
Abstract
Background
To assess the prevalence of myopia and its risk factors in rural school children.
Methods
Children in classes 4–7 of eight randomly selected schools (five government and three private) in rural Haryana, with unaided vision <6/9.5 were screened, their cycloplegic refraction is done, myopes were identified. A questionnaire-based assessment of risk factors was done for myopes and compared with 10% of randomly selected children with normal vision (controls). The prevalence of myopia and its association with risk factors were assessed.
Results
Children screened were 1486 (89.5% coverage). The mean age of children was 11.2 ± 1.5 years with 861 (57.9%) boys. Prevalence of myopia was 6.4% (95% Confidence intervals [CI]: 5.2%, 7.8%). Prevalence was higher among private schools (10.1%) compared to government schools (1.4%) (p < 0.001), and among girls 7.2% (45/625) compared to boys 5.8% (50/861) (p = 0.2786). The mean spherical equivalent refractive error was −1.61D ± 1.32D. The prevalence of high myopia was 1.1% (1/95). There was a 75% unmet need for spectacles. Studying in private school was positively associated with myopia as per our multivariate analysis (p = 0.016). An inverse association was found for time spent outdoors (p = 0.009). Watching television, indoor time, screen time, age, or gender were not found to be statistically significant as risk factors.
Conclusion
The prevalence of myopia is increasing among children of rural areas, especially those in private schools with a strong inverse association with time spent outdoors. Regular screening, lifestyle modification and awareness about modifiable risk factors are essential.
Similar content being viewed by others
Introduction
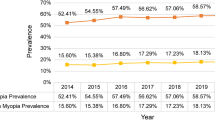
Refractive errors are one of the most common causes of visual impairment worldwide, of which myopia is the most common [1, 2]. Prevalence of myopia varies among countries, ethnic groups and ages [2,3,4]. Variations have also been documented between urban and rural populations [5,6,7]. The previous notion that myopia was less prevalent in rural areas as compared to urban areas in India has been challenged by recent studies [8,9,10]. In rural Indian children, the prevalence of myopia has increased from 4.6% (95% CI, 3.0–6.1) in 1980–2008 to 6.8% (95% CI, 4.2–9.3) in 2009–2019. The percentage increase in myopia prevalence among rural school children was four times compared to their urban counterparts, in the last decade (48% vs 12%) [10].
Uncorrected myopia has significant social, economic, psychological and developmental implications [11]. Also, ineffective preventive methods warrant identifying modifiable risk factors [12, 13]. However, due to differences in cultures, habits, socioeconomic status, educational levels and urbanisation, there remains uncertainty about the exact burden of myopia in rural Indian school-going children and their risk factors.
This study was undertaken to measure the prevalence of myopia and assess its association with behavioural and epidemiological risk factors in rural north Indian school-going children.
Materials and methods
Study subjects and sampling
This school-based study was conducted in villages of Nuh District, located in Haryana, northern India, in January–February 2020. Although located close to the national capital, Nuh (formerly Mewat) is among the bottom 20 backward districts in India and has been included in the Aspirational Districts programme of the country. With an estimated prevalence of myopia being 6.8% in rural children, the relative error of 25%, design effect of 1.6, and coverage of 90%, we aimed to enrol 1559 students for the primary objective (prevalence of myopia). A case-control design was adopted for the secondary objective (association of myopia with risk factors).
Recruitment of students was two-staged. At first, schools were selected randomly from a list of all schools in the district. Two distinct types of schools were listed: Government schools and privately funded schools (reflecting on the socioeconomic status (SES) of the children attending these schools—private schools being more expensive) Thereafter, all students of classes 4 to 7 of selected schools were eligible for participation in the study.
Permission for conducting the study in the selected schools was taken from the District Education Authority. Written informed consent was taken from parents. Students who didn’t submit completely filled and signed forms by their parents were excluded from the study.
Procedures
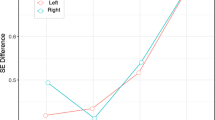
The examination was done during school hours. Line listing of students was done followed by vision assessment. The visual acuity was recorded with the help of the 'E' chart of the Early Treatment Diabetic Retinopathy Study (ETDRS) chart as the smallest line read under ambient room light by a trained health worker. Presenting visual acuity was tested in the right eye first followed by the left eye.
