/hemodynamic markers, and skeletal muscle oxygenation markers were extracted.
The eight “long-term intervention” studies were published between 2013 and 2020 and included a total of 144 participants (97 males and 47 females with an age range of 20–81 years). Five different vibration platforms were utilized. The most commonly utilized instruments were the simultaneous side-alternating whole-body vibration platforms Galileo Fitness, Novotech (Pforzheim, Germany) and the vertical vibration platform, Fitvibe, Gymna Uniphy NV (Bilzen, Belgium). The frequency and amplitude (peak-to-peak displacement) of the vibrations ranged from 20 to 40 Hz and from 2 to 6 mm, respectively (for more details, see Table 3).
No “long-term intervention” study involved WBV alone. The “long-term intervention” studies (n = 8) for RVE involved 2–3 sessions of RVE per week for a duration of 5–12 weeks, and the execution of static or dynamic exercises mainly for the lower body (squats and calf raises), for a total of 2–3 sets for ~8–12 repetitions or 30–60 s of exercise (see Table 3).
Methodological quality of included studies
The studies differed in study design (e.g., age of participants, sex, and type of resistive exercise), mechanical vibration stimulus (e.g., frequency, amplitude, duration of vibration exposure and platform utilized) and measurement intervals. The marked methodological heterogeneity across the studies and the limited number of papers prevented a meta-analysis. Hence, the results are described qualitatively.
Effects of whole-body vibration or resistive vibration exercise on blood markers—short-term interventions
The main variables related to blood markers in both WBV and RVE studies involved angiogenic and endothelial factors, fibrinolysis and coagulation markers, cytokine levels, and plasma oxidative stress markers (see Table 2).
Jawed et al.37 investigated the vascular endothelial growth factor (VEGF) responses after 8 × 60 s in young (i.e., 24 ± 1 years) and old (55 ± 3 years) participants who stood on a vibration platform. An increase in VEGF and in the non-angiogenic circulating stem/progenitor cell (CPC) levels were found in the young participants but not in the elderly, suggesting a selective positive effect on young subjects on the maintenance of vascular health37. The study by Rittweger et al.38, however, did not confirm these findings, reporting no change in VEGF following 3 min of WBV in young participants (29 ± 4 years). However, these negative results may be due to the poor sensitivity of the ELISA kit used in that study. Jawed et al.37 reported an increase in tumor necrosis factor-alpha (TNF-α) which, together with the increases in VEGF, pointed to a pro-angiogenic effect, even if no changes were observed in the angiogenic CPCs and endothelial colony-forming cells following WBV, both in young and old subjects37.
Boyle and Nagelkirik39 reported no changes in plasminogen activator inhibitor (PAI-1) and in tissue plasminogen activator (tPA) levels, suggesting an unchanged fibrinolytic activity following 15 min of WBV.
Cytokine levels were investigated during WBV by Jawed et al.37. Increased levels of anti-inflammatory cytokine (interleukine-10), associated with a decreased level of inflammatory interleukin-6 point toward a reduced inflammatory state37.
WBV significantly increased hemoglobin and platelet counts with no effects on white blood cells, red blood cells, hematocrit, and neutrophil levels37.
As for RVE, the angiogenic and endothelial factors did not show any further benefit compared to resistive exercise alone (not associated with vibrations)40,41. Angiogenic CPCs increased in young participants but not in the elderly during RVE, and not during resistive exercise alone or WBV37. Matrix metalloproteinases (MMPs) have been associated with the release and bioavailability of growth factors and seem to play a role in initiating endothelial cell migration and proliferation as well as in physiological angiogenesis42,43,44. Beijer et al.40, reported no changes in the circulating levels of matrix metalloproteinases −2 (MMP-2) and −9 (MMP-9) when RVE was compared to resistive exercise alone, suggesting that vibration did not have any further angiogenic stimulus when applied during resistive exercise. No change was found in the serum levels of endostatin between RVE and resistive exercise alone40. No change37,38,41 or lower levels40 of VEGF were found when RVE was compared to resistive exercise alone.
