
Abstract
Beta thalassemia minor (BTM) is a hereditary disease caused by defective globin synthesis and it is frequently asymptomatic or only mildly anemic. Female sexual dysfunction affects 21–41% of women worldwide. In this study we aimed to investigate female sexual dysfunction in subjects with BTM. A total of 183 subjects who had regular sexual intercourse with marital partners were enrolled in this cross-sectional study. The study group was comprised of 87 subjects with BTM and the control group included 96 healthy subjects. Hemoglobin electrophoresis were performed in all subjects, and all participants were assessed by the Female Sexual Function Index (FSFI) questionnaire and the Arizona Sexual Experience Scale (ASEX). The FSFI scores of the study group were significantly lower than in the control group (19.1 ± 9.6 vs. 25.2 ± 6.6, p < 0.001). Conversely, the ASEX scores of the study group were higher than in the control group (15.2 ± 41 vs. 13.5 ± 6.1, p = 0.0085). Sexual functions were poor in subjects with BTM in this study and we conclude that certain metabolic diseases associated with BTM, such as insulin resistance, hyperglycemia and dyslipidemia, may be the main causes of sexual dysfunctions in these subjects.
Similar content being viewed by others


Introduction
Thalassemia is a heterogenic group of inherited blood disorder that occurs due to the mutation in the gene related to the synthesis of hemoglobin. The beta thalassemias are caused by deficient synthesis of the beta chains of hemoglobin and may result in many clinical types ranging from severely anemic to asymptomatic individuals [1]. Beta-thalassemia minor (BTM) is an important public health problem and nearly 1.5% of world population is BTM. The disease is common in Mediterranean countries and also in several parts of Asia, Africa, and South America [1, 2].
Sexuality is an important physiological event of human life and it can influence both the physical and mental health of a subject [3]. Female sexual dysfunction (FSD) affects 21–41% of women worldwide, making it a common medical problem [4]. It is mostly caused by neurogenic, psychogenic, and vascular factors or generally by the combination of those factors [5]. Sexual functions can be also impaired by the metabolic disorders. Diabetes mellitus is one of the most common systemic diseases that cause sexual function disorder [6]. Insulin resistance was found to be associated with impairment of sexual desire and satisfaction [7]. Hypertension may contribute to sexual dysfunction: blood pressure alterations can affect vascular functions in the female genital tract [8]. Hypertensive women showed lower vaginal lubrication, less frequent orgasms and more frequent pain than normotensive women [9]. Impaired lipid profile has also previously been reported as a risk factor for the development of sexual dysfunction [10].
Previous studies have shown associations between BTM and some metabolic and/or systemic disorders. According to these studies, hypertension is less frequent in persons with BTM as compared with the normal population [11]. Conversely, high blood glucose, insulin resistance and lipid disorders are common with this genetic disorder [12].
To our knowledge, no studies have been carried out to determine sexual functions of subjects with BTM. The objective of this study was therefore to evaluate sexual functions in female subjects with BTM.
Materials and methods
The study was carried out in the internal medicine outpatient clinic of a tertiary hospital from March 2018 to December 2018. It was performed according to the terms of the ethical standards of the committee responsible for human experimentation and in accordance with the Declaration of Helsinki. The protocol was approved by the local Ethics Committee (05/12/2018-343) and an informed consent was obtained before enrollment.
Power analysis (for 80% power and 0.05 type 1 error) was performed to determine the optimum sample size for the study and a total of 183 subjects who had regular sexual intercourse with marital partners were enrolled in this cross-sectional study. The study group was comprised of 87 subjects with BTM and the control group included 96 healthy subjects. Both of the groups (BTM and healthy) were in the same population (Adana, Turkey) and they were chosen on a voluntary basis who admitted to the internal medicine outpatient clinics of the institute. Subjects in the control group had no health complaints and were admitted only for check-up. Patients with a history of diabetes, hypertension, dyslipidemia, obesity, ischemic heart disease, malignancy, mental disorder, chronic obstructive pulmonary disease, obstructive sleep apnea syndrome, cerebrovascular disease or other diseases that would interfere with sexual function, or who used sex-enhancing medication, were excluded. Breastfeeding, pregnant and nonsexually active women as well as under 18 years olds were also excluded.
