
Abstract
The effectiveness of inactivated vaccines (VE) against symptomatic and severe COVID-19 caused by omicron is unknown. We conducted a nationwide, test-negative, case-control study to estimate VE for homologous and heterologous (BNT162b2) booster doses in adults who received two doses of CoronaVac in Brazil in the Omicron context. Analyzing 1,386,544 matched-pairs, VE against symptomatic disease was 8.6% (95% CI, 5.6–11.5) and 56.8% (95% CI, 56.3–57.3) in the period 8–59 days after receiving a homologous and heterologous booster, respectively. During the same interval, VE against severe Covid-19 was 73.6% (95% CI, 63.9–80.7) and 86.0% (95% CI, 84.5–87.4) after receiving a homologous and heterologous booster, respectively. Waning against severe Covid-19 after 120 days was only observed after a homologous booster. Heterologous booster might be preferable to individuals with completed primary series inactivated vaccine.
Similar content being viewed by others
Introduction
The substantial initial protection of primary series Covid-19 vaccines against moderate and severe Covid-19 has been demonstrated through randomized clinical trials and observational studies1,2,3. Since then, accumulating evidence has demonstrated the importance of waning protection following primary series completion4,5,6, and decreased effectiveness of current vaccines to variants of concern (VoC), in particular the Omicron (B.1.1.529) variant4,7. Delineating the effectiveness of the range of booster vaccination strategies is therefore critical for guiding national and global policy8.
The majority of the existing vaccine effectiveness evidence is for mRNA vaccines and adenoviral vectored vaccines, both as the primary series and as booster doses7,9,10, leaving significant evidence gaps regarding inactivated vaccine products. Inactivated vaccines are widely used, particularly in low- and middle-income countries, and represent half of the administered doses of Covid-19 vaccines worldwide as of Jan 202211. Large Omicron epidemics associated with severe cases and deaths have occurred in regions, most recently Eastern Asia, where inactivated vaccines have been extensively administered12. Brazil initiated booster vaccination in September 2021, after Delta VoC began to dominate in the country and three months before Omicron dominance5. Evidence concerning the effectiveness of inactivated vaccines with homologous or heterologous boosters is critically needed to inform vaccine policies in countries that used these vaccines in their initial rollout.
We evaluated the vaccine effectiveness of CoronaVac and BNT162b2 booster doses among Brazilian adults who completed the primary series of the CoronaVac vaccine in a nationwide test-negative case-control study. Our primary analysis focused on the period from December 25, 2021 to April 22, 2022, when circulation of the Omicron variant was predominant, and compared these findings with those from the prior period, from September 6, 2021, to December 14, 2021, when the Delta variant was predominant in the country.
Results
Descriptive Characteristics
During the study period, there was a low incidence of Covid-19 cases and hospital admissions or deaths during the Delta wave compared to earlier periods in Brazil, until the end of December 2021, which corresponded to the introduction and spread of the Omicron variant (Fig. 1). During Omicron period, 97.3% of samples were BA.1 (97.3%) followed by BA.2 (2.7%) according to the GISAID data. Across all age groups in Brazil, on April 22, 2022, coverage was 83.7% for the first vaccine dose, 77.1% for second doses, and 40.7% for boosters (Fig. 1).

Daily prevalence of SARS-CoV-2 variants among genotyped isolates were obtained from the GISAID (global initiative on sharing avian influenza data) database (extraction on 09 May 2022), selecting samples from Brazil. Green represents Delta prevalence, pink area represents Omicron prevalence and grey area represents others. Second dose coverage includes a single dose of Ad26.COV2.S. MA—moving averages.
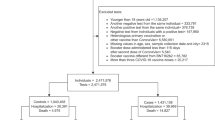
After applying the inclusion and exclusion criteria, there were 3,548,209 RT-PCR/antigen tests from 3,320,429 individuals eligible for matching for the primary analysis. After matching one control per case, with replacement, the analysis population was 3,094,478 RT-PCR/antigen tests from 2,107,696 individuals for the primary analysis (Supplementary Fig. 2). Controls were matched to multiple cases a mean 2.7 ± 4, the median of 2 (IQR: 1-3) times. The characteristics for the selected case-control sets for the main analysis during the Delta and Omicron periods is shown in Table 1. Among severe Covid-19, 88% (54,307/61,647) of patients had at least one sign/symptom of respiratory distress (dyspnoea, hypoxaemia, respiratory discomfort); 77% (46,739/60,919) of patients received either non-invasive or invasive mechanical ventilation. During the omicron period, these numbers were 87% (36,702/42,195) and 75% (31,151/41,714) respectively. The characteristics of those who received an homologous or heterologous booster are shown on Supplementary Table 2.
