
Abstract
Objectives
To observe the changes of viral load in aqueous humour samples and visual outcomes in varicella zoster virus (VZV)-induced acute retinal necrosis (ARN).
Methods
Observational retrospective study. Medical records and viral load measured by real-time quantitative polymerase chain reaction (qPCR) of 20 eyes with VZV-induced ARN were reviewed.
Results
The mean viral load at presentation was 5.7 × 107 ± 9.7 × 107 copies/mL. An initial plateau phase for viral load lasting up to 2 weeks occurred in most eyes (18 eyes, 90%). In the following logarithmic reduction phase, the mean slope of the decline in viral load was −0.103 ± 0.029 log/day, and the expected time for half reduction of the initial viral load was 3.2 ± 1.0 days. At the end of the first 8-week’s antiviral treatment, the viral load was below detection threshold in all 20 eyes (100.0%). The mean logarithm of the minimum angle of resolution (logMAR) best-corrected visual acuity (BCVA) improved from 1.1 ± 0.7 (Snellen equivalent 20/250) to 0.7 ± 0.6 (Snellen equivalent 20/100) after a follow-up of 8.6 ± 2.0 months. Thirteen of the 20 eyes (65.0%) suffered retinal detachment and underwent vitrectomy. The initial viral load was the independent predictive factor of logMAR BCVA at the last follow-up (β = 0.745, P < 0.001).
Conclusions
The observation of viral load changes by qPCR was useful for better monitoring of therapeutic efficacy and deciding needed antiviral duration in VZV-induced ARN patients.
Similar content being viewed by others

Introduction
Acute retinal necrosis (ARN) is a panuveitis entity caused by herpes virus family infection, with varicella zoster virus (VZV) the most common causative pathogen [1]. ARN is characterised by acute necrotising retinitis, which may be complicated by retinal detachment (RD) [2, 3]. ARN is a rapidly destructive form of infectious uveitis, timely antiviral treatment and monitoring the extent of disease are vital. The extent of necrotising retinitis is routinely monitored under clinical observation, the assessment is usually subjective, and it is difficult to observe the posterior segment in some eyes with vitreous opacities [2, 4].
Real-time quantitative polymerase chain reaction (qPCR) is a technique which can quantify the genome copies of pathogen in samples, thus provides us a perspective to monitor the extent of infectious diseases beyond clinical observation [5]. Real-time qPCR has been used to diagnose viral infections and assess response to antiviral therapy in a series of studies, including ARN [6, 7]. But most of the studies were single case reports or small case series. The changes of viral deoxyribonucleic acid (DNA) load after antiviral treatment have not been well described in ARN patients in a substantial series.
In the present study, we assessed the changes of viral DNA load in aqueous humour samples by real-time qPCR in VZV-induced ARN patients, in order to evaluate the contribution of real-time qPCR for monitoring and treatment of ARN.
Methods
Diagnosis criteria and data compilation
In this observational retrospective study, we examined the clinical records of all subjects with a diagnosis of ARN who visited our clinic between December 2018 and November 2019. All eyes were clinically diagnosed according to the diagnostic criteria for ARN defined by the American Uveitis Society [3], and eyes with VZV infection identified by PCR were included in the study.
Demographic and clinical data, including age, sex, laterality, duration between symptoms and presentation, and previous medical history were collected. Ophthalmologic characteristics were also collected, including best-corrected visual acuity (BCVA) at presentation and last follow-up, initial retinal quadrants and zones involved referring to the previous definition for cytomegalovirus (CMV) retinitis [8], type of treatment, and occurrence of RD. Visual acuity was recorded by Snellen visual acuity ratios, while logarithms of the minimum angle of resolution (logMAR) was applied for statistical analysis [9].
The study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of the Eye and ENT Hospital of Fudan University.