A venous blood sample was collected in the morning after overnight fasting. The complete blood count and peripheral blood samples were evaluated in all of the subjects. The measurements taken included blood glucose, insulin, serum lipid concentrations, ferritin, vitamin B12, and folate. Serum fasting glucose and lipids were analyzed on the Beckman Coulter Synchron LX 20 (MA, USA), using commercially available kits. Insulin levels were measured using the Abbott Architect I 2000 SR analyzer system (IL, USA). The hemoglobin electrophoreses of all of the subjects were analyzed using the Primus Ultra 2 (USA) with high-performance liquid chromatography. A diagnosis of BTM was established on the basis of hemoglobin A2 (HbA2) ≥3.5 %, mean corpuscular volume (MCV) < 80 fl, and hemoglobin F between 2 and 10%. Complete blood counts were measured with the Sysmex XE 2100i (Japan) by fluorescence flow cytometry, and the biochemical values were analyzed on the Beckman Coulter Synchron LX 20 (MA, USA) using commercially available kits. Ferritin, vitamin B12 and folate levels were measured with the Roche C-601 analyzer system (Japan) using an electrochemiluminescence immunoassay.
All participants were dressed in lightweight clothes during the measurement of their weight. The women’s height was measured in centimeters, their weight was measured in kilograms and their body mass index (BMI) was calculated as the ratio of weight/height2 (kg/m2).
Blood pressure was measured by using periodically calibrated sphygmomanometers (Erka, Germany) and two separate readings, at five-minute intervals.
The sexual functions of participants were assessed using the FSFI questionnaire and the ASEX scale. The FSFI has 19 questions and grouped as follows: desire, arousal, vaginal lubrication, orgasm, sexual satisfaction, pain. The score ranges from 2 to 36 and women with scores ≤ 26.5 were considered as having sexual dysfunction: a lower score of FSFI indicating greater sexual dysfunction [13]. The ASEX is a five-item survey that assesses sexual drive, arousal, vaginal lubrication, ability to reach orgasm and satisfaction from orgasm. Responses are scored on a 1–6 Likert scale with a potential range of 5–30; higher scores indicate worse sexual function whereas absolute scores of ≥19 indicate sexual dysfunction [14]. The Turkish validity and reliability tests of the FSFI and ASEX were conducted prior to our study [15, 16].
Statistical analysis
The MedCalc v19.0.5 software program (MedCalc Belgium) was used for statistical analyses. Categorical measurements were reported as numbers and percentages. Quantitative measurements were reported as the mean ± standard deviation. The Kolmogorov-Smirnov test was used to show the normal distribution of quantitative measurements. The T test or Mann Whitney U tests were used for comparison of quantitative measurements between the two groups. Rank correlation was used to analyze the degree of association between the FSFI and the ASEX (Spearman correlation coefficient rho and/or Kendall’s tau with p-value, and a 95% confidence interval (CI) for the correlation coefficient). The multiple linear regression test (backward method) was used to analyze the relationship between a dependent variable (FSFI) and one or more independent variables (predictor variables or explanatory variables). A p-value of less than 0.05 was considered to be statistically significant.