Vaccine effectiveness estimates
Unadjusted vaccine effectiveness estimates for two doses of CoronaVac, and for a booster dose of CoronaVac and BNT162b2, are displayed in Supplementary Table 3. Adjusted vaccine effectiveness estimates for two doses of CoronaVac, and for a booster dose of CoronaVac and BNT162b2, are displayed in Fig. 2 and in Supplementary Table 4. Relative to the Delta period, the Omicron period was associated with a substantial decrease in vaccine effectiveness against symptomatic disease for the primary series of CoronaVac (VE ≥ 180 days after second dose 34.0%, 95% CI 32.3 to 35.7; in the Delta period; compared to 6.3%, 95% CI 5.3 to 7.3, during the Omicron period). During the Omicron period, vaccine effectiveness 8-59 days after a homologous booster was 8.6% (95% CI, 5.6 to 11.5) against symptomatic Covid-19 and 73.6% (95% CI, 63.9 to 80.7) against severe Covid-19 and for a BNT162b2 booster, vaccine effectiveness was 56.8% (95% CI, 56.3 to 57.3) against symptomatic and 86.0% (95% CI, 84.5 to 87.4) against severe Covid-19.

a against symptomatic Covid-19 (n = 321,390 for Delta predominance period and n = 2,773,088 for Omicron predominance period). b against Covid-19 hospitalization or death (n = 37,844 for Delta predominance period and n = 71,614 for Omicron predominance period). Squares represent the vaccine effectiveness adjusted by age, sex, self-reported race, number of chronic comorbidities, previous symptomatic events notified to the surveillance system, municipality of residence, and RT-PCR/antigen test sample collection date. The error bars represent the 95% confidence interval of the adjusted vaccine effectiveness. Grey shaded area represents the adjusted vaccine effectiveness for the two doses of CoronaVac, green shaded area represents the adjusted vaccine effectiveness for the homologous (CoronaVac) booster dose and the red shaded area represents the adjusted vaccine effectiveness for the heterologous (BNT162b2) booster dose.
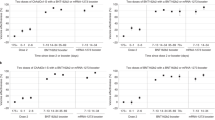
We observed lower vaccine effectiveness against hospitalization or death in individuals aged ≥75 years, compared to younger individuals, for a primary series of CoronaVac, a CoronaVac booster, and for a BNT162b2 booster (Supplementary Table 5 and Table 2). However, vaccine effectiveness against hospitalization and death was significantly higher in individuals aged ≥75 years who received a heterologous BNT162b2 booster than a homologous CoronaVac booster ≥60 days of booster dose (78.5% vs 51.4%, respectively). Vaccine effectiveness against symptomatic disease was overall lower than severe COVID-19 across age groups and an age-related trend was not discernible.
A total of 1,240,266 RT-PCR/antigen tests out of 1,308,364 eligible were selected into matched case-control pairs for the waning vaccine effectiveness in the Omicron period (Supplementary Table 6). Administration of a CoronaVac booster was associated with an increased VE against hospitalization or death relative to individuals who received their second dose ≥180 days previously (Supplementary Table 7 and Table 3; rVE 8-59 days after third dose 47.1%, 95% CI 27.8 to 61.2), but minimal increase in VE against symptomatic disease (rVE 8-59 days after booster dose 4.9%, 95% CI 1.5 to 8.1). In addition, the additional protection gained by the booster dose against hospitalization or death waned after three months (rVE 90-119 days after booster dose 23.5%, 95% CI 12.4 to 33.1; rVE ≥120 days after booster dose 20.7%, 95% CI 10.1 to 30.0). In contrast, a BNT162b2 booster was associated with the substantial increase in protection against hospitalization or death that was maintained for at least four months (Table 3; rVE ≥120 days after booster dose 62.8%, 95% CI 59.3 to 65.9). The gain in VE against the symptomatic disease was lower for the homologous booster and appeared to wane over time for the homologous and heterologous booster (Table 3).
A sensitivity analysis for the matching strategy obtained comparable estimates to the main analysis (Supplementary Table 8, Supplementary Table 9, and Supplementary Table 10), as after using a different definition for severe Covid-19 (Supplementary Table 11 and Supplementary Table 12), and adjusting for month of the second dose (Supplementary Table 13), as a sensitivity analysis that was restricted to RT-PCR tests only (Supplementary Fig. 3, Supplementary Table 14) obtained comparable estimates to the main analysis (Supplementary Table 15, Supplementary Table 16, Supplementary Table 17 and Supplementary Table 18).
