
Abstract
Background/objectives
To assess the influence of patient age on visual outcomes in eyes with diffractive multifocal intraocular lenses (IOLs)
Subjects/methods
Based on age, we classified eyes with diffractive multifocal IOL into four groups: u50 (under 50 years old), 50s (50–59 years), 60s, and 70s. Corrected distance (CD), distance-corrected near (DCN) visual acuity (VA), and defocus curve were measured postoperatively. Using an “area-of-focus” metric, the distant, intermediate, and near area-of-focus (AoF) were also measured. These postoperative results were compared between the age groups.
Results
At 3 months after surgery, the CDVA in the u50, 50s, 60s, and 70s groups were −0.18, −0.16, −0.14, and −0.10 logMAR, respectively. The 70s CDVA was significantly worse than the u50 and 50s groups (P = 0.002, P = 0.049). The DCNVA in the u50, 50s, 60s, and 70s were 0.01, 0.03, 0.03, and 0.08 logMAR. DCNVA in the 70s group was significantly worse than that in the u50 and 60s groups (P = 0.008 and P = 0.019, respectively). The near AoF was smaller in the 70s than in the u50 and 50s groups (P = 0.040, P = 0.047). In both the intermediate and distant AoFs, there was no significant difference between the four age groups. A steep decline in near AoF was observed in patients over 60 years of age.
Conclusions
The CDVA, DCNVA, and near AoF declined with patient age in eyes with diffractive multifocal IOL. The near AoF showed a drastic decline over 60 years.
Similar content being viewed by others


Introduction
The implantation of multifocal intraocular lens (IOL) provides both distant and near vision and achieves spectacle independence with high patient satisfaction. Many previous studies have already shown the effectiveness of multifocal IOL implantation after cataract extraction [1,2,3,4].
To achieve higher patient satisfaction, some complications and factors after multifocal IOL implantation remains to be resolved. Residual refractive error [5, 6], pupil diameter [6, 7], posterior capsule opacification (PCO) [6, 8], higher-order aberrations [9], and dry eyes [10] play important roles in the postoperative visual performance of multifocal IOLs. However, only few studies have discussed whether the patient’s age affects the postoperative visual outcomes of multifocal IOLs. Yoshino et al. [11] first approached this issue and demonstrated that the corrected distance (CD) and near visual acuity (VA) and contrast sensitivity were worse in older patients than in younger patients. Because the number of cataract patients requesting multifocal IOL implantation is expected to increase in the future, further studies investigating the connection between aging and multifocal IOL are needed. To the best of our knowledge, it remains unclear how and to what extent patient age affects the defocus curve in eyes with a multifocal IOL.
Herein, the “area-of-focus (AoF)” analysis [12] was used for the comprehensive assessment of the defocus curves. We classified cataract patients with diffractive multifocal IOLs into four age groups and assessed the influence of patient age on visual outcomes using defocus curves as well as distant and near VA. As a control, patients undergoing cataract extraction with monofocal IOL implantation were also enrolled. We found that aging affected the defocus curve as well as the CD and distance-corrected near (DCN) VA in eyes with multifocal IOL.
Subjects and methods
Patients
We retrospectively reviewed a consecutive series of patients with cataracts who underwent cataract surgery with diffractive multifocal IOL implantation from August 2009 to November 2015 at the Jikei Hospital, Tokyo, Japan. The criterion for preoperative corneal astigmatism was 1.50 diopter (D) or below. Patients with ocular diseases that are likely to affect postoperative visual function (such as macular disease and glaucoma), those with a history of ophthalmic surgery, and those with severe intraoperative or postoperative complications were excluded from this study. All patients were given a thorough explanation of the risks and benefits of cataract surgery, and informed consent was obtained. This retrospective study was approved by the Ethical Committee of the Jikei University School of Medicine (approval number: 25–169 [7304]), and the study design followed the tenets of the Declaration of Helsinki.
Based on age, the patients with multifocal IOLs were divided into four groups: u50 (<50 years), 50s (50–59 years), 60s (60–69 years), and 70s (70–79 years). As a control, we enrolled patients who underwent cataract surgery with monofocal IOL implantation from May 2017 to November 2017, and stratified them into the following groups: u50 (<50 years), 50s (50–59 years), 60s (60–69 years), 70s (70–79 years), and 80s/90s (80–99 years).