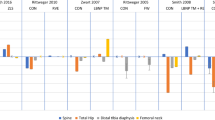
Increases in tPA and decreases in PAI-1 suggested an increased fibrinolytic activity during RVE39. Von Willebrand factor (vWF) was increased after RVE suggesting possible vascular dysfunction45.
A trend for reduced levels of pro-inflammatory interleukin-6 with unchanged values of TNF alpha and interleukin-10 suggests a reduced inflammatory state following RVE; no differences were observed compared to resistive exercise alone37.
RVE increased neutrophil levels, with no effects on hemoglobin, hematocrit, red blood cells, white blood cells, and platelets37.
One study investigated the effects of RVE on oxidative stress markers in 21 females46. RVE resulted in an increased superoxide dismutase antioxidant enzymes activity (SOD) and catalase (CAT), with no effect on thiobarbituric acid reactive substances (TBARS) and iron reduction capacity (FRAP), suggesting an improved antioxidant function46.
Effects of whole-body vibration or resistive vibration exercise on blood markers—long-term interventions
The main variables related to blood markers in “long-term intervention” RVE studies involved, as in short-term intervention studies, angiogenic and endothelial factors, fibrinolysis and coagulation markers and cytokine levels (see Table 3). No long-term WBV studies were found.
Following RVE, circulating levels of MMP-2 were generally elevated after 6-week of training compared to baseline in young healthy and recreationally active participants; both at rest and post-exercise MMP-2 levels were significantly higher compared to resistive exercise alone40. No changes in MMP-9, VEGF or in endothelial cell proliferation were observed after both exercise and vibration interventions40. Circulating post-exercise endostatin levels were higher only after intervention with resistive exercise (no vibrations involved)40. Therefore, it seems that superimposing a vibration stimulus to resistance exercise might not be beneficial for triggering angiogenic-inducing signaling pathways in skeletal muscle40.
Five weeks of a high-amplitude (4 mm) vibration training program caused an increase in tPA and a decrease in PAI-147. Fibrinogen and plasminogen levels showed a decrease, albeit not significant47. Low-amplitude vibration training showed an increase in tPA. PAI‑1, fibrinogen and plasminogen slightly decreased, but did not change significantly47. No differences between groups (high- vs. low-amplitude vibration) in tPA, PAI‑1, plasminogen, and fibrinogen were observed47. These results suggest that resistive vibration training positively affects fibrinolytic activity.
Although vWF was increased after short-term intervention RVE, it significantly decreased after 8 weeks of training, suggesting a beneficial effect of RVE training on vascular function in a previously untrained population45.
Nine weeks of training with RVE did not alter inflammatory markers (i.e., levels of C-reactive protein, IL-6, IL-1β, TNF-α, and IL-10) in healthy older adults48. Rodriguez-Miguelez et al.49 reported an improved anti-inflammatory status in elderly subjects after a 8-week RVE training program. More specifically, a reduced mRNA and protein levels of markers involved in the toll-like receptors (TLR2/TLR4) myeloid differentiation primary response gene 88 (MyD88) and TIR domain-containing adaptor-inducing interferon (TRIF)-dependent pathways were reported. Also, plasma concentration of pro-inflammatory C-reactive protein and TNF-α decreased after training, whereas anti-inflammatory cytokine IL-10 were upregulated49.
Effects of whole-body vibration and resistive vibration exercise on functional/hemodynamic markers—short-term interventions
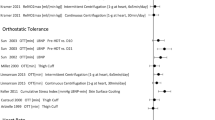
Functional and hemodynamic markers mostly involved blood pressure measurements, systemic vascular resistance, blood flow and arterial stiffness measurements (see Table 2). Heterogeneous results have been reported for blood pressure values during WBV. Dipla et al.50 observed an increase in systolic and diastolic blood pressure with WBV, as well as a decrease in systemic vascular resistance in premenopausal women (age: 37 ± 1.5 years)50. On the contrary, Jawed et al.37, Hazell et al.23, and Yarar-Fisher et al.51 did not find any change in blood pressure.