Discussion
In this large observational study, we observed substantially lower effectiveness of a primary series of CoronaVac, and of a homologous CoronaVac and heterologous BNT162b2 booster dose, against symptomatic Covid-19 during an Omicron-dominated period compared to a Delta-dominated period. Effectiveness against severe outcomes was more similar between the two periods. In addition, a homologous booster dose conferred no additional protection against symptomatic disease during the Omicron-dominated period, and a moderate increase in protection against severe disease. Of note, the increased protection afforded by a homologous booster against severe disease does waned during the four-month period after its administration. In contrast, the effectiveness of a heterologous BNT162b2 booster dose was substantially higher against symptomatic and severe disease, and protection against severe disease appeared to be durable up to four months.
Our findings have immediate implications for the current suggestion to administer homologous booster doses of inactivated vaccines in the context of the current global spread of the Omicron variant8. There was overall a small benefit of a homologous booster and, for individuals aged ≥75 years, both the primary series and homologous booster afforded limited protection against severe disease (40–50%). However, a heterologous booster dose of BNT162b2 afforded a substantial increase in protection against severe disease in all age groups, including the elderly with age ≥75 years, compared to the primary series and some protection against symptomatic disease, albeit of uncertain duration. Although the direct comparison between homologous and heterologous booster is not straightforward because of the potential confounding factors between the individuals who received each vaccine (Supplementary Table 2), the main differences are region of residence and age, both factors accounted for in our adjustment. Additionally, based on the literature and magnitude of difference on the estimated VEs, it is unlikely the difference to be due to residual confounding. These findings suggest that the use of homologous CoronaVac as an option for booster doses8, may need to be revisited, as preference to heterologous booster doses may be crucial to reducing morbidity and mortality associated with Omicron epidemics. Further research should investigate combinations of heterologous booster doses other than BNT162b2, including non-mRNA vaccines.
The reduced effectiveness of primary vaccination with CoronaVac and subsequent boosting schemes was observed primarily for symptomatic to moderate cases during the Omicron period. Low neutralizing antibody responses against the Omicron variant have been observed in individuals receiving two doses of CoronaVac13,14,15 and three doses of CoronaVac13,16. A BNT162b2 booster dose has been shown to increase neutralizing antibodies against Omicron compared to a primary series of CoronaVac13,16, and to a higher level than individuals who received a primary series of BNT162b215. The protection against severe disease for inactivated vaccines observed in this study speaks to the gaps in understanding of correlates of protection against severe disease, with a decoupling between measured neutralizing antibodies and clinical protection. This disparity has been observed for the primary series of CoronaVac, with moderate-to-high levels of protection against severe disease maintained beyond six months5 despite the lack of detectable neutralizing antibodies during this period17.
Our findings on the effectiveness against severe Covid-19 of homologous and heterologous booster doses during the Delta period is consistent with a previous test-negative study in Brazil5 and with a cohort study from Chile conducted during the same Delta period18. For the Omicron period, our estimates are consistent with an ecological study from Hong Kong regarding the effectiveness of a primary vaccination with CoronaVac12. However, our estimates of vaccine effectiveness against severe disease for a homologous booster are lower than reported the study in Hong Kong. The population seroprevalence in Brazil is higher than in Hong Kong, meaning that there is likely more infection-derived immunity in unvaccinated individuals, leading to lower VE estimates in this context. In addition, differences in study design, time of follow-up, non-pharmaceutical interventions in place during the Omicron outbreak in Hong Kong, and limited sample size for severe disease in the Hong Kong study could introduce differences12.
There was evidence for waning of effectiveness against symptomatic disease for homologous and heterologous boosters, and against severe disease for a homologous booster dose after three months during the Omicron period. This finding is consistent with numerous studies of primary series vaccination4,5,6, and with more recent studies of booster dose effectiveness over time7,19. In this study, we attempted to mitigate this bias by estimating relative VE over time since booster dose administration. We chose to evaluate waning using the reference group of those ≥180 days of second dose, assuming the waning from this period is slow or minimal. Where appreciable waning ≥180 days of second dose occurs, the interpretation of waning from rVE could be limited, because we would compare waning of booster against waning of second dose. Studies designed to identify and mitigate such biases should be prioritized to estimate the extent and timescale of waning effectiveness20,21.
