
Abstract
Objectives
To investigate the rate of orthokeratology lens (ortho-k lens) use and its associated factors in children and adolescents with myopia.
Methods
Cross-sectional study. Children from 104 primary and middle schools in Shanghai were enrolled by cluster sampling. Ophthalmic examinations were conducted and information was obtained using questionnaires for associated factors analysis.
Results
A total of 72,920 children and adolescents were included, among which 32,259 were the potential population for ortho-k lens use. A total of 1021 participants used ortho-k lenses, equating to a use rate of 1.4% in the total population and 3.1% in the potential population. Age (OR 0.91, 95% CI: 0.88–0.95, p < 0.001), BMI (≥95th percentile: OR 0.48, 95% CI: 0.35–0.66, p < 0.001), age at initiation of refractive correction (≤12 years: OR 1.75, 95% CI: 1.31–2.33, p < 0.001), and parental myopia (either: OR 2.09, 95% CI: 1.58–2.75, p < 0.001; both: OR 3.94, 95% CI: 3.04–5.11, p < 0.001) were independently associated with ortho-k lens use. Of the ortho-k lenses users, 12.4% had a logMAR CVA of ≥0.3. A correction target (SE) of ≤−3.0 D (OR 2.05, 95% CI: 1.38–3.05, p < 0.001) and a sleeping duration of ≤6 h (OR 4.19, 95% CI: 2.03–8.64, p < 0.001) were factors independently associated with CVA ≥ 0.3.
Conclusions
A certain proportion of children and adolescents in Shanghai chose to wear ortho-k lenses, related to the situation of parents and children themselves. Health education and follow-ups should be strengthened to ensure orthokeratology application quality.
Similar content being viewed by others


Introduction
The worldwide prevalence of myopia has risen sharply over the years, with the prevalence in certain regions, such as China, Japan and South Korea, reaching ≥80% and the prevalence of high myopia >10% [1,2,3,4,5]. Myopia progression is usually accompanied by axial length elongation [6, 7]. The stretching of eyeball wall in high myopia can induce various complications, which may lead to visual impairment and blindness [8,9,10,11]. Thus, effective measures should be taken to control myopia progression once it occurs.
Meta-analyses have indicated that orthokeratology lenses (ortho-k lenses) can reduce axial growth by 0.15 mm/year or 0.26–0.27 mm in 2 years in individuals with low and moderate myopia [12,13,14,15,16]. The process of corneal reshaping can decrease peripheral hyperopic defocus to increases peripheral myopic defocus and reduce stimuli for axial elongation, which is a possible mechanism for delaying the progression of myopia [17]. Ortho-k lenses are worn to flatten the cornea overnight, and wearers consequently possess good unaided vision during the daytime [18]. With ortho-k lenses becoming a widely used optical control intervention, the efficacy and safety of ortho-k lenses have been well studied; however, few studies have examined the use rate and other associated factors of ortho-k lens use.
In light of this research gap, our study was designed to explore the rate of ortho-k lens use and its associated factors in a large paediatric population aged 6–18 years, as well as the distribution of daytime corrected visual acuity (CVA) after one night of wearing ortho-k lenses.
Materials and methods
Study design and population
As a sub-project of the Shanghai Child and Adolescent Large Eye Study, some detailed methods of the study have previously been reported [19]. In this cross-sectional study, primary and secondary schools in Shanghai were selected by cluster sampling in 2019. A total of 104 schools were included, including 36 primary schools, 45 junior high schools, and 43 senior high schools. Written informed consent was obtained from the parents or guardians of the participants, and verbal consent was obtained from the participants. The tenets of the Declaration of Helsinki were followed, and the Institutional Review Board of Shanghai General Hospital, Shanghai Jiao Tong University, approved the study (ID: 2015KY149). Related supporting information has been provided in the methodology article published previously [19]. Basic information, such as height and weight, was collected from all participants, ophthalmic examinations were performed, and the participants were asked to complete a questionnaire.
The exclusion criteria of the study were as follows: (1) eye diseases other than refractive errors; (2) a history of eye trauma or eye surgery; (3) failure to complete the questionnaire or to undergo ophthalmic examinations; (4) lack of refractive information or conjoint use of any other optical correction except single vision spectacles by ortho-k lens users. Primary outcome measures were the rate of ortho-k lens use and its associated factors. Secondary outcome measures were the rate and associated factors of users with unsatisfactory daytime vision.
