
Abstract
Background/objectives
The aim of this study was to compare surgical outcomes and postoperative characteristics, between eyes that underwent pars plana vitrectomy (PPV) for RRD, with air or different gas agents as tamponade.
Subjects/methods
The records of 262 patients that underwent PPV for RRD with air or different gas tamponades and a follow-up of at least 6 months were examined. Only cases with superior retinal breaks were included. Demographic, pre-, intra- and postoperative characteristics including rate of recurrence and complications were analysed.
Results
48 patients were treated with air and 214 were treated with gas. No differences were found in success rate between air and gas group at both 3 and 6 months (respectively, 93.8% vs 93.6 and 100% vs 100%, all P values > 0.05). Postoperative best-corrected visual acuity (BCVA) was significantly higher in the air group compared with the gas group 7 days and 1 month postoperatively (respectively, 0.2 ± 0.4 vs 2.6 ± 0.5, P < 0.001 and 0.1 ± 0.4 vs 0.4±0.9, P = 0.04). The occurrence ocular hypertension at 1 month postoperatively was significantly higher in the gas group compared with the air group (15.4 % vs 0%, P < 0.001). At 6 months, the prevalence of epiretinal membrane (ERM) was significantly higher in the gas group compared with air group (4.2% vs 16.8%, P = 0.02).
Conclusions
Air was comparable to gas tamponades in terms of surgical outcome and BCVA at 6 months. In addition, air allowed an earlier visual recovery and resulted in a lower rate of postoperative ocular hypertension and ERM.
Similar content being viewed by others


Introduction
Rhegmatogenous retinal detachment (RRD) is a major cause of visual loss in developed countries. It is caused by the presence of one or more retinal breaks that allow the passage of fluid from the vitreous cavity into the subretinal space, leading to the separation of the neurosensory retina from the underlying retinal pigment epithelium [1]. Thanks to recent innovations and improvements in the surgical field, pars plana vitrectomy (PPV) with gas tamponade is becoming an increasingly popular technique for the treatment of RRD. The rationale for the use of intraocular gas is to tamponade retinal breaks following surgery, in order to ensure the re-attachment of the retina [2]. The most commonly used tamponade agents are sulfur hexafluoride (SF6), perfluoroethane (C2F6) and octafluoropropane (C3F8), which are able to exert a long-lasting tamponade action [2]. Although the use of tamponade agents at the conclusion of PPV is well established, these have some limitations such as long postoperative positioning, a slow visual recovery, the need to avoid travels by plane or at high altitudes in the postoperative period and their availability could be limited particularly in developing countries [3]. In addition, different potential complications have been reported in eyes treated with intraocular gases, including postoperative ocular hypertension, cataract progression, and blood-retinal barrier breakdown [4,5,6]. Previous studies showed that room air is able to provide a good tamponade efficacy and can represent a valid alternative to the use of intraocular gases. Moreover, being not expandable and having a short persistence time in the vitreous cavity, room air presents a limited risk of postoperative hypertension and allows rapid visual recovery [7,8,9,10,11,12,13,14,15,16]. Although air is considered an effective tamponade agent in the treatment of superior RRD, to date only few reports have specifically investigated this aspect and limited information is available on long-term follow-up and postoperative complications [7,8,9, 15]. Thus, the aim of this study was to compare surgical outcomes and postoperative characteristics between eyes that underwent 25-gauge PPV, for the treatment of primary superior RRD, with air or different gas agents as tamponade.
Material and methods
Study design and patients
This retrospective multicentre study included patients treated for RRD at two tertiary academic referral centres (OphtalmoPole de Paris, Hôpital Cochin (Paris, France), Hôpital des Quinze-Vingts (Paris, France) between January 2016 and May 2020. Institutional review board approvals for retrospective chart reviews were obtained commensurate with the respective institutional requirements prior to the beginning of the study. Described research was approved by the ethics committee of the French society of ophthalmology (IRB 00008855) and adhered to the tenets of the declaration of Helsinki. Consecutive patients that underwent uneventful PPV for primary RRD were screened for enrolment. We included patients, both phakic and pseudophakic, that presented superior retinal break(s), between 3 and 9 o’clock, and had either air or a gas (SF6, C2F6 or C3F8) as tamponade. Exclusion criteria were: a follow-up of less than 6 months, any previous vitreoretinal surgery, external buckling procedure, use of silicon oil tamponade, presence of retinal break(s) between 4 and 8 o’clock, presence of giant retinal tears, inability to maintain a postoperative positioning, existence of vitreoretinal disease, including preoperative macular membranes, presence of macular hole and any risk factors for proliferative vitreoretinopathy at the time of diagnosis, in particular: aphakia, uveitis, choroidal detachment, penetrating trauma.