We observed “negative” VE for some vaccination groups of homologous booster particularly for the Omicron period and homologous booster against symptomatic Covid-19. This phenomenon has been observed in some VE studies against Covid-19 and it is likely related to uncontrolled bias22. We observed “negative” VE after some time from the vaccine, likely relating the bias driven by those early adopters or a widespread attack rate during Omicron surge. Additionally, some modeling suggests increased contact between vaccinated individuals associated with low VE could explain “negative” VE23. Other unexpected finding is the lower VE in the groups <75 y compared to ≥75 y against symptomatic COVID-19. Differences in risk behaviour between age groups during the Omicron surge could explain these findings, making higher attack rates among the young and decreasing VE24. This phenomenon was not observed for VE against severe Covid-19.
There are several strengths of our study. We used a nationwide database resulting in a large sample size and geographical coverage. We applied a matched test-negative design, including matching by time of epidemic and each one of 5,570 Brazilian municipalities. Finally, the timing of the booster campaign in Brazil together with the size and extent of the Omicron epidemic afforded us an opportunity to analyze a large population with three vaccine doses during an Omicron-dominated period, providing effectiveness estimates with relatively high precision even in age subgroups and over time.
Some limitations should be acknowledged. The data available for this study was collected as part of Brazil’s passive surveillance efforts for Covid-19, so important covariates may be missing or incomplete. As usually done in population-based studies with record linkage, we considered those individuals not linked to the vaccination database as unvaccinated, so we can have some degree of misclassification on vaccination status. We did not expect a relevant proportion of misclassification because the databases are centrally managed by the same data guarantor and we excluded few inconsistencies between and within databases. The distribution of RT-PCR tests and antigen tests, which have different sensitivity, changed over the course of the study period, which could have led to a decrease in estimated VE during the Omicron period through misclassification. However, a sensitivity analysis restricted to RT-PCR tests produced similar results. In the same topic, a higher vaccine effectiveness was observed in the main analysis against symptomatic Covid-19 during Omicron period (VE: 24.6%) in the period 0-13 days after the first dose (“bias indicator”) compared with the estimate in the sensitivity analysis restricted to RT-PCR tests (VE: 4.6%), showing evidence for potential misclassification of rapid antigen tests. In all analyses the overall vaccine effectiveness estimates were consistent and we don’t expect these biases would change considerably the message of this study. In addition, the test-negative controls may have been different during the Omicron and Delta periods, which could explain some of the difference in VE estimates. In particular, a higher proportion of controls were hospitalized or died during the Delta period (Table 1), implying either that other pathogens with severe outcomes were circulating during that period, or that less testing was being done in the outpatient setting during the Delta period. VE estimates in the primary analysis could be biased downwards due to the accrual of undetected infection in unvaccinated individuals25,26. However, if the additional protection by the vaccine on those with the previous infection are proportional to the added protection in those naive of infection, the bias could be minimal. We tried to adjust for it by using the proxy indication of previous COVID-19 likely illness, and at the same time immunity acquired by natural infection is less protective against Omicron. Our study is observational and so the VE is subject to confounding27, given the bias indicator for the Delta period is close to 0, and for Omicron is significantly different from 0 for symptomatic cases, our VE estimates for the Omicron period appear to be more affected by bias. Additionally, the direct comparison between homologous and heterologous booster doses is not straightforward because there is a possibility for differences in risk by those who were offered and uptake of each booster type. However, we have controlled for important confounders (in particular age, location, time of test, comorbidities), and the difference in effectiveness observed between homologous and heterologous boosters is very unlikely to be explained by unmeasured confounding alone. Nevertheless, our results could be biased through this mechanism, and the direction of bias is unclear. Finally, differences in effectiveness and waning patterns by age could be driven by other factors, including occupational exposure (e.g., health care workers) and personal risk mitigation behavior20.
Overall, we found that primary vaccination with two doses of the CoronaVac vaccine provided 40–50% effectiveness against severe Covid-19 outcomes during the Omicron epidemic in Brazil, although effectiveness against the symptomatic disease was close to zero. While a homologous booster afforded little additional protection, a heterologous booster dose of BNT162b2 restored high effectiveness against severe Covid-19, and moderate effectiveness against symptomatic disease up to four months.