Children unable to read the 6/9.5 letters or those previously wearing spectacles underwent refraction by an ophthalmic technician. Streak retinoscopy refraction was done under cycloplegia using 2% homatropine hydrobromide eye drops which were instilled in the inferior conjunctival cul-de-sac twice at an interval of 10 min. After 20 min if the pupillary light reflex was still present, a third drop was administered. Cycloplegia was considered complete if the pupil dilated to 6 mm or more and there was no pupillary light reflex. Subjective acceptance testing was done after a week. The refractive error was documented on the basis of subjective acceptance.
Children prescribed spectacles were provided spectacles free of cost. Those unable to read the 6/12 letters on the ETDRS charts even after refraction or with other ocular illnesses underwent a complete ophthalmic examination by an ophthalmologist and were managed at a tertiary care facility.
Risk factor assessment
Children unable to read the 6/9.5 letters or those wearing spectacles (myopic group), and 10% of those who had normal vision (non-myopic group) selected randomly by trained health workers were assessed for myopic risk factors using a structured questionnaire. The questionnaire was interviewer-administered which aimed to collect detailed information regarding the activity patterns of the student. Time spent in various indoor and outdoor activities at home and at school expressed as a number of minutes per day was elicited. Outdoor activity was defined as any time spent outdoors, during the daytime, irrespective of physical activity. Near screen time was defined as time spent using mobile phones, tablet computers, desktop computers or playing video games. Total screen time included near screen time and television (TV) watching. Separate information was collected for weekdays and weekends, which was summated to calculate time spent per week in various activities. The details were cross-checked by confirming with his/her teacher and parents (telephonic interviews). The questions were asked in Hindi (local vernacular). The study was preceded by 1 month of staff training and field exercise in a school not a part of the study.
Statistical analysis
The spherical equivalent refractive error (SE) was calculated as the numerical sum of the sphere and half the cylinder. Myopia was defined as spherical equivalent refractive error of −0.50 D or worse in either eye, and high myopia was defined as refractive error of < −6.0 D. All myopic children were included for statistical analysis as cases. Controls included students not having any form of refractive error or any other eye diseases requiring referral to an ophthalmologist. Children who did not provide risk factor data were excluded from association analysis but were included for prevalence estimation. Statistical analysis was carried out using STATA software 15.2 (College Station, USA). The magnitude of myopia was presented as prevalence (95% CI). The risk factors were divided into demographic (non-modifiable) and behavioural (modifiable) risk factors.
Multiple logistic regression analysis was used for studying the association of risk factors of myopia and results were reported as odds ratio (95% CI). The variables included in the multivariable logistic model were age, gender, type of school, family spectacle use, mother education, total time spent outdoors (continuous) and time spent on watching television. P value <0.05 was considered statistically significant. An unplanned subgroup analysis was done comparing students of government and privately funded schools.
Ethics statement
The study was approved by the institutional ethics committee of the All India Institute of Medical Sciences, New Delhi and followed the tenets of the Declaration of Helsinki for biomedical research. Written informed consent was a prerequisite. All examinations were carried out in the presence of an appointed representative of the school. Students with the refractive error were provided free spectacles.
Results
The number of eligible children in selected schools was 1660, and 1486 children (89.5% coverage) were enroled and underwent vision screening. The number of children examined in government schools was 636 (42.8%) and 850 (57.2%) children in private schools. The mean age of children examined in the study was 11.21 ± 1.45 years and 861(57.9%) were boys. The proportion of boys and girls in the enroled and examined children was similar. The age, gender, type of school and presenting visual acuity distribution of the examined children are depicted in Table 1.
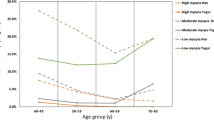
Of 1486 children examined, 132 had visual acuity <6/12 with 95 being myopic (−0.5D or worse in either eye). The prevalence of myopia was 6.4% (95% CI: 5.2%, 7.8%) in our study. It was higher among private schools (10.1%; 95% CI: 8.2%, 12.3%) compared to government schools (1.4%; 95% CI: 0.7%, 2.7%; p < 0.001), but was similar among girls 7.2% (95% CI: 5.3%, 9.5%) and boys 5.8% (95% CI: 4.3%, 7.6%; p = 0.28). The mean spherical equivalent was −1.6D ± 1.3D. The prevalence of high myopia was 1.1% (1/95) (Table 2). Among myopic children, 72 (75%) had not been wearing spectacles.