Surgical procedure
All the procedures were performed under regional anaesthesia by peribulbar injection and/or sub-tenon injection of 6 mL of 2% xylocaine and 2 mL of 0.5% bupivacaine. Three-port 25-gauge PPV was performed using the Alcon Constellation system (Alcon Laboratories, Inc, Forth Worth, TX) or Stellaris Elite System (Bausch & Lomb, St. Louis, MO, USA) and a wide-angle viewing lens. After central and peripheral vitreous removal, all eyes underwent 360° scleral indentation to shave the vitreous base up to the ora serrata, followed by the removal of vitreous tractions from retinal tears. According to surgeon’s preference perfluorocarbon liquid (PFCL) was used in selected cases. Subsequently, a complete fluid–air exchange was performed, and subretinal fluid was aspirated with a flute needle. Patients underwent either trans-scleral cryopexy or endolaser to achieve retinopexy under air. The sclerotomy was closed with 8.0 vicryl to avoid gas leakage at surgeon’s discretion. At the end of the procedure patients had either air or a gas tamponade (20% SF6, 17% C2F6, 14% C3F8). All the patients were required to adopt a face down positioning for 6 h. Anatomically, a successful surgery was defined as the complete disappearance of SRF and flattening of the entire circumference of the retinal breaks. Hypotonizing eye drops containing brinzolamide 10 mg/ml and timolol maleate 5 mg/ml, two times a day, were prescribed after surgery to all patients and were discontinued after one month if IOP was normal.
Data collection
Patients were divided into two groups according to the use of air or gas as a tamponade during surgical procedure. The clinical data was extracted from an electronic patient record containing pre- and postoperative examinations and the operative report. The following data were collected: (i) Epidemiological characteristics including age, sex and ophthalmological history (high myopia, glaucoma and other ocular diseases); (ii) Preoperative evaluation including best corrected visual acuity (BCVA) in Snellen, the status of the lens (phakic or pseudophakic), intraocular pressure (IOP) with Goldmann applanation tonometer, slit lamp biomicroscopy and fundus examination with accurate evaluation of the peripheral retina using 3-mirrors lens. In addition, the presence of vitreous haemorrhage, the extent in quadrant of RRD, the status of the macula, the number of retinal breaks were noted. If preoperative vitreous haemorrhage was present, a B-mode ultrasound was systematically carried out; (iii) Intraoperative procedures including use of PFCL, type of retinopexy (cryo or laser -therapy), tamponade (air, 20% SF6, 17% C2F6, 14% C3F8); iv) Postoperative evaluations performed at 7 days (D7), 1 month (M1), 3 months (M3) and 6 months (M6) following the surgical procedure, including BCVA in Snellen, IOP with Goldmann applanation tonometer, occurrence of complications on fundus or OCT examination, presence of a recurrence, existence of a proliferative vitreoretinopathy (PVR) and cataract progression.
The status of the lens was assessed during slit lamp examination according to the Lens Opacities Classification System III [17]. A change between the baseline and last follow-up visit was registered as cataract progression.
The percentage of gas or air remaining at day 7 was estimated by two of the authors (AA and FB) in wide-field fundus images (Optos California, Optos plc, Dunfermline, Scotland) and the average of the two observers’ results was used for statistical analysis. In addition, the presence of ocular hypertension, defined as an IOP ≥ 25 mmHg or ≥ 10 mm Hg compared to the preoperative value.
For statistical analysis, Snellen ratios were converted to LogMAR (logarithm of the minimum angle of resolution) decimal values [18].