Methods
Study setting and design
We conducted a matched test-negative case-control study between September 6, 2021, and April 22, 2022, in Brazil. The national Covid-19 vaccination campaign started on January 17, 2021, and the administration of booster doses began for the general population on September 6, 2021. The primary series used in Brazil were homologous schemes of Sinovac CoronaVac (two doses), Oxford-AstraZeneca ChAdOx1 nCoV-19 (two doses), Pfizer BNT162b2 (two doses), Janssen Ad26.COV2.S (single dose), and heterologous combinations of the above products in periods of vaccine shortage. All four vaccine products were administered as a homologous or heterologous booster dose. There was no differential recommendation for which vaccine to be administered, except a suggestion for BNT162b2 if available. The booster vaccination followed an age-prioritization scheme. The interval between second and booster doses was initially six months and was subsequently shortened to four months during November 2021 in some states and nationally on December 20, 2021. The proportion of individuals with a primary series of CoronaVac who received a booster dose of Ad26.COV2.S or ChAdOx1 nCoV-19 was small; therefore we limited our analysis to booster doses of CoronaVac and BNT162b2.
Data sources
We obtained individual-level information on Covid-19 outcomes from two national surveillance databases in Brazil: e-SUS and SIVEP-Gripe. e-SUS collects information of any individual suspected to have mild Covid-19 syndromic illnesses, including those who were not tested, tested negative and tested positive. SIVEP-Gripe collects information on any severe acute respiratory infection, including all Covid-19 hospitalizations and deaths3,5,28. We obtained individual-level vaccination status from the national vaccination database (SI-PNI). Notification to these three systems is compulsory in Brazil. The three databases have a unique identifier after pseudo-anonymization by the Ministry of Health. Additional information is available on Supplementary Table 1. We extracted eSUS, SIVEP-Gripe and SI-PNI on 29/04/2022 and used data until 22/04/2022, allowing for a one-week potential delay. This study was approved by the ethical committee for research of Federal University of Mato Grosso do Sul (CAAE: 43289221.5.0000.0021)
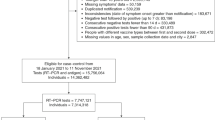
The study population was adults (aged ≥18 years) residing in Brazil, and who underwent SARS-CoV-2 RT-PCR or rapid antigen testing associated with symptomatic illness29 during the study period. We excluded individuals with missing or inconsistent information on age, sex, municipality of residence, and on vaccination and testing status and dates. We excluded RT-PCR/antigen tests that were not collected within 10 days of symptom onset to avoid potentially misclassification, positive or negative RT-PCR/antigen tests with a positive RT-PCR/antigen test in the previous 90 days to capture only incident infections and avoid a second positive test because of prolonged viral shedding, and negative RT-PCR/antigen tests with a positive RT-PCR/antigen test occurring in the following 14 days because of likely false-negative test in the first negative test. For individuals who received multiple RT-PCR or antigen tests during the study period, we included all eligible tests up to and including the first positive test (ie, the first positive test in the study period and at least 90 days prior to another positive). The number of RT-PCR/antigen tests performed during the study period in Brazil is shown in Supplementary Fig. 1.
To assess waning of the booster doses over time since administration, we performed a separate, secondary, case-control analysis on the same study population, restricting to cases and controls who received a primary series of CoronaVac and received an RT-PCR/antigen test at least six months after their second dose, i.e. when eligible for a booster dose. The study design and matching procedure was otherwise the same.
Selection of cases and matched controls
Cases were defined as those from the study population who had Covid-19 symptoms, defined by the presence of at least one symptom: fever, sore throat, headache, cough, chills, runny nose, dyspnea, anosmia, and ageusia, and a positive SARS-CoV-2 RT-PCR/antigen test result. Eligible controls were defined as those from the study population who had Covid-19 symptoms as defined by cases, and a negative SARS-CoV-2 RT-PCR/antigen test result. Finally, we excluded all RT-PCR/antigen tests that were obtained after receipt of a primary series of ChAdOx1 nCoV-19, BNT162b2 or Ad26.COV2.S vaccines.
We matched each case with one control according to the age (± 10 years), sex, municipality of residence, variant period, and RT-PCR/antigen test sample collection date (± 10 days). The algorithm used for the continuous variables (age and test sample collection date) was nearest neighbour matching. After identification of each case, we randomly chose one control from the set of all eligible matching controls, allowing for the replacement of controls. We performed a sensitivity analysis on the matching approach by creating strata of unique combinations of the matching factors (age category in 10 years band, sex, municipality of residence, variant period and week of testing). The numbers of cases and controls per stratum are not pre-specified, and strata with no cases, or with no controls, were excluded. This leads to varying ratios of cases to controls. This was done to use all available information, reducing how often unmatched cases or controls needed to be discarded and no case or control appears in more than one stratum, thus dealing with the potential issue related to replacement. To improve the computational performance of the models while retaining the majority of cases, large strata were reduced in size by dividing into smaller strata. In strata with more controls than cases, each stratum allowed a case to be matched to up to ten controls, and vice versa. For strata with at least ten times as many controls as cases, excess controls were discarded, and vice versa. In this way, strata sizes varied from two to eleven20.