The demographic and behavioural (modifiable) risk factors were compared between myopes (n = 93) and controls (n = 331) (Table 3). Children studying in private schools had more odds of being myopic as compared to government schools (p = 0.016). An inverse association was found with outdoor activities (p = 0.009). Positive association (univariate analysis) was found for family history of wearing spectacles (p = 0.018) and higher mother education (p = 0.0004), though on multivariate analysis these were not found to be statistically significant. Watching television, indoor time or screen time, age and gender as risk factors were also not found to be statistically significant on multivariate analysis.
In view of the observed differences in the prevalence of myopia between government and private school students, we also did a head-to-head comparison between cases and controls from private and government schools for all other risk factors. We observed that students in government schools spent significantly more time in outdoor activities as compared with those in private schools (p < 0.0001). Watching television and total screen time was also higher in children of private schools (p < 0.0001) (Table 4).
Discussion
The aim of this study was to evaluate the prevalence of myopia and the possible behavioural risk factors associated with it in rural Indian school-going children. We observed a 6.4% prevalence of myopia, but there was a marked difference in the prevalence among students studying in private and government-funded schools. Time spent in outdoor activities was protective for myopia and this difference persisted after adjusting for age, gender, type of school (also itself statistically significant), familial spectacle use and TV watching.
The prevalence of myopia as per our study is consistent with the estimated prevalence in the recently published meta-analysis [10], but is higher than the estimates published by previous Indian studies [5, 9, 14] and studies from Nepal [15]. This may reflect regional differences in risk factors or may be due to an actual increase in the prevalence nationwide as has been reported in the meta-analysis [10]. Previous studies by the authors using similar methodology have reported a prevalence of 13.1% among urban school-going children in north India with an annual incidence of 3.4% [16, 17]. Higher prevalence has been reported from various other countries of East Asia [18,19,20,21,22,23,24,25,26,27,28].
In our study gender predilection for myopia was not statistically significant. A higher prevalence of myopia among girls has been reported in earlier studies from India both in rural and urban populations, possibly due to girls spending more time studying and doing other indoor activities [5, 17]. On bivariate analysis, higher maternal education showed a positive association with myopia but the same was not reproduced on multivariate analysis. Higher mother education would encourage more emphasis on the education of the girl child.
The unmet need to correct refractive errors in children was significant with over 75% of children in rural schools not wearing spectacles. In private schools, significantly greater spectacle coverage was noted as compared to government schools. This could be due to the better awareness, pressure for performance and results and greater health-seeking behaviour. However numerous barriers to the use of spectacles among these children still exist; and counselling, motivation and accessibility to eye health care facilities is necessary to improve compliance [29,30,31].
Our study found a higher prevalence of myopia among children studying in private schools compared to government schools. Although the overall academic curriculum and the number of hours spent in school were similar between the two types of schools, children in private schools spent a significantly greater time reading and writing at home, reflecting greater educational pressures and greater likelihood of attending extra classes and private tuitions. Also, these children have more access to computer, video games and television as compared to children of government schools, increasing their indoor times.
An increase in outdoor activity/playing decreases the risk of development and progression of myopia according to our study, which is consistent with the various studies previously done [10, 32]. It has been suggested that higher exposure to sunlight increases dopamine production from the retina which decreases the prevalence of myopia [33, 34]. Influence of near work such as reading at school and home on myopia was not evident in our study, however the two have been positively associated in few other studies [17, 35, 36]. Bivariate analysis of risk factors including total screen time on mobile, computer, videogame and tablets at school and home and watching television at home showed an increased risk of myopia but the results were not reproduced on multivariate analysis. This might be due to the fact that in rural areas there is a paucity of these facilities and thus children spend more time playing outdoors. Thus, watching television at home and total screen time and playing outdoors are probably not independent risk factors in our study population.