Surgical success was defined as the absence of recurrence 3 months after the initial surgical procedure. The rate of success was compared between the two groups. Secondary outcome measures included: surgical success following a second procedure evaluated at 6 months after the initial procedure. If recurrence occurred, time between first procedure was noted and compared between the two groups.
Statistical analysis
The R studio software, version 3.6.2 (http://www.r-project.org) was used for data analysis. Values are expressed as mean ± standard deviation. The Shapiro–Wilk test was used to determine normality of data. An independent t-test was used to compare normally distributed variables between the two groups, whereas the Mann–Whitney U test was used for not normally distributed variables. Comparisons of qualitative data were performed using the chi-square test or the exact test of Fisher when appropriate. A multiple logistic regression analysis was performed to identify potential independent predictors associated with the recurrence of RRD. A P value < 0.05 was considered statistically significant.
Results
Baseline demographic and clinical characteristics of patients
A total of 262 patients treated with PPV for superior RRD were included in the study. Forty-eight received air tamponade while 214 patients received gas tamponade (SF6, C2F6, C3F8). The air group consisted of 25 women (52%) and 23 men (48%), mean age was 62.2 ± 8.9 years. The gas group consisted of 82 women (38.3%) and 132 men (61.7%), mean age was 64.3 ± 11 years. Demographic and clinical characteristics of the two groups are reported in Table 1. There were no significant differences in age, sex, history of glaucoma or high myopia and lens status between the two groups (all P values > 0.05). Surgical characteristics of air and gas groups are reported in Table 2. There were no significant differences in preoperative clinical parameters including BCVA, IOP, presence of vitreous haemorrhage, extension of RRD, number of retinal breaks and status of the macula between the two groups (all P values > 0.05). Regarding the surgical procedure, only the type of retinopexy differed significantly between the two groups: in the air group 66.7% (n = 32) underwent cryotherapy and 33.7% (n = 16) underwent laser, while in the gas group 37.3% (n = 80) underwent cryotherapy and 62.6% (n = 134) underwent laser (always P < 0.001). In the gas group, 118 (51.1%) patients had had SF6, 88 (41.1%) C2F6, and 8 (3.7%) C3F8.
Postoperative characteristics
No significant differences were found in primary success rate between air and gas group at both 3 and 6 months (respectively, 93.8% vs 93.6 and 100% vs 100%, all P values > 0.05). The comparisons of clinical characteristics between the two groups after surgery for RRD are reported in Table 3. Time to recurrence evaluated at 6 months was not significantly different between groups (respectively, 25.7 ± 21.4 days vs 41.6 ± 40.9, P = 0.37). Among patients with recurrences, in the gas group 3 (1.4%) exhibited PVR at 3 months postoperatively while none of the air group presented this latter complication. However, the difference between the two groups was not statistically significant (P = 1). The 3 cases of recurrence observed in the air group were treated with 25-gauge PPV and gas tamponade (2 by SF6, 1 by C2F6). In the gas group, all the patients with recurrences were treated with 25-gauge PPV and gas tamponade (7 by SF6, 3 by C2F6) or 1000 cs silicone oil (4 cases).
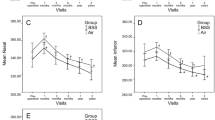
Postoperative BCVA was significantly higher in the air group compared with the gas group, at both, 7 days (respectively, 0.2 ± 0.4 vs 2.6 ± 0.5, P < 0.001) and 1 month (respectively, 0.1 ± 0.4 vs 0.4 ± 0.9, P = 0.04) after surgical procedure. No significant difference was found in BCVA between air and gas group at 3 months (0.1 ± 0.1 vs 0.2 ± 0.4, P = 0.24). The percentage of air in the vitreous cavity at day 7 was 30% while in the gas group it was 72%, 90% and 95%, respectively for SF6, C2F6 and C3F8.