Statistical analysis
We estimated the vaccine effectiveness of booster doses of CoronaVac and BNT162b2 against symptomatic Covid-19 in the 0-7 days, 8-59 days and ≥60 days after the booster dose. We also estimated the vaccine effectiveness of a booster dose against Covid-19 hospitalization and/or death by restricting the analysis population to case-control pairs in which the case was hospitalized or died3,5,30,31. Symptomatic Covid-19 includes mild and severe cases. Severe Covid-19 was defined as hospital admission and death with severe acute respiratory infection due to SARS-CoV-2 (positive RT-PCR/Antigen test). For the analyses of symptomatic and severe Covid-19, we considered the date of respiratory sample collection as the date of the event. There are several choices of controls for severe outcomes, including community nonsyndromic controls, community syndromic controls, and hospitalized test-negative controls with or without symptoms30,32,33. Each has their advantages and disadvantages in how well they represent the source population in their uptake of Covid-19 vaccination. We choose a priori to use community and hospitalized syndromic controls as we agreed these are the controls that better represent the vaccination status in the Brazilian setting. Additionally, we chose syndromic controls to reduce the bias in testing behaviour25, as those tested in the absence of symptoms are more likely to be part of special groups of individuals (e.g., healthcare workers). The reference group was unvaccinated individuals. For the secondary analysis assessing waning effectiveness, we estimated the relative vaccine effectiveness (rVE)7,34, using booster eligible (≥180 days after the second dose) CoronaVac recipients as the reference group, and stratified the time since booster administration by 8–59 days, 60–89 days, 90–119 days and ≥120 days. We used RT-PCR/Antigen test respiratory samples to define cases and controls in any effectiveness analyses. Cases and controls that were not linked to the vaccination database were ascertained as unvaccinated.
We used conditional logistic regression to estimate the adjusted odds ratio (aOR) of vaccination comparing cases and controls, and (1−aOR)*100 provided an estimate of vaccine effectiveness under the assumptions of a test negative design30. Because age is a strong determinant of Covid-19 outcomes, we adjusted for age (as a continuous variable, modeled with a restricted cubic spline) after matching to control for potential residual confounding within age bands. We also adjusted for chronic comorbidities (including cardiovascular, renal, diabetes, chronic respiratory disorder, obesity, or immunosuppression, categorized as 0, 1, and ≥2 comorbidities), self-reported race, and any previous symptomatic event that were reported to the surveillance systems (categorized as 0, and ≥1). We adjusted for self-reported race because it is a main surrogate of socioeconomic status and associated with risk of infection and outcomes in Brazil3. Prior SARS-CoV-2 exposure is defined as notified acute respiratory infection or positive SARS-CoV-2 test result prior to the sampled RT-PCR/Antigen test. This variable is our best surrogate of previously confirmed or suspected infection of SARS-CoV-2. We considered the vaccine effectiveness estimates for the 0-13 days after the first dose as a “bias indicator”, because it is expected that vaccines have no or limited effectiveness for this period35.
We conducted an analysis of vaccine effectiveness within age subgroups (<60, 60-74 and vs ≥75 years old) by adding an interaction term with the vaccination category. Because the analysis period incorporated a Delta (B.1.617.2) (September 6, 2021 to December 14, 2021) and Omicron (December 25, 2021 to April 22, 2022) period, we conducted separate analyses in each time period. We defined the end of the Delta period as when national Omicron VoC prevalence amongst sequenced genomes reached 25% and the beginning of the Omicron period as when the prevalence reached 75% in the GISAID database36. We conducted the same analyses using only RT-PCR tests as a sensitivity analysis, to address potential misclassification. Finally, we conducted two posthoc sensitivity analyses, evaluating vaccine effectiveness in the main analysis population defining severe Covid-19 as use of respiratory support, intensive care admission, and death with severe acute respiratory infection due to SARS-CoV-2 (positive RT-PCR/Antigen test); and evaluating relative vaccine effectiveness in the main analysis population further adjusting by month of second dose as a factor in the model.
All analyses were done in R (v.4.1.2)37
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
Deidentified analysis data sets are available in the Github repository https://github.com/juliocroda/VebraCOVID-19. Any information for assessing the databases must be addressed to the Brazilian Ministry of Health at https://datasus.saude.gov.br/, and requests can be addressed to datasus@saude.gov.br. Our agreement with the Ministry of Health for accessing the databases patently denies authorization of access to the full datasets by a third party because of privacy and ethical/legal issues. For Fig. 1, vaccine data was obtained from OpenDataSUS (https://opendatasus.saude.gov.br/, access date 2022-05-09) and variant data from GISAID (https://www.gisaid.org/hcov19-variants/, access date 2022-05-09).