The present study had some notable limitations. First, the data was collected from examination of school-going children of a village located in the outskirts of Delhi, thus may have an urban influence; hence the results may not be reflective of the rest of rural Indian schools [5,6,7]. Secondly, ours was a questionnaire-based study which in itself may be biased subject to ways of collecting responses. Also, though a multifactorial analysis was performed, there may be overlap among commonly associated risk factors’ influence. Furthermore, our study mainly concentrated on myopia, other refractive errors were not included.
With the increasing influence of urban lifestyle, increasing awareness about the need for education, rising competition and digital revolution with easier access to the internet, mobile phones, etc. prevalence of myopia is rising among children of rural India [10]. Our study confirms the same. Also, the larger unmet need reflects a hub of unidentified myopia in rural Indian children. Thus, the myopia control programmes need to encourage regular screening, refraction, promoting regular use of spectacles, lifestyle modification and increasing awareness about risk factors. Changes in the school curriculum and education policy to increase outdoor activity also require attention.
To conclude, this study should help initiate and augment resource planning and building infrastructure for the prevention and correction of myopia, especially in rural school children, to tackle this menace on time before myopia becomes an epidemic.
Summary
What was known before
-
Earlier studies have shown a lower prevalence of myopia in children of rural India.
What this study adds
-
A study from rural northern India shows a 6.4% prevalence of myopia, a strong inverse association with time spent outdoors, higher prevalence in privately funded schools and 75% unmet need of spectacles.
References
Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86:63–70.
Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379:1739–48.
Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32:3–16.
Vitale S, Sperduto RD, Ferris FL. Increased prevalence of myopia in the United States between 1971-2 and 1999–2004. Arch Ophthalmol. 2009;127:1632–39.
Dandona R, Dandona L, Srinivas M, Sahare P, Narsaiah S, Muñoz SR, et al. Refractive error in children in a rural population in India. Invest Ophthalmol Vis Sci. 2002;43:615–22.
Murthy GV, Gupta SK, Ellwein LB, Muñoz SR, Pokharel GP, Sanga L, et al. Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci. 2002;43:623–31.
Ghosh S, Mukhopadhyay U, Maji D, Bhaduri G. Visual impairment in urban school children of low-income families in Kolkata, India. Indian J Public Health. 2012;56:163–67.
Saxena R, Vashist P, Menon V. Is myopia a public health problem in India? Indian J Community Med. 2013;38:83–5.
Sheeladevi S, Seelam B, Nukella PB, Modi A, Ali R, Keay L. Prevalence of refractive errors in children in India: a systematic review. Clin Exp Optom. 2018;101:495–503.
Agarwal D, Saxena R, Gupta V, Mani K, Dhiman R, Bhardawaj A, et al. Prevalence of myopia in Indian school children: meta-analysis of last four decades. PLoS ONE. 2020;15:e0240750.
Congdon N, Burnett A, Frick K. The impact of uncorrected myopia on individuals and society. Community Eye Health J. 2019;32:7–8.
Pratt C, Bryant P. Young children understanding that looking leads to knowing (so long as they are looking into a single barrel). Child Dev. 1990;61:973–82.
Packwood EA, Cruz OA, Rychwalski PJ, Keech RV. The psychosocial effects of amblyopia study. J AAPOS. 1999;3:15–17.
Agrawal D, Sahu A, Agrawal D. Prevalence of ocular morbidities among school children in Raipur district, India. Indian J Ophthalmol. 2020;68:340–4.
Pokharel GP, Negrel AD, Munoz SR, Ellwein LB. Refractive error study in children: results from Mechi Zone, Nepal. Am J Ophthalmol. 2000;129:436–44.
Saxena R, Vashist P, Tandon R, Pandey RM, Bhardawaj A, Gupta V, et al. Incidence and progression of myopia and associated factors in urban school children in Delhi: the North India myopia study (NIM Study). PLoS ONE 2017;12:e0189774.
Saxena R, Vashist P, Tandon R, Pandey RM, Bhardawaj A, Menon V, et al. Prevalence of myopia and its risk factors in urban school children in Delhi: the North India myopia study (NIM Study). PLoS ONE. 2015;10:e0117349.