Blood flow changes were mostly assessed by eco-doppler in the femoral artery and in the popliteal artery (see Table 2). Betik et al.52 investigated the blood flow changes in the femoral artery in response to different vibration frequencies (i.e., 5–7.5–10–12–15 Hz). They observed an increase in blood flow by about fourfold, and the greatest increase was achieved with 12.5 Hz. The increase in blood flow following WBV was also confirmed by Menendez et al.53, who observed an increase in peak blood velocity in the popliteal artery. On the contrary, Hazell et al.23 did not see any changes in the common femoral artery during 15 × 60 s of WBV. Skeletal muscle oxygenation was mainly evaluated by NIRS. An increase in total hemoglobin was observed during WBV, suggesting vasodilatation51,54.
As for RVE, blood pressure measurements, systemic vascular resistance, blood flow and arterial stiffness measurements have been assessed (see Table 2). Blood pressure has been reported to be unchanged in RVE vs. baseline conditions27,55,56 and increased23. A reduced systemic vascular function (i.e., capacitive [for large artery] and oscillatory [for small artery] arterial compliance) and arterial stiffness have been reported following RVE55,57. There is a general agreement among studies indicating an increased blood flow during RVE. An increased blood flow was observed in the femoral23,27 and popliteal arteries53,56, as well as in muscular blood flow in the calf and thigh56. No changes in total hemoglobin (determined by NIRS) have been reported during RVE38,58,59 in vastus lateralis and in gastrocnemius. In contrast, Yamada et al.58 and Coza et al.60 observed an increase in total hemoglobin during RVE.
Effects of whole-body vibration and resistive vibration exercise on functional/hemodynamic markers—long-term interventions
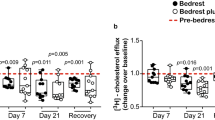
Six weeks of training with RVE determined positive effects on vascular function, as shown by a larger reactive hyperemia (greater increase in total hemoglobin [tHb] evaluated by NIRS over baseline in the recovery period after a set of calf raises) and an increased blood volume (larger absolute tHb value at baseline and both during and after exercise) compared to resistance exercise alone61. In healthy postmenopausal women (64 ± 1 years), both RVE and resistive exercise induced similar improvements in brachial artery (BA) endothelial function (i.e., increased FMD) after 12 weeks of training62. On the other hand, Weber et al.63 did not find any changes in FMD after both interventions (RVE and resistive exercise) in any of the investigated arteries (i.e., superficial femoral artery [SFA], BA and carotid arteries [CA]) in young healthy subjects following 6 weeks of training.
Some positive structural adaptations were found after vibration training. Beijer et al.61 reported an increased number of capillaries around fibers in the soleus muscle after 6 weeks of both RVE and resistive exercise in recreationally active and young men. Moreover, an increased SFA resting diameter and a reduced arterial wall thickness in CA were described after 6 weeks of resistive exercise, with and without vibration63.
Improvements in indices of wave reflection and cardiac pulsatile load (i.e., increased pulse pressure amplification, reduced augmentation index and augmented pressure) were also reported in healthy postmenopausal and normal weight women after 12-week RVE training program, but not after only resistive exercise intervention alone62. Therefore, RVE training may have a greater benefit in preventing cardiovascular events compared to resistive exercise alone.
Discussion
The safety of WBV and RVE, in terms of the risk of inducing undesired blood clotting and venous thrombosis, is not clear. We therefore performed the present systematic review of the available scientific literature on the issue. The limited available evidence suggests neutral or potentially positive effects of short- and long-term interventions with WBV and RVE on variables related to blood coagulation, fibrinolysis, inflammatory status, oxidative stress, cardiovascular, microvascular, and endothelial functions. No significant warning signs towards an increased risk of undesired clotting and venous thrombosis deriving from WBV or RVE were identified.
In total, 33 studies that investigated the effects WBV and RVE on both clotting and thrombosis formation in healthy participants were included. Two broad categories of biomarkers were identified, which were circulating blood and functional/hemodynamic markers. All studies were grouped under these two classifications and further subdivided into short- and long-term interventions.