Ophthalmic examinations
Ophthalmic examinations were performed for all children by specialized and experienced ophthalmologists or optometrists from local community hospitals. An international standard logarithmic visual acuity chart was used to measure unaided vision for all children and CVA for children wearing spectacles or lenses. Visual acuity measurements were recorded as the logarithm of the minimum angle of resolution (logMAR). Autorefraction was performed with an autorefractor (model KR-8900; Topcon, Tokyo, Japan) without cycloplegia. Five readings were obtained and averaged, all of which had to be less than 0.25 dioptre (D) apart. The spherical equivalent (SE) was calculated as the sum of the spherical power plus half of the cylindrical power. All of the examinations were carried out on school days and completed between 8 a.m. and 3 p.m.
Questionnaires
Children’s parents or guardians, together with children themselves, were required to complete an online questionnaire prior to the ophthalmic examination. The questionnaire assessed the chosen correction method at the time; the power of spectacles or lenses, including ortho-k lenses; basic information; premature birth; the refractive status of the parents; age at the start of refractive correction and the sleeping duration on school days. In the questionnaire, the chosen correction method by the time included the following options: single-vision spectacles, defocus spectacles, soft contact lenses, ortho-k lenses, and others.
Definition and evaluation criteria
In this study, the unaided daytime vision after one night’s use of ortho-k lenses was regarded as the CVA. An unsatisfactory CVA was defined as a CVA of ≥0.3 considering that this is the boundary visual acuity of mild visual impairment based on standard WHO definition [20]. The target of correction of ortho-k lenses (regarded as SE [D]) was defined as the sum of the spherical power plus half of the cylindrical power of the lens. Low myopia was defined as an SE of >−3.0 D, and moderate to high myopia was defined as an SE of ≤−3.0 D.
According to the range of applications of ortho-k lenses registered in the National Medical Products Administration, the spherical degree of an ortho-k lens wearer should be between 0 D and −6.0 D, while the cylindrical degree should be ≤2.0 D. In clinical practice, ortho-k lenses are commonly used within a correction range of −5.0 D ≤ SE ≤ − 1.0 D; therefore, in this study, the potential population was defined as the potential clinical user of ortho-k lens, with −5.0 D ≤ SE ≤ − 1.0 D and cylindrical degree ≤2.0 D.
Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Underweight, healthy, overweight, and obesity were categorized according to recent published research [21, 22].
Statistical analysis
Weight and BMI values less than the 1st percentile and greater than the 99th percentile were removed. Due to the high correlation between both eyes in the study, only the refractive and visual acuity data of the right eye were included in the analysis (Pearson’s correlation coefficient = 0.908, p < 0.001). The ortho-k lens wearing rates in the total population and in the potential population were calculated. After verifying normal distribution and homogeneity of variance, parametric variables were compared using an independent-samples t-test and are expressed as mean ± standard deviation (SD). Dichotomous variables were compared using the χ2 test according to grouping and are expressed as N (%). Otherwise, u-test or other methods were used for comparison. The selection of variables included in the regression model considered both the results of univariate analysis and the clinical significance of variables. A P < 0.05 was considered statistically significant.
Results
General characteristics of participants
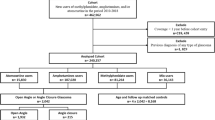
A total of 76,526 children and adolescents from 104 primary and secondary schools were enrolled. A total of 3542 met the criteria for exclusion. Finally, 72,920 children and adolescents (37,170 boys and 35,750 girls) were included in the analysis. The participants ranged in age from 6 to 18 years (mean age, 11.96 ± 3.52 years). Of these, 1021 wore ortho-k lenses, while 71,899 did not. The selected potential population of non-wearers comprised 32,259 participants (15,659 boys and 16,600 girls), with a mean age of 13.04 ± 2.95 years, while the 1021 wearers (417 boys and 604 girls) had a mean age of 12.38 ± 2.57 years. The detailed screening process is shown in Fig. 1. The basic information of the participants is shown in Table 1. Age, sex, height, and weight of children from enrolled schools and those from non-enrolled schools were compared and that our sample was representative.

*The potential population of ortho-k lens use was defined as −5.0 D ≤ SE ≤ − 1.0 D and a cylindrical degree of ≤2.0 D for non-users.