Results
Table 1 shows the demographical and clinical characteristics of the groups. The groups were comparable according to the age and BMI (p > 0.05). The mean ages of the study and control groups were 35.4 ± 10.1 and 35.1 ± 5.8 years old, respectively. The BMI of the groups were 24.7 ± 1.9 and 24.3 ± 1.1, respectively. The mean HbA2 levels were 5.3 ± 0.4 and 2.1 ± 0.3, respectively, and there was a statistically significant difference between the study and control groups (p < 0.001). Not surprisingly, there were significant differences between the MCV values and hemoglobin F values in both groups (p < 0.001 for each). Vitamin B12, folate and ferritin levels of both groups were comparable (p = 0.513, 0.912, 0.633, respectively). Blood glucose, insulin, and lipids of both groups are shown in Table 2. Blood glucose, insulin, and triglyceride concentrations were high in subjects with BTM (p = 0.001, 0.0049, 0.031, respectively). Low-density lipoprotein cholesterol concentrations were comparable in both groups (p = 0.973). High-density lipoprotein (HDL) cholesterol concentrations were lower in subjects with BTM (p < 0.001). Systolic (120.9 ± 13.3 vs. 117.4 ± 13.0, p = 0.075) and diastolic (77.4 ± 9.2 vs. 75.2 ± 8.9, p = 0.101) blood pressures were comparable in both groups.
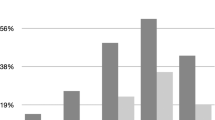
The scores of FSFI and ASEX are shown in Table 3. FSFI scores of the study group were significantly lower than in the control group (19.1 ± 9.6 vs. 25.2 ± 6.6, p < 0.001). Conversely, the ASEX scores of the study group were higher than in the control group (15.2 ± 4.0 vs. 13.3 ± 6.3, p = 0.0085). As expected, there was a negative correlation between the FSFI and ASEX scores (r = −0.230, p = 0.032).
Multiple regression analyses (backward method) were performed with FSFI as a dependent variable and with age, BMI, glucose, insulin, triglyceride, LDL, HDL, systolic, and diastolic blood pressures as independent variables in the study group. A significant correlation persisted between FSFI and insulin (p < 0.001), and between FSFI and triglyceride (p = 0.0048).
Discussion
In this study we investigated for the first time FSD in subjects with BTM. We assessed the sexual function of participants with both the FSFI questionnaire and the ASEX score. Sexual functions of women with BTM were poor when compared with the healthy population in our study. FSFI scores were low and ASEX scores were high in subjects with BTM.
A healthy and satisfying sex life is an important physiological need for the holistic eudemonia of many young and middle-aged women. Multiple studies have shown a strong positive association between sexual function and health-related quality of life [17, 18]. Although subjects with BTM are frequently asymptomatic, this blood disorder is associated with mental disorders such as depression [19]. Increases in depressive symptoms result in decreases in sexual functions in women [20]. In addition, BTM has been reported to be associated with certain metabolic diseases such as diabetes, insulin resistance and dyslipidemia, which are associated with sexual dysfunction [6, 7, 10, 12].
In accordance with the literature, serum insulin levels and blood sugars of subjects with BTM were higher than the healthy controls in the current study. Further reinforcing this link, Tong et al. showed high fasting insulin levels and insulin resistance in BTM subjects with normal glucose tolerance [21]. Increased oxidative stress secondary to chronic microcytic hemolysis and inflammation facilitates the development of insulin resistance and diabetes in subjects with BTM [21]. Disorder of the female sexual arousal response and the orgasm were previously reported to be associated with insulin resistance. Moreover, a positive association between increased clitoral vascular resistance and high insulin level was reported in a study by Maseroli et al. [22, 23]. Diabetes is the leading metabolic disorder among systemic diseases that cause sexual function disorders. Ozcan et al. conducted a study on 310 women with diabetes in Turkey. The frequency of sexual dysfunction in women with type 2 DM was found to be 46.7% in their study [24]. Esposito et al. studied 595 women with type 2 diabetes in Italy and reported the sexual dysfunction prevalence was 53.4% in women patients with diabetes [25]. Neuropathy, vascular impairment and psychological complaints have an important role in the development sexual dysfunction in patients with diabetes. Neurovascular processes that mediate genital vasocongestion are impaired in diabetes [26] and lead to vaginal discomfort and dyspareunia in diabetic women. In addition, psychological problems associated with diabetes may prevent orgasm in female subjects [27].