As mentioned above, the marked methodological heterogeneity across the selected studies and the limited (very limited for several aspects) number of available studies prevented a formal meta-analysis of studies. In particular frequency, amplitude and movement principle were found to be very heterogeneous between the included studies (see Tables 2 and 3). Since the effects of WBV and RVE are strongly dependent upon the parameters that characterize mechanical vibration, such as the frequency and amplitude of the vibration as well as the duration of vibration exposure27,64 the results are described in qualitative terms, and they are intrinsically associated with a significant degree of uncertainty. Overall, the analysis stresses the need for further research on the topic.
Data on coagulation factors following short-term intervention WBV or RVE are very scarce. Only one study45 observed increased levels of von Willebrand factor after RVE, suggesting a possible vascular dysfunction. In the same study, however, levels of the von Willebrand factor significantly decreased after eight weeks of RVE training. If present, therefore, negative effects of RVE on blood coagulation factors were only transitory, and a positive effect may be present following long-term exposure. These results are in agreement with studies which show an increased risk of thrombotic events after acute exercise, particularly in sedentary individuals, but a decreased risk after regular physical activity65. Fibrinolytic activity was unchanged following short-term exposure to WBV39, whereas long-term exposure47 RVE increased fibrinolytic activity.
Overall, it can be concluded that the few studies available do not suggest the presence of an increased risk of blood coagulation, or of impairments of fibrinolytic activity in subjects exposed to WBV or RVE. Actually, short- or long-term intervention with RVE may exert positive effects on these functions.
In terms of angiogenesis and endothelial function, conflicting results37,38 are present in the literature as far as VEGF and CPC levels following short-term exposure to WBV. On the other hand, short-term RVE had positive effects on these factors, although not greater than those obtained with resistive exercise alone (not associated with vibrations)40,41. An exception might be represented by MMPs, molecules considered to be essential for extracellular matrix degradation and physiological angiogenesis, for which higher values following long-term intervention with RVE were observed compared to those described following resistive exercise alone40.
Studies dealing with cytokine levels concur in indicating a reduced inflammatory state following short-term intervention WBV (see e.g., 37). Following short-term RVE the positive effects on the inflammatory state were not greater compared to those obtainable with resistive exercise alone37. Unchanged48 or improved49 inflammatory markers were described following long-term RVE interventions. Considering the pivotal role played by inflammation in promoting undesired coagulation, the effects of WBV and RVE on the latter seem to be either neutral or positive. The same concept could be applied to antioxidant function, which was found to be improved following short-term exposure to RVE46.
Increases in blood flow during short-term intervention WBV52,53 or RVE have been described. By preventing blood stasis, slow, stagnant or retrograde blood flow and by enhancing shear stress, increases in blood flow may favor the prevention of undesired coagulation and thrombus formation.
Conflicting results have been described in terms of flow-mediated vasodilation and endothelial function following long-term RVE interventions: improvements62 or no significant changes63 have been reported. In any case, no study observed impairments of flow-mediated vasodilation or endothelial dysfunction following WBV or RVE. An improved reactive hyperemia (index of microvascular function) was observed by Beijer et al.61 by NIRS. The same authors described an increased number of capillaries around muscle fibers following long-term RVE intervention, as well as higher levels of total (oxygenated + deoxygenated) hemoglobin in skeletal muscle, determined by NIRS at rest, during and after exercise61. Other indices of cardiovascular function were observed to be improved following RVE, also in comparison with resistive exercise alone, such as an increased resting diameter and reduced arterial wall thickness63, improvements of indices of pulse wave reflection and cardiac pulsatile load62.
This current review identifies the need for further studies dedicated to investigating the effects of WBV and RVE on both clotting and thrombosis formation in healthy participants. Precisely, controlled, reproducible studies should be adopted in the future, incorporating larger sample sizes (e.g., different age of participants and different sex), with a standardization of protocol designs and data analysis. A major limitation of the present review is indeed represented by the pronounced methodological heterogeneity across studies in terms of mechanical vibration stimulus (e.g., frequency, amplitude, duration of vibration exposure and platform utilized) and measurement intervals. Future studies should also clearly consider safety issues and adverse events.