Ortho-k lens wearing rate
The distribution of age and correction target in ortho-k lens users is shown in Fig. 2. The children who wore ortho-k lenses were mainly concentrated in the 10–13-year age group, which comprised 53.2% of the total wearers, with the majority (15.1%) being 12 years of age. Up to 53.0% of ortho-k lens users had a correction target (SE) of between −3.0 D and −1.0 D.

The distribution, range and average of age (a), CVA (b), sleeping time on school days (c), and correction target (d) of ortho-k lens users. CVA corrected vision acuity, D dioptre. *The correction target of ortho-k lenses was defined as the sum of the spherical power plus half of the cylindrical power of the lens.
As shown in Table 1, the ortho-k lens wearing rate was 1.4% in the total population and 3.1% in the potential population. The ortho-k lens wearing was concentrated in certain age groups, with the highest rate appearing at the age of 10 years (2.7% in the total cohort and 5.8% in the potential population) and a gradual decrease in wearing rate in children older or younger than 10 years. Children aged 9–13 years showed a higher wearing rate than other age groups in the potential population (χ2 = 88.25, p < 0.001, χ2 test).
Factors associated with ortho-k lens use
The comparisons between ortho-k lens users and non-users are shown in Table 2. The differences in sex, age, height, weight, BMI, academic stage, parental myopia, and age at initiation of refractive correction between ortho-k lens users and non-users were statistically significant (p < 0.001 for all). No significant differences were observed between the two groups in premature delivery (p = 0.697), and sleeping duration on school days (p = 0.320).
Considering the results of univariate analysis and the clinical significance of variables, sex, age, BMI, age at initiation of refractive correction, and parental myopia were included in the binary logistic regression model with weather wearing ortho-k lens or not as dependent variable [Fig. 3a]. It is indicated that starting refractive correction at ≤12 years of age (odds ratio [OR] 1.75, 95% confidence interval [CI] 1.31–2.33, p < 0.001) and parental myopia (either: OR 2.09, 95% CI: 1.58–2.75, p < 0.001; both: OR 3.94, 95% CI: 3.04–5.11, p < 0.001) were positively associated with ortho-k lens use, while age (OR 0.91, 95% CI: 0.88–0.95, p < 0.001) and obesity (OR 0.48, 95% CI: 0.35–0.66, p < 0.001) were negatively associated with ortho-k lens use. Sex was not independently related to ortho-k lens use (p = 0.105).

Forest plots of binary logistic regression model and its results with ortho-k lens use (a) and unsatisfactory CVA (b) as dependent variables respectively. The selection of variables considered both statistical results and clinical significance. BMI body mass index, D dioptre, CVA corrected visual acuity. *P < 0.05 was considered statistically significant. aThe correction target of ortho-k lenses was defined as the sum of the spherical power plus half of the cylindrical power of the lens.
Unsatisfactory CVA in ortho-k lens users and associated factors
The distribution of daytime CVA in ortho-k lens users is shown in Fig. 2. Of the 1021 ortho-k lens users, 127 participants (12.4%) had a CVA of ≥0.3 in the right eye. Multiple regression analysis of factors associated with unsatisfactory CVA was performed and the results indicated that correction target (p < 0.001) and sleeping time on school days (p = 0.008) were independently associated with a CVA of ≥0.3, while no significant differences were observed in other factors (p > 0.05) (Supplementary Table 1). In the binary logistic regression model with unsatisfactory CVA as dependent variable [Fig. 3b], SE ≤ − 3.0 D (OR 2.05, 95% CI: 1.38–3.05, p < 0.001) and a sleeping duration of ≤6 h on school days (OR 4.19, 95% CI: 2.03–8.64, p < 0.001) were independently associated with an unsatisfactory CVA. As shown in Fig. 2, 4.1% of children who wore ortho-k lenses slept for no more than 6 h.
Discussion
To our knowledge, this is the first report to analyse the use rate of ortho-k lenses in school-aged children and adolescents. Our study found that a certain proportion of children and adolescents chose to wear ortho-k lenses, some of which had unsatisfactory daytime vision. Age, BMI, age at initiation of refractive correction, and parental myopia were independently associated with ortho-k lens use.