Matsumura H, Hirai H. Prevalence of myopia and refractive changes in students from 3 to 17 years of age. Surv Ophthalmol. 1999;44:S109–S115. PMID: 10548123
Yoon KC, Mun GH, Kim SD, Kim SH, Kim CY, Park KH, et al. Prevalence of eye diseases in South Korea: data from the Korea National Health and Nutrition Examination Survey 2008-9. Korean J Ophthalmol. 2011;25:421–33.
Lim HT, Yoon JS, Hwang SS, Lee SY. Prevalence and associated sociodemographic factors of myopia in Korean children: the 2005 third Korea National Health and Nutrition Examination Survey (KNHANES III).Jpn J Ophthalmol. 2012;56:76–81.
Saw SM, Zhang MZ, Hong RZ, Fu ZF, Pang MH, Tan DT. Near-work activity, night-lights, and myopia in the Singapore-China study. Arch Ophthalmol. 2002;120:620–7.
Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singap. 2004;33:27–33.
Lin LL, Shih YF, Hsiao CK, Chen CJ, Lee LA, Hung PT. Epidemiologic study of the prevalence and severity of myopia among schoolchildren in Taiwan in 2000. J Formos Med Assoc. 2001;100:684–91.
Fan DS, Lam DS, Lam RF, Lau JT, Chong KS, Cheung EY, et al. Prevalence, incidence, and progression of myopia of school children in Hong Kong. Invest Ophthalmol Vis Sci. 2004;45:1071–5.
Lam CS, Lam CH, Cheng SC, Chan LY. Prevalence of myopia among Hong Kong Chinese schoolchildren: changes over two decades. Ophthalmic Physiol Opt. 2012;32:17–24.
He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern China. Invest Ophthalmol Vis Sci. 2004;45:793–99.
Qian YS, Chu RY, He JC, Sun XH, Zhou XT, Zhao NQ, et al. Incidence of myopia in high school students with and without red-green color vision deficiency. Invest Ophthalmol Vis Sci. 2009;50:1598–605.
You QS, Wu LJ, Duan JL, Luo YX, Liu LJ, Li X, et al. Prevalence of myopia in school children in great- er Beijing: the Beijing Childhood Eye Study. Acta Ophthalmol. 2014;92:e398–406.
Rustagi N, Uppal Y, Taneja DK. Screening for visual impairment: outcome among schoolchildren in a rural area of Delhi. Indian J Ophthalmol. 2012;60:203–06.
Gogate P, Mukhopadhyaya D, Mahadik A, Naduvilath TJ, Sane S, Shinde A, et al. Spectacle compliance amongst rural secondary school children in Pune district, India. Indian J Ophthalmol. 2013;61:8–12.
Gupta V, Saxena R, Vashist P, Bhardwaj A, Pandey RM, Tandon R, et al. Spectacle coverage among urban schoolchildren with refractive error provided subsidized spectacles in North India. Optom Vis Sci. 2019;96:301–08.
Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007;48:3524–32.
Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmol. 2008;115:1279–85.
Ashby R, Ohlendorf A, Schaeffel F. The effect of ambient illuminance on the development of deprivation myopia in chicks. Invest Ophthalmol Vis Sci. 2009;50:5348–54.
Saw SM, Cheng A, Fong A, Gazzard G, Tan DT, Morgan I. School grades and myopia. Ophthalmic Physiol Opt. 2007;27:126–29.
Morgan IG, Rose KA. Myopia and international educational performance. Ophthalmic Physiol Opt. 2013;33:329–38.
Acknowledgements
The authors would like to acknowledge the assistance of all school principals and teachers for their support. We also acknowledge the contribution of Mr. Deepak towards data analysis.
Funding
The study was funded through Grant number E-1475/390/2015 of the Department of Science and Technology, Government of India. The funds were for school visits, data collection and analysis. None of the authors are employed by the funding agency (www.dst.gov.in). The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
R.S.—Concept and editing of the manuscript. V.G.—conduction of the study and data collection. P.P.—preparation of manuscript A.B.—data analysis. P.V.—conduction of the study and data collection.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Saxena, R., Gupta, V., Prasad, P. et al. Prevalence of myopia and its risk factors in rural school children in North India: the North India myopia rural study (NIM-R Study). Eye 36, 2000–2005 (2022). https://doi.org/10.1038/s41433-021-01797-3
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01797-3