Further studies on high-risk populations, during bed rest or in long-term analogs, and eventually in-flight assessments are needed. If confirmed to be safe and effective in these conditions, WBV and RVE could be considered in the training and rehabilitation interventions to be performed in at-risk populations or in special conditions, or with the aim of preventing or attenuating the muscular and cardiovascular deconditioning associated with spaceflights, permanence on planetary habitats and ground-based simulations of microgravity. As for other types of exercise, WBV and RVE could help preventing muscle atrophy and sarcopenia, increase the muscle pump effect, induce shear stress, improve endothelial function, prevent venous stasis, inappropriate aggregation and coagulation. An obvious advantage would be represented by the fact that these interventions could be implemented reasonably easily during spaceflights and/or permanence on planetary habitats.
In summary, within the substantial limitations described above, the available evidence identified by the present systematic review suggests neutral or potentially positive effects of short- and long-term intervention with WBV and RVE on variables related to blood coagulation, fibrinolysis, inflammatory status, oxidative stress, cardiovascular, microvascular and endothelial functions. No significant warning signs towards an increased risk of undesired coagulation and venous thrombosis were identified. Although it is not possible at this stage to derive firm recommendations from the existing knowledge, mainly due to the lack of coherence in end-points across studies, the lack of any reported clotting events, despite therapeutic and leisure applications of vibration in many countries worldwide, provides some confidence.
Data availability
All relevant data are presented in the manuscript. Data not shown are available from the corresponding author upon request.
References
Tubic, B. et al. Randomised study of children with obesity showed that whole body vibration reduced sclerostin. Acta Paediatr. 108, 502–513 (2019).
Stark, C. et al. Vibration-assisted home training program for children with spinal muscular atrophy. Child Neurol. Open. 5, 2329048X18780477 (2018).
Furness, T., Joseph, C., Naughton, G., Welsh, L. & Lorenzen, C. Benefits of whole-body vibration to people with COPD: a community-based efficacy trial. BMC Pulm. Med. 14, 38 (2014).
Rittweger, J. Vibration as an exercise modality: how it may work, and what its potential might be. Eur. J. Appl. Physiol. 108, 877–904 (2010).
Rittweger, J. Manual of Vibration Exercise and Vibration Therapy, no. 181165 (Springer, 2020).
Hazell, T. J., Jakobi, J. M. & Kenno, K. A. The effects of whole-body vibration on upper- and lower-body EMG during static and dynamic contractions. Appl. Physiol. Nutr. Metab. 32, 1156–1163 (2007).
Ogawa, M. et al. Effects of 8 weeks of bed rest with or without resistance exercise intervention on the volume of the muscle tissue and the adipose tissues of the thigh. Physiol. Rep. 8, e14560 (2020).
Belavý, D. L. et al. Resistive vibration exercise during bed-rest reduces motor control changes in the lumbo-pelvic musculature. J. Electromyogr. Kinesiol. 22, 21–30 (2012).
Blottner, D. et al. Human skeletal muscle structure and function preserved by vibration muscle exercise following 55 days of bed rest. Eur. J. Appl. Physiol. 97, 261–271 (2006).
Kim, D. S. et al. The effect of microgravity on the human venous system and blood coagulation: a systematic review. Exp. Physiol. 106, 1149–1158 (2021).
Zuccarelli, L. et al. Peripheral impairments of oxidative metabolism after a 10-day bed rest are upstream of mitochondrial respiration. J. Physiol. 599, 4813–4829 (2021).
Salvadego, D. et al. PlanHab∗: hypoxia does not worsen the impairment of skeletal muscle oxidative function induced by bed rest alone. J. Physiol. 596, 3341–3355 (2018).
Baldassarre, G. et al. Decrease in work rate in order to keep a constant heart rate: biomarker of exercise intolerance following a 10-day bed rest. J. Appl. Physiol. 132, 1569–1579 (2022).
Porcelli, S. et al. Role of skeletal muscles impairment and brain oxygenation in limiting oxidative metabolism during exercise after bed rest. J. Appl. Physiol. 109, 101–111 (2010).
Demontis, G. C. et al. Human pathophysiological adaptations to the space environment. Front. Physiol. 8, 547 (2017).