Mean IOP was significantly higher in the gas group compared with air group at 7 days postoperatively (respectively, 18.1 ± 4.8 vs 14.7 ± 3.6 mmHg, P < 0.001), while no significant difference was found 1 month postoperatively (respectively, 15.3 ± 3.4 mmHg and 15.7 ± 3.1, P = 0.68). The occurrence of ocular hypertension during the first month postoperatively was significantly higher in the gas group compared with the air group (respectively, 33 (15.4 %) vs 0 (0%), P < 0.001).
Among macular complications detected on OCT scans at 6 months, the prevalence of epiretinal membrane (ERM) was significantly higher in the gas group compared with the air group (2 (4.2%) vs 36 (16.8%), P = 0.02). To the contrary, no significant differences were found in the prevalence of cystoid macular oedema and macular hole between the two groups (respectively, 1 (2.1%) vs 10 (4.7%) and 0 vs 1 (0.5%), always P > 0.05). No significant difference was found in the progression of cataract at 6 months postoperatively between air and gas group (respectively, 6 (12.5%) vs 31 (26%), P = 0.90).
The comparisons of potential factors predicting surgical success between the two groups are reported in Table 4. The results of multiple regression analysis are reported in Table 5. No predictive factor for RRD recurrence was identified among the following variables: type of tamponade agent, age, gender, history of high myopia, extent of RRD, presence of vitreous haemorrhage, status of the macula, status of the lens, type of retinopexy.
Discussion
The use of intraocular gas tamponades is increasingly common in vitreoretinal surgery, particularly in the treatment of RRD. In fact, in this case their surface tension is able to ensure an adequate adhesion of the retina, preventing the passage of fluid in the subretinal space [2]. Several studies investigated the role of air during PPV in the treatment of RRD showing good outcomes in terms of surgical success, ranging from 70 to 100% [7,8,9,10,11,12,13,14,15, 19]. In our routine surgical practice air is used only for RRD that are caused by superior retinal breaks, preferring the use of long-acting tamponades or episcleral surgery in the other cases. In the present study, we retrospectively evaluated surgical outcomes and postoperative complications in eyes that underwent PPV for the treatment of RRD related to superior retinal breaks, comparing air tamponed with gas agents. Interestingly, we observed the same efficacy of air and gas tamponade in terms of surgical success at both 3 and 6 months. In addition, we found no difference in the time to recurrence evaluated at 6 months.
As far as we are aware, only two previous studies specifically investigated this issue [8, 12]. Our results are in agreement with those of Pak and co-authors, that, however, are limited by a follow-up of only 3 months [12]. On the contrary, Tan et al. reported that SF6 seems to be slightly superior to air in RRD with involvement of the lower quadrants [8]. However, some baseline characteristics, including, the status of the macula, the status of the lens and the involvement of the inferior quadrants, differed between the two groups limiting the conclusions that may be drawn [8].
The good efficacy of air probably lies in the fact that the adhesion between the retina and the retinal pigment epithelium occurs within 24 h in the absence of subretinal fluid, thus the persistence time of air in the vitreous cavity is enough to ensure the reattachment of the retina [20].
In the present study, air showed better outcomes compared with gas tamponades in terms of early visual recovery. In fact, patients in air group presented a significantly better BCVA at both 7 days and 1 month after surgical procedure. This is related to the fact that it has a persistence time of 7 days, which is shorter compared with those of gas tamponades agents, respectively 1–2 weeks for SF6, 4–5 weeks for C2F6 and 6–8 weeks for C3F8 2. In this way, air allows a faster functional recovery of the patient resulting in reduced socio-economic burden. In addition, this can represent an advantage in one-eyed patients who need rapid visual recovery after surgery.
We observed that, despite the treatment with hypotonizing eye drops, a high rate of patients in the gas group presented ocular hypertension during the first month after the surgical procedure. Conversely, no patient in the air group showed this complication. This is probably related to the expandable nature of gas tamponades, even when they are using at non-expansive concentrations. The increase in IOP in patients who received gas tamponade has already been reported with a similar prevalence [21]. These results, on one hand encourage the administration of hypotonizing eye drops in the early postoperative period when gas agents are used, in order to avoid possible damages to the ganglion cells. On the other hand, the present study supports the safety profile of air regarding postoperative IOP.