Serum triglyceride (TG) concentrations were high and HDL concentrations were low in the subjects with BTM in our study. Insulin resistance and high glucose levels may lead to high TG levels in these subjects. In accordance with this link, high TG and low HDL concentrations as well as an increased TG/HDL ratio due to the insulin resistance, were reported by Von Bibra et al. [28]. Low HDL concentrations were also reported by Tong et al. in subjects with BTM [21]. Increased prevalence of female sexual dysfunction in women with dyslipidemia was studied by Esposito et al. They highlighted that HDL cholesterol and TG concentrations were independent predictors of a lower FSFI score [29]. In addition, Maseroli et al. studied 71 women for sexual dysfunction and they demonstrated that decreased HDL cholesterol and increased TGs were associated with increased vascular resistance in the clitoris [23].
This study has some limitations, namely the cross-sectional design, the fact that the genetic analysis was not performed for the diagnosis of BTM, the fact that due to volunteer participation, sexual function research may be characterized by a bias. Furthermore, we did not evaluate the sexual function of partners.
Conclusion
In conclusion, sexual function was found to be poor in subjects with BTM in this study. FSFI scores were low and ASEX scores were high, sustaining the possibility that certain metabolic diseases associated with BTM, such as insulin resistance, hyperglycemia and dyslipidemia, may lead to sexual dysfunctions. Multicenter longitudinal studies with larger sample sizes would provide clearer and greater information about sexual dysfunction in subjects with BTM.
References
Galanello R, Origa R. Beta-thalassemia. Orphanet J Rare Dis. 2010;21:5–11.
Kalleas C, Anagnostopoulos K, Sinopoulou K, Delaki E, Margaritis D, Bourikas G, et al. Phenotype and genotype frequency of beta-thalassemia and sickle cell disease carriers in Halkidiki, Northern Greece. Hemoglobin. 2012;36:64–72.
World Health Organization. Sexual and reproductive health, working definitions. http://www.who.int/reproductivehealth/topics/sexual_health/sh_definitions/en/. Accessed 11 Jul 2019.
McCool ME, Zuelke A, Theurich MA, Knuettel H, Ricci C, Apfelbacher C. Prevalence of female sexual dysfunction among premenopausal women: a systematic review and meta-analysis of observational studies. Sex Med Rev. 2016;4:197–212.
Erol B, Tefekli A, Sanli O, Ziylan O, Armagan A, Kendirci M, et al. Does sexual dysfunction correlate with deterioration of somatic sensory system in diabetic women? Int J Impot Res. 2003;15:198–202.
Pontiroli AE, Cortelazzi D, Morabito A. Female sexual dysfunction and diabetes: a systematic review and metaanalysis. J Sex Med. 2013;10:1044–51.
Krysiak R, Drosdzol-Cop A, Skrzypulec-Plinta V, Okopień B. Sexual functioning and depressive symptoms in women with diabetes and prediabetes receiving metformin therapy: a pilot study. Exp Clin Endocrinol Diabetes. 2017;125:42–8.
Maseroli E, Scavello I, Vignozzi L. Cardiometabolic risk and female sexuality-Part I. Risk factors and potential pathophysiological underpinnings for female vasculogenic sexual dysfunction syndromes. Sex Med Rev. 2018;6:508–24. https://doi.org/10.1016/j.sxmr.2018.02.009.
Duncan LE, Lewis C, Jenkins P, Pearson TA. Does hypertension and its pharmacotherapy affect the quality of sexual function in women? Am J Hypertens. 2000;13:640–7.
Baldassarre M, Alvisi S, Mancini I, Moscatiello S, Marchesini G, Seracchioli R, et al. Impaired lipid profile is a risk factor for the development of sexual dysfunction in women. J Sex Med. 2016;13:46–54.