Code availability
Code used to perform conduct statistical analysis is available in the repository https://github.com/juliocroda/VebraCOVID-19
References
Voysey, M. et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397, 99–111 (2021).
Polack, F. P. et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med 383, 2603–2615 (2020).
Ranzani, O. T. et al. Effectiveness of the CoronaVac vaccine in older adults during a gamma variant associated epidemic of covid-19 in Brazil: test negative case-control study. BMJ. https://doi.org/10.1136/bmj.n2015 (2021).
Accorsi, E. K. et al. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 327, 639 (2022).
Cerqueira-Silva, T. et al. Vaccine effectiveness of heterologous CoronaVac plus BNT162b2 in Brazil. Nat. Med. https://doi.org/10.1038/s41591-022-01701-w (2022).
Chemaitelly, H. et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med 385, e83 (2021).
Andrews, N. et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. https://doi.org/10.1056/NEJMoa2119451 (2022).
Strategic Advisory Group of Experts on Immunization—SAGE (WHO). Highlights from the Meeting of the Strategic Advisory Group of Experts (SAGE) on Immunization, 4-7 October 2021. (2021).
Abu-Raddad, L. J. et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. https://doi.org/10.1056/NEJMoa2200797 (2022).
Feikin, D. R. et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet 399, 924–944 (2022).
Dolgin, E. Omicron thwarts some of the world’s most-used COVID vaccines. Nature 601, 311–311 (2022).
McMenamin, M. E. et al. Vaccine effectiveness of one, two, and three doses of BNT162b2 and CoronaVac against COVID-19 in Hong Kong: a population-based observational study. Lancet Infect. Dis. https://doi.org/10.1016/S1473-3099(22)00345-0 (2022).
Cheng, S. M. S. et al. Neutralizing antibodies against the SARS-CoV-2 Omicron variant BA.1 following homologous and heterologous CoronaVac or BNT162b2 vaccination. Nat. Med 28, 486–489 (2022).
Lu, L. et al. Neutralization of Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant by Sera From BNT162b2 or CoronaVac Vaccine Recipients. Clin. Infect. Dis. ciab1041 https://doi.org/10.1093/cid/ciab1041 (2021).
Pérez-Then, E. et al. Neutralizing antibodies against the SARS-CoV-2 Delta and Omicron variants following heterologous CoronaVac plus BNT162b2 booster vaccination. Nat. Med 28, 481–485 (2022).
Costa Clemens, S. A. et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): a phase 4, non-inferiority, single blind, randomised study. Lancet 399, 521–529 (2022).
Zeng, G. et al. Immunogenicity and safety of a third dose of CoronaVac, and immune persistence of a two-dose schedule, in healthy adults: interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect. Dis. 22, 483–495 (2022).
Jara, A. et al. Effectiveness of homologous and heterologous booster doses for an inactivated SARS-CoV-2 vaccine: a large-scale prospective cohort study. Lancet Glob. Health 10, e798–e806 (2022).
Ferdinands, J. M. et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 71, 255–263 (2022).
Hitchings, M. D. T. et al. Change in covid-19 risk over time following vaccination with CoronaVac: test negative case-control study. BMJ e070102 https://doi.org/10.1136/bmj-2022-070102 (2022).
Kahn, R., Schrag, S. J., Verani, J. R. & Lipsitch, M. Identifying and Alleviating Bias Due to Differential Depletion of Susceptible People in Postmarketing Evaluations of COVID-19 Vaccines. Am. J. Epidemiol. 191, 800–811 (2022).
Hansen, C. H. et al. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://doi.org/10.1101/2021.12.20.21267966 (2021).
Bodner, K., Knight, J., Hamilton, M. A. & Mishra, S. Higher contact among vaccinated can be a mechanism for negative vaccine effectiveness. https://doi.org/10.1101/2022.04.25.22274266 (2022).
Kaslow, D. C. Force of infection: a determinant of vaccine efficacy? npj Vaccines 6, 51 (2021).
Lewnard, J. A. et al. Theoretical Framework for Retrospective Studies of the Effectiveness of SARS-CoV-2 Vaccines. Epidemiology 32, 508–517 (2021).
Lipsitch, M., Goldstein, E., Ray, G. T. & Fireman, B. Depletion-of-susceptibles bias in influenza vaccine waning studies: how to ensure robust results. Epidemiol. Infect. 147, e306 (2019).