Surprisingly, we found that patients in the gas group showed a significantly higher prevalence of ERM at 6 months compared with those in the air group. As far as we are aware, this is the first study reporting such results [7,8,9,10,11,12,13,14,15, 19]. Only two previous reports evaluated this complication showing no statistical difference between gas and air group [8, 22]. Nevertheless, these data could be underestimated since it is not clear whether this feature was systematically evaluated by using OCT [8, 22].
The pathogenesis of ERM seems to be related to the dispersion and the proliferation over the retinal surface of cells derived from the retinal pigment epithelium, the retinal glia and the perivascular connective tissue [23,24,25]. Different risk factors for the occurrence of ERM after PPV for RRD have been proposed, such as number and size of retinal breaks, macula-off status, use of cryopexy, presence of proliferative vitreoretinopathy and/or vitreous haemorrhage at baseline [23,24,25].
In the present study, baseline characteristics were comparable in the two groups in terms of number of retinal breaks, extension of RRD, PVR rate and status of the macula. In addition, cryotherapy, that was previously associated with ERM formation, was more used in patients in the air group [23,24,25]. It could be speculated, that the high occurrence of ERM in the gas group could be related with the compartmentalisation effect produced by intraocular gas bubble. However, further longitudinal studies are needed to investigate the causal relationships between intraocular tamponades and the formation of ERM.
Interestingly, at the last follow-up visit, patients in the gas group showed a higher prevalence of cataract progression, although the difference between the two groups was not significant. A previous report showed that severity of cataract progression following vitreoretinal procedures with gas tamponade correlates with the persistence time of the intraocular tamponade in the vitreous cavity [26]. It has been hypothesised that the presence of intravitreal tamponade could induce the dehydration of the posterior layers of the lens resulting in cataract progression [26]. Thus, it can be assumed that the reduced persistence time of air could results in a lower occurrence of cataract compared with gas tamponade. Further studies with larger sample size and longer follow-up will be helpful to clarify this issue.
Finally, among the advantages that air tamponade seems to offer compared with intraocular gas agents, it must be emphasised that it has a considerable economic impact that becomes particularly relevant in developing countries where resources can be limited.
Although, the present study has several strengths, such as the well-matched baseline characteristics between the two groups and the evaluation of different postoperative complications, it suffers from some limitations that need to be acknowledged. In particular, its retrospective nature and the absence of randomisation between the use of air or gas tamponades, may have resulted in selection or indication bias, limiting the conclusions we can draw from our results. In addition, although a 6-month follow-up is considerable, studies with a longer follow-up are desirable to assess more accurately both postoperative complications and final BCVA.
In conclusion, our results showed that the use of air as intraocular tamponade at the end of 25-gauge PPV for the treatment of RRD related to superior breaks, was not different from gas tamponades in terms of surgical outcome and BCVA at 6 months. In addition, compared with gas agents, air tamponade allowed an earlier visual recovery and was associate with fewer postoperative complications, including ocular hypertension and ERM.
Summary table
What was known before
-
Air as tamponade in pars plana vitrectomy for rhegmatogenous retinal detachment seems to be an effective alternative to gas agents.
-
To date, controversial data are available on postoperative outcomes and complications
What this study adds
-
Air was comparable to gas in terms of surgical success at 6 months.
-
Patients treated with air showed an early visual recovery, a lower prevalence of postoperative ocular hypertension and a lower occurrence of epiretinal membrane.
References
Park SW, Lee JJ, Lee JE. Scleral buckling in the management of rhegmatogenous retinal detachment: patient selection and perspectives. Clin Ophthalmol. 2018;12:1605–15. Available at: http://www.ncbi.nlm.nih.gov/pubmed/30214145 Accessed October 14, 2019
Neffendorf JE, Gupta B, Williamson T H. The role of intraocular gas tamponade in rhegmatogenous retinal detachment: a synthesis of the literature. Retina. 2018;38:S65–S72. Available at: https://pubmed.ncbi.nlm.nih.gov/29280936/ Accessed November 20, 2020
Chan CK, Lin SG, Nuthi ASD, Salib DM. Pneumatic retinopexy for the repair of retinal detachments: a comprehensive review (1986–2007). Surv Ophthalmol. 2008;53:443–78. Available at: https://pubmed.ncbi.nlm.nih.gov/18929759/ Accessed November 26, 2020
Chang S, Lincoff HA, Coleman DJ, Fuchs W, Farber ME. Perfluorocarbon gases in vitreous surgery. Ophthalmology. 1985;92:651–6. Available at: https://pubmed.ncbi.nlm.nih.gov/4011139/ Accessed November 26, 2020
Abrams GW, Swanson DE, Sabates WI, Goldman AI. The results of sulfur hexafluoride gas in vitreous surgery. Am J Ophthalmol. 1982;94:165–71.