Treatment protocol
All subjects received a combined antiviral treatment. Systemic treatment included intravenous antiviral treatment (acyclovir, 10 mg/kg, q8h) for the first 14 days, and a following oral administration (valaciclovir 2000 mg tid for 2 weeks, followed by a maintenance dose of 1000 mg tid). Intravitreal injections of ganciclovir, 4 mg/0.1 mL, twice a week were administered once ARN was suspected, and until the disappearance of active retinitis was observed by two senior doctors (R.J. and M.Z.), or the occurrence of RD requiring vitrectomy. Intravitreal antiviral injections could be administered for a maximal dose of nine injections (4 weeks’ duration). An intravitreal or oral corticosteroid was given depending on the severity of intraocular inflammation. Patients with RD underwent vitrectomy with silicon oil tamponade.
Sample collection and virological analysis
Aqueous humour samples (~100 μL) were collected from each participant before intravitreal injections, and were used for a qualitative multiplex PCR assay to measure the genomic DNA levels of herpes simplex virus type 1, type 2, VZV, Epstein–Barr virus, and CMV at the first visit, as previously described [10]. If VZV was detected, a real-time qPCR assay was performed. For eyes with VZV-induced ARN, the scheduled time point for aqueous humour samples collection and real-time qPCR analysis was the time of the first visit (day 1), day 4, week 1, 2, 3, 4 in the first 4-week’s treatment, and was stopped at any time when intravitreal injections discontinued. During the following treatment, aqueous humour samples collection and real-time qPCR analysis was made once a month until the viral load was below detection threshold. The real-time qPCR assay was performed with a TaqMan PCR kit (Shanghai ZJ Bio-Tech Co., Ltd., Shanghai, China) and a real-time PCR system (ABI 7500, Thermo Fisher Scientific, Waltham, MA), as previously described [11]. The viral DNA load is expressed as the number of copies per millilitre of aqueous humour. The threshold of detection was 1 × 103 copies/mL.
Statistical analysis
Continuous data are described as means ± standard deviations. Categorical data are described as the absolute and relative frequencies in each category. Nonparametric statistical tests including the Wilcoxon test and Spearman test were used, for the data were positively skewed on histograms. A multiple regression analysis was used to identify the virological parameters that were independently associated with the visual outcome. The viral DNA load was modelled using a logarithmic decay curve; the exponential model was analysed using linear regression analysis.
P Values of <0.05 were considered as statistically significant. SPSS for Windows version 17.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
Results
Baseline characteristics
During the study period, 32 eyes in 28 patients were diagnosed as ARN. VZV was detected in the aqueous humour samples in 27 eyes of 25 patients. Continuous aqueous humour samples were collected in 20 eyes (13 left eyes and 7 right eyes) of 20 patients (13 men and 7 women), which were included in this study. No primary (congenital) or secondary immune deficiencies were found in any of the patients. The patients’ demographic and baseline clinical data are listed in Table 1.
Treatment and outcomes
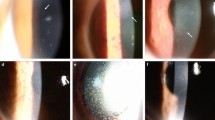
The logMAR BCVA was 1.1 ± 0.7 (Snellen equivalent 20/250; range, hand motion (HM) to 20/66) at first visit, and 0.7 ± 0.6 (Snellen equivalent 20/100; range, HM to 20/20) at the last follow-up, at a mean of 8.6 ± 2.0 months (range, 6–12 months) (P = 0.012). Visual acuity improved in 13 eyes (65.0%), remained the same in five eyes (25.0%), and decreased in two eyes (10.0%). Visual acuity was 20/200 or less in four eyes (20.0%) at the last follow-up (Fig. 1).

BCVA best-corrected visual acuity, logMAR logarithm of the minimum angle of resolution.
RD occurred in 13 of 20 eyes (65.0%) and was treated with vitrectomy. The mean duration between symptoms and occurrence of RD was 8.0 ± 5.3 weeks (range, 1–18 weeks). The mean duration between occurrence of RD and vitrectomy was 4.8 ± 3.0 days (range, 1–9 days). After vitrectomy, all retinas were still attached at the last follow-up visit.