Belavý, D. L., Gast, U. & Felsenberg, D. Exercise and Transversus Abdominis Muscle Atrophy after 60-d Bed Rest. Med. Sci. Sports Exerc. 49, 238–246 (2017).
Miokovic, T. et al. Muscle atrophy, pain, and damage in bed rest reduced by resistive (vibration) exercise. Med. Sci. Sports Exerc. 46, 1506–1516 (2014).
Armbrecht, G. et al. Resistive vibration exercise attenuates bone and muscle atrophy in 56 days of bed rest: biochemical markers of bone metabolism. Osteoporos. Int. 21, 597–607 (2010).
Bleeker, M. W. et al. Vascular adaptation to deconditioning and the effect of an exercise countermeasure: results of the Berlin Bed Rest study. J. Appl. Physiol. 99, 1293–1300 (2005).
van Duijnhoven, N. T. et al. Impact of bed rest on conduit artery remodeling: effect of exercise countermeasures. Hypertension 56, 240–246 (2010).
van Duijnhoven, N. T. et al. Resistive exercise versus resistive vibration exercise to counteract vascular adaptations to bed rest. J. Appl. Physiol. 108, 28–33 (2010).
Hu, R., Wang, W. Q., Lau, C. P. & Tse, H. F. Gender differences on brachial flow-mediated dilation and carotid intima-media thickness for prediction of spontaneous cardiovascular events. Clin. Cardiol. 31, 525–530 (2008).
Hazell, T. J., Thomas, G. W., Deguire, J. R. & Lemon, P. W. Vertical whole-body vibration does not increase cardiovascular stress to static semi-squat exercise. Eur. J. Appl. Physiol. 104, 903–908 (2008).
Rittweger, J., Beller, G. & Felsenberg, D. Acute physiological effects of exhaustive whole-body vibration exercise in man. Clin. Physiol. 20, 134–142 (2000).
Harris, K. et al. Pathophysiology, risk, diagnosis, and management of venous thrombosis in space: where are we now? NPJ Microgravity 9, 17 (2023).
Marshall-Goebel, K. et al. Assessment of jugular venous blood flow stasis and thrombosis during spaceflight. JAMA Netw. Open 2, e1915011 (2019).
Lythgo, N., Eser, P., de Groot, P. & Galea, M. Whole-body vibration dosage alters leg blood flow. Clin. Physiol. Funct. Imaging 29, 53–59 (2009).
Zange, J. et al. In the unloaded lower leg, vibration extrudes venous blood out of the calf muscles probably by direct acceleration and without arterial vasodilation. Eur. J. Appl. Physiol. 114, 1005–1012 (2014).
Çakar, H. I. et al. Vibration-related extrusion of capillary blood from the calf musculature depends upon directions of vibration of the leg and of the gravity vector. Eur. J. Appl. Physiol. 117, 1107–1117 (2017).
Cochrane, D. J., Loram, I. D., Stannard, S. R. & Rittweger, J. Changes in joint angle, muscle-tendon complex length, muscle contractile tissue displacement, and modulation of EMG activity during acute whole-body vibration. Muscle Nerve 40, 420–429 (2009).
Bressel, E., Smith, G. & Branscomb, J. Transmission of whole body vibration in children while standing. Clin. Biomech. 25, 181–186 (2010).
Scott, J. P. R., Weber, T. & Green, D. A. Introduction to the frontiers research topic: optimization of exercise countermeasures for human space flight—lessons from terrestrial physiology and operational considerations. Front. Physiol. 10, 173 (2019).
Winnard, A. et al. Developing, implementing, and applying novel techniques during systematic reviews of primary space medicine data. Aerosp. Med. Hum. Perform. 92, 681–688 (2021).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. BMJ 339, b2700 (2009).
Harris, K. et al. Search for venous endothelial biomarkers heralding venous thromboembolism in space: a qualitative systematic review of terrestrial studies. Front. Physiol. 13, 885183 (2022).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5, 210 (2016).
Jawed, Y., Beli, E., March, K., Kaleth, A. & Loghmani, M. T. Whole-body vibration training increases stem/progenitor cell circulation levels and may attenuate inflammation. Mil. Med. 185, 404–412 (2020).