Fang IM, Huang JS. Central retinal artery occlusion caused by expansion of intraocular gas at high altitude. Am J Ophthalmol. 2002;134:603–5. Available at: https://pubmed.ncbi.nlm.nih.gov/12383821/ Accessed November 26, 2020
Zhang Z, Peng M, Wei Y, Jiang X, Zhang S. Pars plana vitrectomy with partial tamponade of filtered air in Rhegmatogenous retinal detachment caused by superior retinal breaks. BMC Ophthalmol. 2017;17:64. Accessed November 27, 2020.
Tan HS, Oberstein SY, Mura M, Bijl HM. Air versus gas tamponade in retinal detachment surgery. Br J Ophthalmol. 2013;97:80–2.
Chen QY, Tang YX, He YQ, Lin HM, Gao RL, Li MY, et al. Air tamponade in retinal detachment surgery followed by ultra-widefield fundus imaging system. Int J Ophthalmol. 2018;11:1198–203. Available at: https://pubmed.ncbi.nlm.nih.gov/30046539/ Accessed November 27, 2020
Zhou C, Qiu Q, Zheng Z. Air versus gas tamponade in rhegmatogenous retinal detachment with inferior breaks after 23-gauge pars plana vitrectomy: a prospective, randomized comparative interventional study. Retina. 2015;35:886–91.
Sinawat S, Ratanapakorn T, Sanguansak T, Prompol S, Laopaiboon M, Yospaiboon Y. Air vs perfluoropropane gas in pneumatic retinopexy: a randomized noninferiority trial. Arch Ophthalmol. 2010;128:1243–7.
Pak KY, Lee SJ, Kwon HJ, Park SW, Byon IS, Lee JE. Exclusive use of air as gas tamponade in rhegmatogenous retinal detachment. J. Ophthalmol. 2017;2017:1341948. Accessed November 27, 2020.
Martínez-Castillo V, Verdugo A, Boixadera A, García-Arumí J, Corcóstegui B. Management of inferior breaks in pseudophakic rhegmatogenous retinal detachment with pars plana vitrectomy and air. Arch Ophthalmol. 2005;123:1078–81. Available at: https://jamanetwork.com/ Accessed November 27, 2020
Hotta K, Sugitani A, Uchino Y. Pars plana vitrectomy without long-acting gas tamponade for primary rhegmatogenous retinal detachment. Ophthalmologica. 2004;218:270–3. Available at: https://pubmed.ncbi.nlm.nih.gov/15258417/ Accessed November 27, 2020
Michalska-Małecka K, Sierocka-Stȩpień J, Michalik-Jakubek A, Witek K, Nowomiejska K, Jünemann A, et al. Evaluation of the treatment results in patients with rhegmatogenous retinal detachment treated by pars plana vitrectomy with air. Medicines (United States). 2018; 97. https://pubmed.ncbi.nlm.nih.gov/29851816/. Accessed November 27, 2020.
Moussa G, Mathews N, Makhzoum O, Park DY. Vitrectomy with air tamponade and cryotherapy for retinal detachment repair without perfluorocarbon use: A UK 12-month prospective case series. Eur. J. Ophthalmol. 2020: 112067212097888. http://journals.sagepub.com/doi/10.1177/1120672120978884. Accessed December 22, 2020.