Preoperative and postoperative examination
Axial length was measured before surgery using IOLMaster version 5, IOLMaster 500, or IOLMaster 700 (Carl Zeiss Meditec). The SRK/T formula was used to select IOL power. The power of the multifocal IOL was selected for the emmetropia. Monofocal IOL power was selected for emmetropia or moderate myopia. VA was measured at one and 3 months after surgery. The CDVA was measured using a Landolt C chart at a distance of 5 m. The DCNVA was measured using a Landolt C chart at a distance of 30 cm. Defocus curves were measured at 3 months after surgery using a Landolt C chart at 5-m distance in monocular condition with corrected postoperative manifest refraction. Additional lenses were introduced in increments of 0.50 D, and the VA was recorded at each defocus level. The range of defocus was −5.00 to +2.00 D. Corneal aberrations were also measured with OPD-Scan II (Nidek Co., Ltd) for a 4-mm pupil diameter at 1 month. Total higher-order, total coma, total trefoil, and total spherical aberrations were obtained in this study. A postoperative questionnaire containing the usage of reading glasses and a satisfaction survey was administered 3 months after cataract surgery.
Surgical technique
We used a Tecnis ZMA00 or Tecnis ZMB00 diffractive multifocal IOL (Abbott Medical Optics Inc.). A Tecnis PCB00V (Abbott Medical Optics Inc.) was used as a control. All surgeries were performed by two ophthalmologists (T. O. for multifocal IOL and R. T. for monofocal IOL). With a 2.4-mm temporal corneal incision or superior sclerocorneal incision, the cataract was removed by phacoemulsification and aspiration under topical anesthesia. Thereafter, the IOL was implanted inside the lens capsule using an injector.
“Area-of-focus” method
To evaluate the defocus curve, we used modified “AoF” metrics (Supplementary Fig. 1), which was based on the technique reported by Buckhurst et al. [12] Fifteen points, recorded at each defocus level between −5.00 and +2.00 D, were connected with a straight line, which was defined as the defocus curve. Corresponding with the visual standards for driving in Europe and the United States, the cutoff value of VA was defined as +0.30 logarithmic minimum angle of resolution (logMAR). The AoF (logMAR/m), which was surrounded by a defocus curve and +0.30 LogMAR horizontal line, was divided into three zones: distant, intermediate, and near AoFs. Distant AoF was defined as a value between +2.00 and −0.50 D. Intermediate AoFs was defined as a value between −0.50 and −2.00 D, while near AoF was defined as a value between −2.00 and −5.00 D.
Statistical analysis
Statistical analysis was performed using the statistical program R (version 4.0.4) (available in the public domain http://r-project.org). All values are presented as mean ± standard deviation. For statistical analysis, the decimal VA obtained using the Landolt C chart was converted to logMAR values. To analyse the difference in postoperative VA, AoFs, or corneal aberrations between age groups, the Steel–Dwass nonparametric test was used. The Mann–Whitney U test was used to compare the VA between two groups. Spearman’s rank correlation coefficient was used to determine the relationship between two variables. The relationship between AoF and patient age was visualized using a smoothing spline. Statistical significance was set at P < 0.05.
Results
This study enrolled 104 eyes of 67 patients with age ranging from 19 to 77 years (35 men, 32 women; 59.8 years ± 13.0) who underwent cataract extraction with a diffractive multifocal IOL implantation. Based on age, we classified these patients into four groups: u50 (19 eyes), 50s (13 eyes), 60s (53 eyes), and 70s (19 eyes) (Table 1).
Visual acuity
At 1 month postoperatively, the CDVA was significantly worse in the 70s group than in the 60s, 50s, and u50 groups (all P < 0.001) (Fig. 1A). At 3 months postoperatively, the CDVA was significantly worse in the 70s group than in the 50s and u50 groups (P = 0.049 and P = 0.002, respectively). There was a significant but weakly positive relationship between the CDVA at postoperative 1 month and patient age (R = 0.40, P < 0.001), and between the CDVA at postoperative 3 months and patient age (R = 0.31, P = 0.001). CDVA in the 70s group was better at 3 months than at 1 month postoperatively (P = 0.032). The DCNVA at postoperative 1 month was significantly worse in the 70s group than in the 60s, 50s, and u50 groups (P = 0.007; P = 0.003; P = 0.013, respectively) (Fig. 1B). At 3 months postoperatively, the DCNVA was significantly worse in the 70s group than in the 60s and u50 groups (P = 0.019 and P = 0.008, respectively). There was a significant weak positive relationship between the DCNVA at 1 month and patient age (R = 0.23, P = 0.021) and between the DCNVA at 3 months and patient age (R = 0.25, P = 0.011). In DCNVA, there was no significant change from 1 month to 3 months in each age group.