In our study, ortho-k lenses had a use rate of 1.4% in the total cohort and 3.1% in children with myopia. In contact lens users, Morgan et al. reported an ortho-k lens use rate of 1.40% for people of all ages in several countries including China from 2004 to 2017 [23]. These results indicate a relatively low ortho-k lens use rate including in the myopic population. Optometry of ortho-k lens and its follow-ups require the support of experienced clinical doctors, adequate medical conditions, and good adherence of ortho-k lens users [24]. Moreover, adverse effects have been reported, which may be related to corneal hypoxia caused by use during sleep [18, 25, 26]. The features mentioned above may be some of the reasons why ortho-k lenses are not widely used.
Age and the age at initiation of refractive correction are independently associated with ortho-k lens use. In our study, junior high school children comprised the largest proportion of ortho-k lens users, followed by primary school students and senior high school children. This conclusion is similar to the results of Morgan et al., who reported that a high proportion of children aged 13–17 years and 6–12 years used ortho-k lenses [23]. Considering that ortho-k lenses are usually worn by children over the age of 8 years and the onset of myopia mostly appears at 9–10 years of age, our results are consistent with the clinical situation. As reported, an early age of myopia onset suggests a high risk of high myopia, and the likelihood of progressing to high myopia is high in children diagnosed with myopia before the age of 12 years [3, 27, 28]. Thus, it is gratifying to see that children who start refractive correction early are more likely to use ortho-k lenses. In addition, since the progression of childhood myopia slows with age [29,30,31], younger children may also benefit more from ortho-k lenses for myopia control than older children [32,33,34].
Parental myopia was independently associated with the choice to use ortho-k lenses (either: OR 2.09; both: OR 3.94). The understanding and attitude of parents toward myopia may influence the methods used to correct myopia, as well as the treatment compliance of children. Previous studies have found that parents adopt a proactive role when deciding on myopia treatment [24, 35], and parents with myopia may pay more attention to myopia development and control in their children than emmetropic parents [36]. Studies have also reported that the majority of parents obtain information on ortho-k through word of mouth or from ophthalmologists [32, 37], which may suggest a lack of public knowledge about myopia and its available treatments.
Our study found that children with obesity were less likely to wear ortho-k lenses than children with a healthy BMI, which was seldom mentioned in previous studies. Childhood obesity is often related to less physical activities, so children with a higher BMI may have less need to be lens-free during the day [38]. Previous studies have indicated that family income is negatively correlated with BMI in children. In addition, childhood temperament, especially lack of self-regulation and dissatisfaction with limitations, is considered to be an important predictor of obesity in children [39, 40]. Therefore, we speculate that children with a higher BMI are less likely to use ortho-k lenses due to less need, the economic conditions of their families and their lower self-management ability. Sex was not independently associated with ortho-k lens use, although girls were considered more likely to wear ortho-k lenses than boys in the univariable analysis. Sex and BMI are potential associated factors; thus, the findings presented here might provide some clues for future studies.
In our study, 12.4% of the participants who used ortho-k lenses had a CVA of ≥0.3, and ortho-k lens use was associated with a high lens degree and lack of sleep. Ortho-k lens changes an eye’s refractive state by flattening the cornea. Unsatisfactory vision is associated with higher correction target, possibly because the eye has limited deformability and is more likely to return to its original shape. Unsatisfactory vision potentially related to insufficient sleep time may also be related to insufficient deformation. Previous studies have rarely involved the influence of sleep time on the effect of ortho-k lens. Chen et al. studied the factors influencing the effect of ortho-k lens on the control of myopia progression and did not find significant correlation, but all children participants in the study had a sleeping time ≥8 h [41]. Previous studies have shown that daytime vision can reach 0.0 after ortho-k lens use and remain stable for longer than 6 months [34, 42,43,44]. The difference in daytime vision may be due to the fact that our study measured visual acuity in random examination, rather than under close follow-up in clinical trials. Chang et al. found that the compliance of children and their guardians decreased as the follow-up interval lengthened. Lack of compliance included not paying attention to lens hygiene and not examining or replacing lenses in a timely manner [35]. Therefore, ortho-k lenses should be used more specifically for children who meet the indications or with the need to take off glasses during daytime. And to ensure a better therapeutic effect and reduce the risk of adverse reactions, ophthalmologists should conduct more rigorous examination of indications and perform detailed examinations and inquiries during follow-ups in clinical practice, as well as adequately educate the children and their guardians. For children who are not suitable for ortho-k, other means of controlling myopia progression should be chosen instead, which is mentioned below. As for the unsatisfactory daytime vision potentially related to a short duration of sleep, some ophthalmologists suggest that children start to wear ortho-k lenses in the evening to make up the time, which might provide clues for future studies and clinical practices.