Rittweger, J., Moss, A. D., Colier, W., Stewart, C. & Degens, H. Muscle tissue oxygenation and VEGF in VO-matched vibration and squatting exercise. Clin. Physiol. Funct. Imaging 30, 269–278 (2010).
Boyle, L. J. & Nagelkirk, P. R. The effects of whole body vibration and exercise on fibrinolysis in men. Eur. J. Appl. Physiol. 110, 1057–1061 (2010).
Beijer, Å. et al. Whole-body vibrations do not elevate the angiogenic stimulus when applied during resistance exercise. PLoS ONE 8, e8014 (2013).
Chih-Min, W., Wen-Chyuan, C. & Zong-Yan, C. Effect of acute whole-body vibration exercise with blood flow restriction on vascular endothelial growth factor response. Kinesiology50. 2, 149–156 (2018).
Schnaper, H. W. et al. Type IV collagenase(s) and TIMPs modulate endothelial cell morphogenesis in vitro. J. Cell Physiol. 156, 235–246 (1993).
Fowlkes, J. L., Thrailkill, K. M., Serra, D. M., Suzuki, K. & Nagase, H. Matrix metalloproteinases as insulin-like growth factor binding protein-degrading proteinases. Prog. Growth Factor Res. 6, 255–263 (1995).
Coppock, H. A., White, A., Aplin, J. D. & Westwood, M. Matrix metalloprotease-3 and -9 proteolyze insulin-like growth factor-binding protein-1. Biol. Reprod. 71, 438–443 (2004).
Tsung-Cheng, L. & Zong-Yan, C. The effects of whole body vibration training combined with blood flow restriction on von Willebrand factor response. Isokinet. Exerc. Sci. 28, 27–33 (2020).
Santos, J. M. et al. Does whole body vibration exercise improve oxidative stress markers in women with fibromyalgia? Braz. J. Med. Biol. Res. 52, e8688 (2019).
Ghazalian, F., Hakemi, L., Pourkazemi, L. & Akhoond, M. Effects of whole-body vibration training on fibrinolytic and coagulative factors in healthy young men. J. Res. Med. Sci. 19, 982–986 (2014).
Cristi, C., Collado, P. S., Márquez, S., Garatachea, N. & Cuevas, M. J. Whole-body vibration training increases physical fitness measures without alteration of inflammatory markers in older adults. Eur. J. Sport Sci. 14, 611–619 (2014).
Rodriguez-Miguelez, P. et al. Whole-body vibration improves the anti-inflammatory status in elderly subjects through toll-like receptor 2 and 4 signaling pathways. Mech. Ageing Dev. 150, 12–19 (2015).
Dipla, K. et al. Exaggerated haemodynamic and neural responses to involuntary contractions induced by whole-body vibration in normotensive obese versus lean women. Exp. Physiol. 101, 717–730 (2016).
Yarar-Fisher, C. et al. Acute physiological effects of whole body vibration (WBV) on central hemodynamics, muscle oxygenation and oxygen consumption in individuals with chronic spinal cord injury. Disabil. Rehabil. 36, 136–145 (2014).
Betik, A. C., Parker, L., Kaur, G., Wadley, G. D. & Keske, M. A. Whole-body vibration stimulates microvascular blood flow in skeletal muscle. Med. Sci. Sports Exerc. 53, 375–383 (2021).
Menéndez, H. et al. Influence of isolated or simultaneous application of electromyostimulation and vibration on leg blood flow. Eur. J. Appl. Physiol. 115, 1747–1755 (2015).
Games, K. E. & Sefton, J. M. Whole-body vibration influences lower extremity circulatory and neurological function. Scand. J. Med. Sci. Sports 23, 516–523 (2013).
Otsuki, T. et al. Arterial stiffness acutely decreases after whole-body vibration in humans. Acta Physiol. 194, 189–194 (2008).
Kerschan-Schindl, K. et al. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 21, 377–382 (2001).
Karabulut, U., Karabulut, M. & James, E. G. Small arteries stay stiff for a longer period following vibration exercises in combination with blood flow restriction. Clin. Physiol. Funct. Imaging 38, 1000–1007 (2018).