CDVA (A) and DCNVA (B) were measured 1 and 3 months after the multifocal IOL implantation. Both CDVA and DCNVA tended to deteriorate with patient age. The CDVA at 70s was significantly better at 3 months than at 1 month. “1M” and “3M” indicate 1 month after surgery and 3 months after surgery, respectively. Asterisks indicate statistical significance.
Defocus curve and area-of-focus
Defocus curves for the four age groups are shown in Fig. 2A. All age groups showed a double-peak curve. Two peaks were observed at 0 D and −3.0 D. The lowest point between the two peaks was −1.5 D. Distant, intermediate, and near AoFs were measured for each eye (Fig. 2B). The near AoF was smaller in the 70s than in the 50s and u50 groups (P = 0.047 and P = 0.040, respectively). There was a weak negative correlation between near AoF and patient age (R = −0.22, P = 0.023), while there was no significant difference in both distant and intermediate AoFs between the four age groups. Further, we illustrated nonlinear relationships between AoFs of multifocal IOLs and patient age using smoothing splines (Fig. 3A, B, C). The splines in both distant and intermediate AoFs were nearly flat, which suggested that the two AoFs did not change with patient age. Conversely, the near AoF had a steep decline for over 60 years.

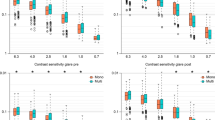
A Defocus curves of four age groups are shown. All age groups had a double-peak curve. Two peaks were at 0 D and −3.0 D. The lowest point between two peaks was at −1.5 D. B The distant, intermediate, and near AoF of four age groups were shown. The near AoF was significantly smaller in the 70s than in the 50s and u50 (P = 0.047 and P = 0.040). There was no significant difference in both the distant and intermediate AoFs between four age groups. Asterisks indicate statistical significance. DIST distant AoF, INT intermediate AoF, NEAR near AoF.

Patients were plotted based on their age and AoF values. Nonlinear relationships between AoF and patient age are shown using a smoothing spline. The dotted lines represent the 95% confidence intervals. A, B The splines in both distant AoF and intermediate AoF are nearly flat, which indicated that these two AoFs did not change with patient age. C The near AoF had a decline over 60 years. D The splines of distant AoF in eyes with monofocal IOL had a flat trend under 60 years and showed a mild linear decline around over 60.
Six eyes of six patients with near AoF of <0.25 logMAR/m are shown (Supplementary Table 1). In all six patients, the same diffractive multifocal IOL was inserted into the contralateral eye at approximately the same time. Although a response to the questionnaire was not available in case #2, postoperative satisfaction was good in the other cases. There were no patients who required reading glasses routinely.
Corneal higher-order aberrations
The relationships between the corneal higher-order aberrations (total higher-order, total coma, total trefoil, and total spherical aberrations) and the three AoFs are shown using correlation coefficients (Table 2). The intermediate AoF had weak positive correlations with total higher-order, total coma, and total trefoil aberrations (R = 0.33, P < 0.001; R = 0.21, P = 0.032; R = 0.29, P < 0.001, respectively), but not with total spherical aberration. Distant and near AoFs were not significantly correlated with these corneal higher-order aberrations. Total higher-order and trefoil aberrations slightly increased with patient age (R = 0.29 and 0.37, P = 0.002 and <0.001, respectively) (Supplementary Fig. 2). Although total coma aberration in the 70s group was higher than that in the u50 and 60s groups, there was no significant correlation between total coma aberration and patient age (R = 0.17, P = 0.09). Total spherical aberration was also not significantly correlated with patient age (R = 0.07, P = 0.45).
Visual outcomes in eyes with a monofocal IOL
We also enrolled patients with monofocal IOLs as controls. Ninety-one eyes of 60 patients (37 men, 23 women; 69.2 years ± 12.6) were enrolled. The eyes were divided into five age groups: u50 (10 eyes), 50s (11 eyes), 60s (18 eyes), 70s (30 eyes), and 80s/90s (22 eyes). The demographics of the five groups, including postoperative visual outcomes, are shown in Supplementary Table 2. The distant AoF was smaller in the 80s/90s groups than in the 70s, 50s, and u50 groups (P = 0.028, P = 0.009, and P = 0.038, respectively). There was a weak negative correlation between the distant AoF and patient age (R = −0.37, P < 0.001). The smoothing spline shows the relationship between the distant AoF and patient age (Fig. 3D). The spline was flat at ~60 years of age. Over 60 years, the distant AoF showed a mild linear decline.