Several strategies have been introduced in China since 2016 to promote the early screening and correction of myopia in children. Visual acuity and autorefraction screening are performed at school in students’ annual physical examinations. Children who may be newly-developed myopia or have a rapid progression of myopia progress are directed to hospitals for detailed refractive examinations and treatments. Meanwhile, different myopia control measures have provided more choices for children with different circumstances. Low concentration atropine and orthokeratology have been included as appropriate technical in guidelines for myopia control in China, while newer measures such as peripheral defocus contact lens or ophthalmic lens are also available [45, 46]. Although the indications and selection of different measures remain to be summarized by the results of clinical trials, this is a step forward for myopia interventions toward routine treatment and wide application.
This study has several limitations that should be noted. First, the refractive status in this study was obtained without cycloplegia, which could result in overestimation of the potential population and correspondingly lead to a lower rate of ortho-k use. Actually, due to practical limitations, it is difficult for us to use cycloplegic optometry for all children in large-scale school examinations. Meta-analysis and study on children aged 4 to 15 showed that, non-cycloplegia refraction resulted in a mean SE difference of −0.60D compared to cycloplegia, with greater differences observed in younger participants and in eyes with more hyperopic refraction degree [47, 48]. Therefore, the influence of non-cycloplegia data on this study could be limited. Second, we lack information about the pharmaceutical agents they used, like atropine, which may affect our analysis of the results. Since atropine is not regularly used as a correction method and the usage and dosage information could be complicated to collect, we failed to collect the information of myopia interventions other than optical means. Nevertheless, we believe that the results of this study could still provide adequate information on the characteristic of ortho-k lens wearers. Third, since ortho-k lens could both control the progression of myopia and be a method of correction, the actual purpose of children wearing lenses may affect the results, which should be distinguished. It is a pity that due to the limitation of the method and sample size, this detail question was not included in our questionnaire, which is also one of limitations in this study and could be studied further. Fourth, this is a cross-sectional study; thus, no causal relationship can be concluded. The information on children and their families was collected using questionnaires, which carry a risk of recall bias. Fifth, our study lacks information about parental education, family economics, and other factors that may be associated with the choice to use ortho-k lenses and daytime vision. Sixth, the time of the examinations could not be unified; thus, the influence of examination time on CVA cannot be completely excluded. However, according to previous research results, visual acuity did not change significantly from 1 h to 10 h after removal of ortho-k lenses [44].
In conclusion, a certain proportion of children and adolescents in Shanghai chose to wear ortho-k lenses. Some of these children and adolescents exhibited a decline in daytime vision. Ortho-k lens is an effective method for myopia control, but for reasons related to safety and efficacy, examinations, health education and clinical follow-up of children who use these lenses must be strengthened. Public education is imperative so that the awareness of myopia control is increased in parents of young children and to help parents make informed decisions.
Summary
What was known before
-
The efficacy and safety of ortho-k lenses have been well studied.
What this study adds
-
A certain proportion of children and adolescents chose to wear ortho-k lenses. Some of the users had unsatisfactory daytime vision. Age, BMI, age at initiation of refractive correction, and parental myopia were independently associated with ortho-k lens use.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Xiang ZY, Zou HD. Recent epidemiology study data of myopia. J Ophthalmol. 2020;2020:4395278.
Dolgin E. The myopia boom. Nature. 2015;519:276–8.
Morgan IG, French AN, Ashby RS, Guo X, Ding X, He M, et al. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018;62:134–49.
Chen M, Wu A, Zhang L, Wang W, Chen X, Yu X, et al. The increasing prevalence of myopia and high myopia among high school students in Fenghua city, eastern China: a 15-year population-based survey. BMC Ophthalmol. 2018;18:159.
Yotsukura E, Torii H, Inokuchi M, Tokumura M, Uchino M, Nakamura K, et al. Current prevalence of myopia and association of myopia with environmental factors among schoolchildren in Japan. JAMA Ophthalmol. 2019;137:1233–9.
Rozema J, Dankert S, Iribarren R, Lanca C, Saw SM. Axial growth and lens power loss at myopia onset in Singaporean children. Invest Ophthalmol Vis Sci. 2019;60:3091–9.