Gozashti MH, Hasanzadeh A, Mashrouteh M. Prevalence of metabolic syndrome in patients with minor beta thalassemia and its related factors: a cross-sectional study. J Diabetes Metab Disord. 2014;13:108.
Kırım S, Keşkek ŞÖ, Turhan A, Saler T. Is β-thalassaemia minor associated with metabolic disorder? Med Princ Pract. 2014;23:421–5.
Rosen C, Brown J, Heiman S, Leiblum C, Meston R, Shabsigh D, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208.
McGahuey CA, Gelenberg AJ, Laukes CA, Moreno FA, Delgado PL, McKnight KM, et al. The Arizona Sexual Experience Scale (ASEX): reliability and validity. J Sex Marital Ther. 2000;26:25–40.
Aygin D, Eti Aslan F. The Turkish adaptation of The Female Sexual Function Index, Turkey clinics. J Med. 2005;25:393–9.
Soykan A. The reliability and validity of Arizona sexual experiences scale in Turkish ESRD patients undergoing hemodialysis. Int J Impot Res. 2004;16:531–4. https://doi.org/10.1038/sj.ijir.3901249.
Biddle AK, West SL, D’Aloisio AA, Wheeler SB, Borisov NN, Thorp J. Hypoactive sexual desire disorder in postmenopausal women: quality of life and health burden. Value Health. 2009;12:763–72.
Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, Moreira E, et al. Sexual problems among women and men aged 40-80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17:39–57.
Keşkek SO, Kirim S, Turhan A, Turhan FG. Depression in subjects with beta-thalassemia minor. Ann Hematol. 2013;92:1611–5.
Ozturk S, Sut HK, Kucuk L. Examination of sexual functions and depressive symptoms among infertile and fertile women. Pak J Med Sci. 2019;35:1355–60.
Tong Peter CY, Ng Maggie CY, Ho Vhung S, So Wing Y, Li June KY, Lam Chris WK, et al. C-reactive protein and Insulin resistance in subject with thalassemia minor and a family history of diabetes. Diabetes Care. 2002;25:1480–1.
Zsoldos M, Pajor A, Pusztafalvi H. [Relation between sexual dysfunction and metabolic syndrome]. Orv Hetil. 2019;160:98–103.
Maseroli E, Fanni E, Cipriani S, Scavello I, Pampaloni F, Battaglia C, et al. Cardiometabolic risk and female sexuality: focus on clitoral vascular resistance. J Sex Med. 2016;13:1651–61.
Ozcan S, Sahin Nevin H, Bilgic D, Yilmaz Sema D. Is sexual dysfunction associated with diabetes control and related factors in women with diabetes. Sex Disabil. 2011;29:251–61.
Esposito K, Maiorino MI, Bellastella G, Giugliano F, Romano M, Giugliano D. Determinants of female sexual dysfunction in type 2 diabetes. Int J Impot Res. 2010;22:179–84.
Kizilay F, Gali HE, Serefoglu EC. Diabetes and sexuality. Sex Med Rev. 2017;5:45–51. https://doi.org/10.1016/j.sxmr.2016.07.002.
Kolodny RC. Sexual dysfunction in diabetic females. Diabetes. 1971;20:557–9.
Von Bibra H, Saha S, Hapfelmeier A, Müller G, Schwarz PEH. Impact of the triglyceride/high-density lipoprotein cholesterol ratio and the hypertriglyceremic-waist phenotype to predict the metabolic syndrome and insulin resistance. Horm Metab Res. 2017;49:542–9.
Esposito K, Ciotola M, Maiorino MI, Giugliano F, Autorino R, De Sio M, et al. Hyperlipidemia and sexual function in premenopausal women. J Sex Med. 2009;6:1696–703.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Keşkek, Ş.Ö., Demirtaş, D., Uysal, G. et al. Sexual dysfunction in female subjects with beta-thalassemia minor. Int J Impot Res 32, 358–362 (2020). https://doi.org/10.1038/s41443-020-0283-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41443-020-0283-z