Yamada, E. et al. Vastus lateralis oxygenation and blood volume measured by near-infrared spectroscopy during whole body vibration. Clin. Physiol. Funct. Imaging 25, 203–208 (2005).
Cardinale, M., Ferrari, M. & Quaresima, V. Gastrocnemius medialis and vastus lateralis oxygenation during whole-body vibration exercise. Med. Sci. Sports Exerc. 39, 694–700 (2007).
Coza, A., Nigg, B. M. & Dunn, J. F. Effects of vibrations on gastrocnemius medialis tissue oxygenation. Med. Sci. Sports Exerc. 43, 509–515 (2011).
Beijer, Å. et al. Microcirculation of skeletal muscle adapts differently to a resistive exercise intervention with and without superimposed whole-body vibrations. Clin. Physiol. Funct. Imaging 35, 425–435 (2015).
Jaime, S. J., Maharaj, A., Alvarez-Alvarado, S. & Figueroa, A. Impact of low-intensity resistance and whole-body vibration training on aortic hemodynamics and vascular function in postmenopausal women. Hypertens. Res. 42, 1979–1988 (2019).
Weber, T. et al. Vascular adaptations induced by 6 weeks WBV resistance exercise training. Clin. Physiol. Funct. Imaging 33, 92–100 (2013).
Zaidell, L. N. et al. Lower body acceleration and muscular responses to rotational and vertical whole-body vibration at different frequencies and amplitudes. Dose Response 17, 1559325818819946 (2019).
Olsen, L. N., Fischer, M., Evans, P. A., Gliemann, L. & Hellsten, Y. Does exercise influence the susceptibility to arterial thrombosis? An integrative perspective. Front. Physiol. 12, 636027 (2021).
Robbins, D., Yoganathan, P. & Goss-Sampson, M. The influence of whole body vibration on the central and peripheral cardiovascular system. Clin. Physiol. Funct. Imaging 34, 364–369 (2014).
Li, Z. et al. Wavelet analysis of lumbar muscle oxygenation signals during whole-body vibration: implications for the development of localized muscle fatigue. Eur. J. Appl. Physiol. 112, 3109–3117 (2012).
Robbins, D., Elwell, C., Jimenez, A. & Goss-Sampson, M. Localised muscle tissue oxygenation during dynamic exercise with whole body vibration. J. Sports Sci. Med. 11, 346–351 (2012).
Sanchez-Gonzalez, M. A. et al. Impact of passive vibration on pressure pulse wave characteristics. J. Hum. Hypertens. 26, 610–615 (2012).
Yue, Z. & Mester, J. On the cardiovascular effects of whole‐body vibration part I. Longitudinal effects: hydrodynamic analysis. Stud. Appl. Math. 119, 95–109 (2007).
Acknowledgements
The European Space Agency provided funding to cover the open-access cost of this publication. Publication costs were covered specifically from the ESA-sponsored Topical Team on “Pathophysiology, risk and clinical presentation of venous thromboembolism (VTE) and its evaluation of its prevention, diagnosis, mitigation, and management strategies in spaceflight” (Grant number 4000131108/20/NL/PG/pt).
Author information
Authors and Affiliations
Contributions
N.G., T.W., D.A.G., and B.G. conceived the study and obtained the financial support. Data collection and analysis were completed by L.Z. and G.B. L.Z., G.B., A.W., K.M.H., T.W., D.A.V., L.G.P., T.H.K., L.R., D.S.K., D.K.G., R.A., J.M.L., A.E., J.R., B.G., and N.G. interpreted the results. The creation of figures was completed by L.Z. and G.B. L.Z., G.B., and B.G. wrote the article and the final draft was edited by A.W., K.M.H., T.W., D.A.V., L.G.P., T.H.K., L.R., D.S.K., D.K.G., R.A., J.M.L., A.E., J.R., and N.G. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zuccarelli, L., Baldassarre, G., Winnard, A. et al. Effects of whole-body vibration or resistive-vibration exercise on blood clotting and related biomarkers: a systematic review. npj Microgravity 9, 87 (2023). https://doi.org/10.1038/s41526-023-00338-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41526-023-00338-4