Dean, N. E., Hogan, J. W. & Schnitzer, M. E. Covid-19 Vaccine Effectiveness and the Test-Negative Design. N. Engl. J. Med 385, 1431–1433 (2021).
Bastos, L. S. et al. COVID-19 and hospitalizations for SARI in Brazil: a comparison up to the 12th epidemiological week of 2020. Cad. Saúde. Pública 36, e00070120 (2020).
Brazilian Ministry of Health. Epidemiologic Surveillance Guide. National Emergency of Public Health Concern due to the COVID-19 disease.
Sullivan, S. G., Tchetgen Tchetgen, E. J. & Cowling, B. J. Theoretical Basis of the Test-Negative Study Design for Assessment of Influenza Vaccine Effectiveness. Am. J. Epidemiol. 184, 345–353 (2016).
Andrejko, K. L. et al. Prevention of Coronavirus Disease 2019 (COVID-19) by mRNA-Based Vaccines Within the General Population of California. Clin. Infect. Dis. 74, 1382–1389 (2022).
Chua, H. et al. The Use of Test-negative Controls to Monitor Vaccine Effectiveness: A Systematic Review of Methodology. Epidemiology 31, 43–64 (2020).
Foppa, I. M. et al. The case test-negative design for studies of the effectiveness of influenza vaccine in inpatient settings. Int. J. Epidemiol. dyw022 https://doi.org/10.1093/ije/dyw022 (2016).
Thompson, M. G. et al. Effectiveness of Covid-19 Vaccines in Ambulatory and Inpatient Care Settings. N. Engl. J. Med 385, 1355–1371 (2021).
Hitchings, M. D. T. et al. Use of Recently Vaccinated Individuals to Detect Bias in Test-Negative Case–Control Studies of COVID-19 Vaccine Effectiveness. Epidemiology 33, 450–456 (2022).
GISAID—hCov19 Variants. Export 09/05/2022. https://www.gisaid.org/hcov19-variants/.
R Core Team. R: A language and environment for statistical computing. (2021).
Acknowledgements
We thank the Pan American Health Organization for its support. No external funding was provided for this study. OTR is funded by a Sara Borrell fellowship (CD19/00110) from the Instituto de Salud Carlos III. OTR acknowledges support from the Spanish Ministry of Science and Innovation through the Centro de Excelencia Severo Ochoa 2019-2023 programme (CEX2018-000806-S) and from the Generalitat de Catalunya through the Centres de Recerca de Catalunya (CERCA) programme. DATC and MDH report a contract from Merck (to the University of Florida) for research unrelated to this manuscript. These institutions had no role in the study design, data collection, data analysis, data interpretation, or writing of the report.
Author information
Authors and Affiliations
Contributions
All authors conceived the study. D.A.T.C., N.E.D., J.R.A., A.I.K., and J.C. contributed equally as senior authors. O.T.R. completed analyses with guidance from M.D.T.H., M.L.L., D.A.T.C., N.E.D., J.R.A., A.I.K., and J.C. M.S.S.T., D.H.T., L.C.S.D., M.D.T.H. and O.T.R. curated and validated the data. O.T.R. and M.D.T.H. wrote the first draft of the manuscript. R.L.M., G.V.A.F., C.F.R.F., M.A., R.F.C.S. and R.D.O. provided supervision. All authors contributed to, and approved, the final manuscript. O.T.R. and J.C. had verified the data. J.C. is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Nick Andrews and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ranzani, O.T., Hitchings, M.D.T., de Melo, R.L. et al. Effectiveness of an inactivated Covid-19 vaccine with homologous and heterologous boosters against Omicron in Brazil. Nat Commun 13, 5536 (2022). https://doi.org/10.1038/s41467-022-33169-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-022-33169-0
This article is cited by
-
Viral coinfection in hospitalized patients during the COVID-19 pandemic in Southern Brazil: a retrospective cohort study
Respiratory Research (2024)
-
Current Progress, Challenges and Prospects in the Development of COVID-19 Vaccines
Drugs (2024)
-
COVID-19 vaccine updates for people under different conditions
Science China Life Sciences (2024)
-
Immunogenicity and safety of RAZI recombinant spike protein vaccine (RCP) as a booster dose after priming with BBIBP-CorV: a parallel two groups, randomized, double blind trial
BMC Medicine (2024)
-
Dynamic clade transitions and the influence of vaccination on the spatiotemporal circulation of SARS-CoV-2 variants
npj Vaccines (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