Virological analysis
The mean viral DNA load at presentation was 5.7 × 107 ± 9.7 × 107 copies/mL (range, 8.6 × 105–3.7 × 108/mL). The following changes of viral DNA load were described in the DNA curves (Fig. 2). The viral DNA profile in the aqueous humour displayed a kinetic pattern of decline after starting antiviral treatment, including a plateau phase and a logarithmic reduction phase [12, 13].

Circles: time at which active retinitis disappearance was first found. Crosses: time at which retinal detachment occurred. Both the circles and crosses mark the early termination of intravitreal injection and real-time qPCR analysis in the first 4-week’s antiviral treatment.
The plateau phase was defined as the period before a biologically significant decline of viral DNA load was observed (a decrease in viral DNA load of 0.5 log from baseline) [13], and was found to be within 1 week in six eyes (30.0%; Patient 3,6,9,10,17,19), between 1 and 2 weeks in 12 eyes (60.0%; Patient 1,2,4,5,7,8,11–15,18), and between 2 and 3 weeks in one eye (5.0%; Patient 16). We could not assess the plateau phase in one eye (Patient 20), which had limited measurements because of early RD.
After the viral load achieved a biologically significant decline, the viral kinetics of reduction were evaluated in eight patients (Patient 4,6–9,11,17,19) with a minimum of three samples collected after the time point of 0.5 log decrease in viral DNA load from baseline. There was an exponential decrease in the viral DNA load, and in 6 of the 8 eyes (Patient 4,6–9,11), the correlation was significant using linear regression analysis (P < 0.05). The mean slope of the decline of the base 10 logarithm of viral DNA load was −0.103 ± 0.029 log/day (range, −0.150 to −0.060 log/day). The expected time for half reduction in the initial viral DNA load was 3.2 ± 1.0 days (range, 2.0–5.0 days).
At the end of the first 4-week’s antiviral treatment, the mean viral DNA load decreased to 3.1 × 104 ± 1.8 × 104 copies/mL (range, 1.6 × 104–6.0 × 104 copies/mL; P = 0.012). At the end of the first 8-week’s antiviral treatment, the viral DNA load was below detection threshold in all 20 eyes (100.0%).
Relationship between visual outcome and virological parameters determined by real-time qPCR
The relationships between visual outcome and virological parameters determined by real-time qPCR were shown in Table 2. The logMAR BCVA at the last follow-up was assessed in a stepwise multivariable regression model (including initial retinal quadrants involved, initial retinal zones involved, occurrence of RD and initial viral DNA load). The parameter that remained independently associated with logMAR BCVA at the last follow-up was the initial viral DNA load (β = 0.745, P < 0.001).
Discussion
In the present study, we measured changes in the viral DNA load of aqueous humour samples in VZV-induced ARN patients and investigated the visual outcomes. As far as we know, this is the largest series of VZV-induced ARN patients treated under uniform antiviral therapy in a short time span.
The quantitative measurement of viral DNA load using real-time qPCR has recently been described for ocular infections by VZV, including patients with ARN [6, 14], which has become a reliable tool to monitor the extent of disease, especially in eyes with media opacity [5]. The observation by D. Bernheim et al. first depicted the kinetics of viral DNA load in aqueous humour samples during treatment in six patients of VZV-induced ARN [13]. All these publications were performed with small samples, which need to be validated in a substantial series.
In the present study, the initial viral DNA load covered a large dynamic range from 8.6 × 105 to 3.7 × 108 copies /mL, comparable to the studies published before [6, 13, 14]. In the study by Charles et al., initial viral DNA load of ≥5.0 × 106 copies/mL was associated with worse visual acuity, which was similar to what was found in the present study [14]. In the present study, the initial viral DNA load was the independent predictive factor of logMAR BCVA at the last follow-up (β = 0.745, P < 0.001).