Chylack LT, Wolfe JK, Singer DM, Leske MC, Bullimore MA, Bailey IL, et al. The lens opacities classification system III. Arch Ophthalmol. 1993;111:831–6. Available at: https://pubmed.ncbi.nlm.nih.gov/8512486/ Accessed May 24, 2021
Moussa G, Bassilious K, Mathews N. A novel excel sheet conversion tool from Snellen fraction to LogMAR including ‘counting fingers’, ‘hand movement’, ‘light perception’ and ‘no light perception’ and focused review of literature of low visual acuity reference values. Acta Ophthalmol. 2020. https://pubmed.ncbi.nlm.nih.gov/33326177/. Accessed December 22, 2020.
Martínez-Castillo VJ, García-Arumí J, Boixadera A. Pars Plana vitrectomy alone for the management of pseudophakic rhegmatogenous retinal detachment with only inferior breaks. In: Ophthalmology. Vol 123. Elsevier Inc.; 2016. pp. 1563–9. https://pubmed.ncbi.nlm.nih.gov/27126928/. Accessed November 27, 2020.
Folk JC, Sneed SR, Folberg R, Coonan P, Pulido JS. Early retinal adhesion from laser photocoagulation. Ophthalmology. 1989;96:1523–5. Available at: https://pubmed.ncbi.nlm.nih.gov/2587048/ Accessed December 3, 2020.
Sigler EJ, Randolph JC, Charles S, Calzada JI. Intravitreal fluorinated gas preference and occurrence of rare ischemic postoperative complications after pars plana vitrectomy: a survey of the American Society of Retina Specialists. J. Ophthalmol. 2012;2012:230596.
Tetsumoto A, Imai H, Hayashida M, Otsuka K, Matsumiya W, Miki A, et al. The comparison of the surgical outcome of 27-gauge pars plana vitrectomy for primary rhegmatogenous retinal detachment between air and SF6 gas tamponade. Eye. 2020;34:299–306. Available at: https://pubmed.ncbi.nlm.nih.gov/31857712/ Accessed November 27, 2020.
Katira RC, Zamani M, Berinstein DM, Garfinkel RA. Incidence and characteristics of macular pucker formation after primary retinal detachment repair by pars plana vitrectomy alone. Retina. 2008;28:744–8. Available at: https://pubmed.ncbi.nlm.nih.gov/18463520/ Accessed December 7, 2020
Martínez-Castillo V, Boixadera A, Distéfano L, Zapata M, García-Arumí J. Epiretinal membrane after pars plana vitrectomy for primary pseudophakic or aphakic rhegmatogenous retinal detachmentincidence and outcomes. Retina. 2012;32:1350–5. Available at: https://pubmed.ncbi.nlm.nih.gov/22414957/ Accessed December 7, 2020
Sella R, Sternfeld A, Budnik I, Axer-Siegel R, Ehrlich R. Epiretinal membrane following pars plana vitrectomy for rhegmatogenous retinal detachment repair. Int J Ophthalmol. 2019;12:1872–7. Available at: https://pubmed.ncbi.nlm.nih.gov/31850171/ Accessed December 7, 2020
Modi A, Giridhar A, Gopalakrishnan M. Sulfurhexafluoride (Sf6) versus perfluoropropane (C3f8) gas as tamponade in macular hole surgery. Retina. 2017;37:283–90. Available at: http://journals.lww.com/00006982-201702000-00008 Accessed December 6, 2020
Author information
Authors and Affiliations
Contributions
AA and PRR designed the study; AA, FB and PRR wrote the draft of the manuscript, JB, RA, JA, AS, FA, ML, GG, TR and PRR contributed to patient management and acquisition of data; MBC, AA, FA and FB analysed the data; JB, RA, JA, AS, FA, ML, GG, TR and PRR performed the surgical procedure; PRR and JPN supervised the work. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Amara, A., Bernabei, F., Chawki, M.B. et al. Comparison between air and gas as tamponade in 25-gauge pars plana vitrectomy for primary superior rhegmatogenous retinal detachment. Eye 36, 2028–2033 (2022). https://doi.org/10.1038/s41433-021-01739-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01739-z
This article is cited by
-
Outcomes of short- versus long-acting gas tamponades in vitrectomy for rhegmatogenous retinal detachment
International Journal of Retina and Vitreous (2024)