Discussion
To verify the effect of patient age on visual outcomes in eyes with diffractive multifocal IOLs, we classified cataract patients into four age groups and postoperatively measured defocus curves as well as distant and near VA for each patient. We used the modified “AoF” method to comprehensively assess the defocus curve. As a result, eyes with multifocal IOL showed clinically satisfactory CDVA, DCNVA, and AoF across all classified groups. However, we found that near AoF, CDVA, and DCNVA were negatively correlated with patient age. The near AoF had a steep decline over 60 years. To the best of our knowledge, this study is the first to show that the postoperative defocus curve in patients with multifocal IOL could be affected by aging.
Although our results suggest age-related changes in visual performance, aging also causes changes in ophthalmic optics based on higher-order aberrations and pupil size. In addition, PCO and ocular surface disease, including dry eyes, which potentially have a great impact on our results, should be adequately considered. Zheleznyak et al. [9] reported that higher-order aberrations had a negative effect on the through-focus image quality of multifocal IOLs. In our case, there was no negative correlation between corneal higher-order aberrations and visual outcomes, although some higher-order aberrations increased with age. Pupil size may also have affected our results. Ouchi and Shiba [7] reported that small pupils in eyes with diffractive multifocal IOLs affected only contrast sensitivity, but not corrected VA and the defocus curve. In this study, we did not verify the effect of pupil size on postoperative outcomes, which was a limitation of our study. Regarding PCO, there were no cases of PCO in any age decade during the study period. In addition, there were no cases of ocular surface damage or complaints of dry eye symptoms.
This study revealed a remarkable decline of near AoF over 60 years and delayed postoperative CDVA recovery in the elderly. Visual perceptual learning (VPL), which is a permanent improvement of visual performance with repeated visual experience [13, 14], might explain this finding. Patients with multifocal IOLs simultaneously receive different images on the retina. After IOL implantation, they need to adapt to the dramatic changes in the visual environment [5]. Some studies have already indicated the relationship between VPL, neuroadaptation, and postoperative performance of multifocal IOLs [15,16,17,18,19]. Chang et al. [20, 21] demonstrated that aging affected the ability to filter out unimportant visual signals, resulting in age-related decline of stability in VPL. Based on these findings and our findings, we speculate that it is difficult for older patients to accurately discriminate the different images on the retina caused by the multifocal IOL.
We believe that the age-related differences in performance of multifocal IOLs would not prohibit the implantation of multifocal IOL in older patients, because the CDVA of −0.10 logMAR and the DCNVA of 0.08 logMAR in the 70s group were considered clinically satisfactory. The postoperative questionnaire also showed that six eyes with the lowest near AoF could keep high level of visual satisfaction. However, we would recommend that cataract surgeons pay close attention to the finding that elderly patients have a potentially worse near vision risk than young patients. A more detailed preoperative description, including information on postoperative visual function, is important when using multifocal IOL in patients aged 70 years or above. In addition, a thorough examination of retinal diseases that may affect postoperative visual function must be conducted.
This study had the following limitations. First, we did not verify the effect of pupil size on postoperative outcomes, as previously mentioned. Second, the sample size was small in the u50 (19 eyes), 50s (13 eyes), and 70s (19 eyes). In particular, the postoperative performance of patients aged >75 years has not been fully elucidated. Therefore, a large-scale study is required.
In conclusion, the CDVA, DCNVA, and near AoF in eyes with a diffractive multifocal IOL declined with patient age. The near AoF had a remarkable decline over 60 years. Higher-order aberrations had no impact on the decline near AoF. VPL could be one of the main factors leading to age-related deterioration of postoperative visual function in eyes with diffractive multifocal IOL. A thorough preoperative description and ophthalmic examination should be conducted, although patients over 70 years of age could achieve satisfactory visual outcomes in our study.
Summary
What was known before
-
Patient age affects the postoperative outcome of multifocal intraocular lenses (MIOLs) implantation. It is known that postoperative corrected VA and contrast sensitivity were worse in elderly than in young, but to what extent the defocus curve is affected by patient age remains unclear.
What this study adds
-
Patient age is negatively and nonlinearly associated with the performance of defocus curve at near distance, showing a drastic decline over 60 years. Although postoperative satisfaction of MIOL implantations is high, even in cases with poor near zone outcome, adequate preoperative description and ophthalmic examination should be provided, especially for elderly patients.
References
Leyland M, Zinicola E. Multifocal versus monofocal intraocular lenses in cataract surgery: a systematic review. Ophthalmology. 2003;110:1789–98.
Schmickler S, Bautista CP, Goes F, Shah S, Wolffsohn JS. Clinical evaluation of a multifocal aspheric diffractive intraocular lens. Br J Ophthalmol. 2013;97:1560–4.