Mutti DO, Hayes JR, Mitchell GL, Jones LA, Moeschberger ML, Cotter SA, et al. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007;48:2510–9.
Ikuno Y. Overview of the complications of high myopia. Retina. 2017;37:2347–51.
Haarman AEG, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61:49.
Ohsugi H, Ikuno Y, Shoujou T, Oshima K, Ohsugi E, Tabuchi H. Axial length changes in highly myopic eyes and influence of myopic macular complications in Japanese adults. PLoS One. 2017;12:e0180851.
Tideman JW, Snabel MC, Tedja MS, van Rijn GA, Wong KT, Kuijpers RW, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016;134:1355–63.
Huang J, Wen D, Wang Q, McAlinden C, Flitcroft I, Chen H, et al. Efficacy comparison of 16 interventions for myopia control in children: a network meta-analysis. Ophthalmology. 2016;123:697–708.
Tsai HR, Wang JH, Chiu CJ. Effect of orthokeratology on anisometropia control: a meta-analysis. J Formos Med Assoc. 2021;120:2120–7.
Li SM, Kang MT, Wu SS, Liu LR, Li H, Chen Z, et al. Efficacy, safety and acceptability of orthokeratology on slowing axial elongation in myopic children by meta-analysis. Curr Eye Res. 2016;41:600–8.
Si JK, Tang K, Bi HS, Guo DD, Guo JG, Wang XR. Orthokeratology for myopia control: a meta-analysis. Optom Vis Sci. 2015;92:252–7.
Sun Y, Xu F, Zhang T, Liu M, Wang D, Chen Y, et al. Orthokeratology to control myopia progression: a meta-analysis. PLoS One. 2015;10:e0124535.
Li X, Friedman IB, Medow NB, Zhang C. Update on orthokeratology in managing progressive myopia in children: efficacy, mechanisms, and concerns. J Pediatr Ophthalmol Strabismus. 2017;54:142–8.
Lipson MJ, Brooks MM, Koffler BH. The role of orthokeratology in myopia control: a review. Eye Contact Lens. 2018;44:224–30.
He X, Zhao R, Sankaridurg P, Zhu J, Naduvilath T, Ma Y, et al. Design and methodology of the Shanghai child and adolescent large-scale eye study (SCALE). Clin Exp Ophthalmol. 2018;46:329–38.
World report on vision. Geneva: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO.
Song P, Li X, Gasevic D, Flores AB, Yu Z. BMI, waist circumference reference values for Chinese school-aged children and adolescents. Int J Environ Res Public Health. 2016;13:589.
Ma J, Wang Z, Song Y, Hu P, Zhang B. BMI percentile curves for Chinese children aged 7–18 years, in comparison with the WHO and the US Centers for Disease Control and Prevention references. Public Health Nutr. 2010;13:1990–6.
Morgan PB, Efron N, Woods CA, Santodomingo-Rubido J. International survey of orthokeratology contact lens fitting. Cont Lens Anterior Eye. 2019;42:450–4.
Chang LC, Li FJ, Sun CC, Liao LL. Trajectories of myopia control and orthokeratology compliance among parents with myopic children. Cont Lens Anterior Eye. 2021;44:101360.
Morgan PB, Murphy PJ, Gifford KL, Gifford P, Golebiowski B, Johnson L, et al. CLEAR - Effect of contact lens materials and designs on the anatomy and physiology of the eye. Cont Lens Anterior Eye. 2021;44:192–219.
Liu YM, Xie P. The safety of orthokeratology-a systematic review. Eye Contact Lens. 2016;42:35–42.
Guo K, Yang DY, Wang Y, Yang XR, Jing XX, Guo YY, et al. Prevalence of myopia in schoolchildren in Ejina: the Gobi Desert children eye study. Invest Ophthalmol Vis Sci. 2015;56:1769–74.
Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singap. 2004;33:27–33.
Donovan L, Sankaridurg P, Ho A, Naduvilath T, Smith EL 3rd, Holden BA. Myopia progression rates in urban children wearing single-vision spectacles. Optom Vis Sci. 2012;89:27–32.
Hyman L, Gwiazda J, Hussein M, Norton TT, Wang Y, Marsh-Tootle W, et al. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch Ophthalmol. 2005;123:977–87.
Verkicharla PK, Kammari P, Das AV. Myopia progression varies with age and severity of myopia. PLoS One. 2020;15:e0241759.