Just as what has reported before, once antiviral treatment began, the profile of viral DNA load in the aqueous humour follows a well-defined kinetic pattern of virus clearance with a plateau phase and a following logarithmic reduction phase [12, 13]. The plateau phase was found to be within 2 weeks in most of the eyes (18 eyes, 90.0%) in the present study. This seems to be shorter than what was reported in Bernheim’s study (mean, 27.8 days; range, 10–77 days) [13]. The length of plateau phase is reported to be related to a series of factors including the host immune responses and the choice of antiviral therapy [15, 16]. The antiviral susceptibility of the causal virus is also thought to be related to the length of plateau phase [13], and in Hafidi’s study, the patients with antiviral resistance shared a longer plateau phase of viral DNA load [17].
The kinetics of the viral DNA load might be a useful tool for evaluating the clinical course of ARN and help determining the treatment schedule. The most established treatment regimen of ARN included an induction therapy of intravenous acyclovir for 7–10 days followed by a maintenance treatment of oral antivirals for a long period of time [2, 18]. The duration of the currently used intravenous induction dose was consistent with the mean length of the plateau phase of the viral DNA load shown by qPCR. A prolonged plateau phase monitored by real-time qPCR might suggest the antiviral resistance, and the need for a more prolonged high-dose antivirals or change for another antiviral medication in clinical practice [17, 19]. Interestingly, the plateau phase was not correlated with the initial viral DNA load (r = −0.269, P = 0.266), which suggests that there could be far more other issues involved, as the retinal permeability, drug pharmacokinetics, vascular infraction or occlusion, and so on.
Although observation of the length of plateau phase can help us speculate on the possible antiviral resistance, a VZV genotypic antiviral testing is important to validate this speculation. Currently antiviral drugs to treat VZV-associated infections mainly target the viral DNA polymerase (Pol) and viral thymidine kinase (TK); thus mutations in Pol and TK encoding genes confer resistance to antiviral drugs [20]. As a relatively new sequencing technology, ultra-deep sequencing has an enhanced sensitivity to detect minor variants and allows quantitative evaluation of the viral drug resistance mutations [21, 22]. Ultra-deep sequencing might provide us with the antiviral resistance more quickly and accurately, compared to observation of the plateau phase, and is worthy further exploration, which is not investigated in the present study.
Once the viral DNA load starts to decrease (after a viral DNA load decline of 0.5 log), most of the DNA curves behaved similarly, with mean slopes of decline of −0.103 ± 0.029 log/day, and a mean expected time for half reduction of the initial viral DNA load of 3.2 ± 1.0 days. This is consistent with the series reported by Bernheim et al. (3.0 ± 0.7 days) and Hafidi et al. (4.2 days) [13, 17]. Previous studies that measured the time-profile of viral DNA load of ARN patients with real-time qPCR are summarised in Table 3.
In the present study, at the end of the first 8-week’s antiviral treatment, the viral DNA load was below detection threshold in all 20 eyes (100.0%), which might provide some guidance on duration of antiviral maintenance treatment for ARN. Systemic antiviral treatment stopped at 8 weeks in the present series when viral DNA load was not detected, the duration was shorter than most other reports [18, 23, 24]. Long-term oral antiviral treatment is commonly used as maintenance treatment for ARN to stabilise the retina and avoid bilateral involvement. The duration varies greatly, typically many months in the previous published studies [2, 4], and the doctors were perhaps treating ARN for too long. An intensive antiviral treatment conducted in the present series might be one reason for this shorter antiviral duration, with cautious inference. This shorter duration of antiviral treatment can reduce the financial burden and the risk of liver or renal dysfunction. Whether this shorter course of treatment would increase the risk of contralateral eye involvement needs further observation. Firstly, bilateral ARN often results from delays in the initial diagnosis and treatment of the first involved eye [25], while in the present series all eyes were treated with a timely antiviral therapy. Secondly, as Palay et al. investigated, the risk of contralateral eye involvement was greatest in the first 14 weeks after diagnosis [26]; in the present series except for one patient suffering from bilateral ARN at initial presentation, the remaining 19 patients did not suffer from fellow eye involvement after a follow-up of more than 6 months. The incidence of contralateral eye involvement was not higher than that of 11.10–22.70% in prior studies [23, 27, 28]. After the first eye was actively infected by virus, it becomes latent in sensory neurons. The balance of the host’s immune responses and viral status determined whether and when the contralateral eye will be involved. In some patients, contralateral eye involvement may occur even several years later [25]. There is no evidence on the length of antiviral treatment required to prevent contralateral eye involvement after the viral load turns negative in the affected eye. Thus, we administered antiviral treatment until the viral load turned negative in the affected eye, and carefully observed the contralateral eye.