Agresta B, Knorz MC, Kohnen T, Donatti C, Jackson D. Distance and near visual acuity improvement after implantation of multifocal intraocular lenses in cataract patients with presbyopia: a systematic review. J Refract Surg. 2012;28:426–35.
Rasp M, Bachernegg A, Seyeddain O, Ruckhofer J, Emesz M, Stoiber J, et al. Bilateral reading performance of 4 multifocal intraocular lens models and a monofocal intraocular lens under bright lighting conditions. J Cataract Refract Surg. 2012;38:1950–61.
Alio JL, Plaza-Puche AB, Fernandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62:611–34.
de Vries NE, Webers CA, Touwslager WR, Bauer NJ, de Brabander J, Berendschot TT, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37:859–65.
Ouchi M, Shiba T. Diffractive multifocal intraocular lens implantation in eyes with a small-diameter pupil. Sci Rep. 2018;8:11686.
Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35:992–7.
Zheleznyak L, Kim MJ, MacRae S, Yoon G. Impact of corneal aberrations on through-focus image quality of presbyopia-correcting intraocular lenses using an adaptive optics bench system. J Cataract Refract Surg. 2012;38:1724–33.
Donnenfeld ED, Solomon R, Roberts CW, Wittpenn JR, McDonald MB, Perry HD. Cyclosporine 0.05% to improve visual outcomes after multifocal intraocular lens implantation. J Cataract Refract Surg. 2010;36:1095–100.
Yoshino M, Bissen-Miyajima H, Minami K. Assessment of whether visual outcomes with diffractive multifocal intraocular lenses vary with patient age. J Cataract Refract Surg. 2013;39:1502–6.
Buckhurst PJ, Wolffsohn JS, Naroo SA, Davies LN, Bhogal GK, Kipioti A, et al. Multifocal intraocular lens differentiation using defocus curves. Investig Ophthalmol Vis Sci. 2012;53:3920–6.
Sagi D. Perceptual learning in vision research. Vis Res. 2011;51:1552–66.
Sasaki Y, Nanez JE, Watanabe T. Advances in visual perceptual learning and plasticity. Nat Rev Neurosci. 2010;11:53–60.
Hayashi K, Hayashi H, Nakao F, Hayashi F. Aging changes in apparent accommodation in eyes with a monofocal intraocular lens. Am J Ophthalmol. 2003;135:432–6.
Kaymak H, Fahle M, Ott G, Mester U. Intraindividual comparison of the effect of training on visual performance with ReSTOR and Tecnis diffractive multifocal IOLs. J Refract Surg. 2008;24:287–93.
Palomino Bautista C, Carmona Gonzalez D, Castillo Gomez A, Bescos JA. Evolution of visual performance in 250 eyes implanted with the Tecnis ZM900 multifocal IOL. Eur J Ophthalmol. 2009;19:762–8.
Goes FJ. Refractive lens exchange with the diffractive multifocal Tecnis ZM900 intraocular lens. J Refract Surg. 2008;24:243–50.
Mester U, Hunold W, Wesendahl T, Kaymak H. Functional outcomes after implantation of Tecnis ZM900 and Array SA40 multifocal intraocular lenses. J Cataract Refract Surg. 2007;33:1033–40.
Chang LH, Shibata K, Andersen GJ, Sasaki Y, Watanabe T. Age-related declines of stability in visual perceptual learning. Curr Biol. 2014;24:2926–9.
Chang LH, Yotsumoto Y, Salat DH, Andersen GJ, Watanabe T, Sasaki Y. Reduction in the retinotopic early visual cortex with normal aging and magnitude of perceptual learning. Neurobiol Aging. 2015;36:315–22.
Author information
Authors and Affiliations
Contributions
RT was responsible for the study design, data collection and analysis, writing of the paper, creation of the figures, and surgeries. HH and SO were responsible for data analysis and paper writing and review. KS was responsible for data collection. TO was responsible for data collection and surgeries. TS and TN were responsible for the study design and review of paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Terauchi, R., Horiguchi, H., Ogawa, S. et al. Age-related visual outcomes in eyes with diffractive multifocal intraocular lenses. Eye 36, 2260–2264 (2022). https://doi.org/10.1038/s41433-021-01854-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01854-x
This article is cited by
-
Comparison of visual outcomes after two types of mix-and-match implanted trifocal extended-depth-of-focus and trifocal intraocular lenses
Graefe's Archive for Clinical and Experimental Ophthalmology (2022)