Wang X, Yang B, Liu L, Cho P. Analysis of parental decisions to use orthokeratology for myopia control in successful wearers. Ophthalmic Physiol Opt. 2021;41:3–12.
Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Invest Ophthalmol Vis Sci. 2012;53:7077–85.
VanderVeen DK, Kraker RT, Pineles SL, Hutchinson AK, Wilson LB, Galvin JA, et al. Use of orthokeratology for the prevention of myopic progression in children: a report by the American Academy of Ophthalmology. Ophthalmology. 2019;126:623–36.
Wang J, Liu L, Boost M, Yap M, Cho P. Risk factors associated with contamination of orthokeratology lens cases. Cont Lens Anterior Eye. 2020;43:178–84.
McCrann S, Flitcroft I, Lalor K, Butler J, Bush A, Loughman J. Parental attitudes to myopia: a key agent of change for myopia control? Ophthalmic Physiol Opt. 2018;38:298–308.
Cheung SW, Lam C, Cho P. Parents’ knowledge and perspective of optical methods for myopia control in children. Optom Vis Sci. 2014;91:634–41.
Hébert JJ, Sénéchal M, Fairchild T, Møller NC, Klakk H, Wedderkopp N. Developmental trajectories of body mass index, waist circumference, and aerobic fitness in youth: implications for physical activity guideline recommendations (CHAMPS Study-DK). Sports Med. 2020;50:2253–61.
Brown CL, Halvorson EE, Cohen GM, Lazorick S, Skelton JA. Addressing childhood obesity: opportunities for prevention. Pediatr Clin North Am. 2015;62:1241–61.
Ji M, Tang A, Zhang Y, Zou J, Zhou G, Deng J, et al. The relationship between obesity, sleep and physical activity in Chinese preschool children. Int J Environ Res Public Health. 2018;15:527.
Chen X, Xiong Y, Liu F, Wang J, Yang B, Liu L. Factors determining the myopia control effect of an orthokeratology lens: A two-year multi-level model. Ophthalmic Physiol Opt. 2022;42:786–96.
Singh K, Bhattacharyya M, Goel A, Arora R, Gotmare N, Aggarwal H. Orthokeratology in moderate myopia: a study of predictability and safety. J Ophthalmic Vis Res. 2020;15:210–7.
Yang B, Ma X, Liu L, Cho P. Vision-related quality of life of Chinese children undergoing orthokeratology treatment compared to single vision spectacles. Cont Lens Anterior Eye. 2021;44:101350.
Stillitano I, Schor P, Lipener C, Hofling-Lima AL. Stability of wavefront aberrations during the daytime after 6 months of overnight orthokeratology corneal reshaping. J Refract Surg. 2007;23:978–83.
Ruiz-Pomeda A, Villa-Collar C. Slowing the progression of myopia in children with the misight contact lens: a narrative review of the evidence. Ophthalmol Ther. 2020;9:783–95.
Lam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM, Hasegawa K, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104:363–8.
Wilson S, Ctori I, Shah R, Suttle C, Conway ML. Systematic review and meta-analysis on the agreement of non-cycloplegic and cycloplegic refraction in children. Ophthalmic Physiol Opt. 2022;42:1276–88.
Sankaridurg P, He X, Naduvilath T, Lv M, Ho A, Smith E 3rd, et al. Comparison of noncycloplegic and cycloplegic autorefraction in categorizing refractive error data in children. Acta Ophthalmol. 2017;95:e633–e640.
Funding
This study was supported by National Key R&D Program of China (No.2021YFC2702100, No.2021YFC2702104, No.2019YFC0840607), Excellent Discipline Leader Cultivation Program of Shanghai Three Year Action Plan on Strengthening Public Health System Construction (No.GWV-10.2-XD09) and National Natural Science Foundation of China (No.81900911, No.82003562). The sponsor or funding organization had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
WZ, XH, and XX designed this study. WZ, JC, JW, JY, and HX collected and interpreted the data. WZ and JC performed statistical analysis. WZ drafted the manuscript. XH, KL, JW, and XX obtained funding for this study. XH and XX supervised this study. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhao, W., Wang, J., Chen, J. et al. The rate of orthokeratology lens use and associated factors in 33,280 children and adolescents with myopia: a cross-sectional study from Shanghai. Eye 37, 3263–3270 (2023). https://doi.org/10.1038/s41433-023-02503-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-023-02503-1