The strengths of this study include its larger sample size of VZV-induced ARN patients compared with other similar studies, a consistent pathogenic virus in all cases, and the same antiviral therapy used in all patients. However, the study also had several limitations. Firstly, the study was retrospective and the patient data were reviewed from medical records. Secondly, for some patients with mild disease or early RD, the number of aqueous humour samples acquired was limited, resulting in the disability of some statistical analyses. Thirdly, antiviral resistance was not investigated in the series, which is valuable for developing personalised antiviral treatment. Finally, although continuous aqueous sampling and qPCR measurements are useful in the treatment for ARN, the procedure must be conducted with caution considering its invasive nature; explorations for other noninvasive indicators to guide treatment for ARN are needed in the following studies.
In conclusion, real-time qPCR is useful in monitoring the changes of viral DNA load in aqueous humour samples in VZV-induced ARN patients, which followed a clearance kinetics including a plateau phase and a logarithmic reduction phase. Compared with a single simple PCR test, the viral DNA load kinetics measured by continuous real-time qPCR might be useful to monitor the therapeutic efficacy and decide the needed antiviral duration in VZV-induced ARN patients.
Summary
What was known before
-
ARN is caused by herpes virus family infection, with VZV the most common causative pathogen.
-
The viral DNA load reflects the extent of disease and response to antiviral treatment.
What this study adds
-
The viral load displayed a kinetic pattern of decline after starting antiviral treatment, including a plateau phase and a logarithmic reduction phase.
-
The viral load was below detection threshold after 8-weeks’ antiviral treatment.
-
The observation of viral load changes by qPCR was useful for better monitoring of therapeutic efficacy and deciding needed antiviral duration in VZV-induced ARN patients.
References
Urayama A. Unilateral acute uveitis with retinal peri-arteritis and detachment. Jpn J Clin Ophthalmol. 1971;25:607e19.
Schoenberger SD, Kim SJ, Thorne JE, Mruthyunjaya P, Yeh S, Bakri SJ, et al. Diagnosis and Treatment of Acute Retinal Necrosis: a Report by the American Academy of Ophthalmology. Ophthalmology. 2017;124:382–92.
Holland GN. Standard diagnostic criteria for the acute retinal necrosis syndrome. Executive Committee of the American Uveitis Society. Am J Ophthalmol. 1994;117:663–7.
Wong RW, Jumper JM, McDonald HR, Johnson RN, Fu A, Lujan BJ, et al. Emerging concepts in the management of acute retinal necrosis. Br J Ophthalmol. 2013;97:545–52.
Dworkin LL, Gibler TM, Van Gelder RN. Real-time quantitative polymerase chain reaction diagnosis of infectious posterior uveitis. Arch Ophthalmol. 2002;120:1534–9.
Asano S, Yoshikawa T, Kimura H, Enomoto Y, Ohashi M, Terasaki H, et al. Monitoring herpesvirus DNA in three cases of acute retinal necrosis by real-time PCR. J Clin Virol. 2004;29:206–9.
Cottet L, Kaiser L, Hirsch HH, Baglivo E. HSV2 acute retinal necrosis: diagnosis and monitoring with quantitative polymerase chain reaction. Int Ophthalmol. 2009;29:199–201.
Holland GN, Buhles WC Jr, Mastre B, Kaplan HJ. UCLA CMV Retinopathy Study Group. A controlled retrospective study of ganciclovir treatment for cytomegalovirus retinopathy. Use of a standardized system for the assessment of disease outcome. Arch Ophthalmol. 1989;107:1759–66.
Holladay JT. Visual acuity measurements. J Cataract Refract Surg. 2004;30:287–90.
Espy MJ, Teo R, Ross TK, Svien KA, Wold AD, Uhl JR, et al. Diagnosis of varicella-zoster virus infections in the clinical laboratory by LightCycler PCR. J Clin Microbiol. 2000;38:3187–9.
Kido S, Sugita S, Horie S, Miyanaga M, Miyata K, Shimizu N, et al. Association of varicella zoster virus load in the aqueous humour with clinical manifestations of anterior uveitis in herpes zoster ophthalmicus and zoster sine herpete. Br J Ophthalmol. 2008;92:505–8.
Roberts TC, Brennan DC, Buller RS, Gaudreault-Keener M, Schnitzler MA, Sternhell KE, et al. Quantitative polymerase chain reaction to predict occurrence of symptomatic cytomegalovirus infection and assess response to ganciclovir therapy in renal transplant recipients. J Infect Dis. 1998;178:626–35.
Bernheim D, Germi R, Labetoulle M, Romanet JP, Morand P, Chiquet C. Time profile of viral DNA in aqueous humour samples of patients treated for varicella-zoster virus acute retinal necrosis by use of quantitative real-time PCR. J Clin Microbiol. 2013;51:2160–6.
Calvo CM, Khan MA, Mehta S, Garg SJ, Dunn JP. Correlation of Clinical Outcomes with Quantitative Polymerase Chain Reaction DNA Copy Number in Patients with Acute Retinal Necrosis. Ocul Immunol Inflamm. 2017;25:246–52.
Rochat C, Polla BS, Herbort CP. Immunological profiles in patients with acute retinal necrosis. Graefes Arch Clin Exp Ophthalmol. 1996;234:547–52.
Guex-Crosier Y, Rochat C, Herbort CP. Necrotizing herpetic retinopathies. A spectrum of herpes virus-induced diseases determined by the immune state of the host. Ocul Immunol Inflamm. 1997;5:259–65.
Hafidi M, Manificat HJ, Denis P, Charleux B, Rabilloud M, Boibieux A, et al. Acute Retinal Necrosis: virological Features Using Quantitative Polymerase Chain Reaction, Therapeutic Management, and Clinical Outcomes. Am J Ophthalmol. 2019;208:376–86.
Tibbetts MD, Shah CP, Young LH, Duker JS, Maguire JI, Morley MG. Treatment of acute retinal necrosis. Ophthalmology. 2010;117:818–24.
Andrei G, Topalis D, Fiten P, McGuigan C, Balzarini J, Opdenakker G, et al. In vitro-selected drug-resistant varicella-zoster virus mutants in the thymidine kinase and DNA polymerase genes yield novel phenotype-genotype associations and highlight differences between antiherpesvirus drugs. J Virol. 2012;86:2641–52.
Piret J, Boivin G. Antiviral resistance in herpes simplex virus and varicella-zoster virus infections: diagnosis and management. Curr Opin Infect Dis. 2016;29:654–62.
Mercier-Darty M, Boutolleau D, Lepeule R, Rodriguez C, Burrel S. Utility of ultra-deep sequencing for detection of varicella-zoster virus antiviral resistance mutations. Antivir Res. 2018;151:20–23.
Mercier-Darty M, Boutolleau D, Rodriguez C, Burrel S. Added value of ultra-deep sequencing (UDS) approach for detection of genotypic antiviral resistance of herpes simplex virus (HSV). Antivir Res. 2019;168:128–33.
Roy R, Pal BP, Mathur G, Rao C, Das D, Biswas J. Acute retinal necrosis: clinical features, management and outcomes-a 10-year consecutive case series. Ocul Immunol Inflamm. 2014;22:170–4.
Baltinas J, Lightman S, Tomkins-Netzer O. Comparing Treatment of Acute Retinal Necrosis With Either Oral Valacyclovir or Intravenous Acyclovir. Am J Ophthalmol. 2018;188:173–80.
Lei BY, Jiang R, Wang ZJ, Xu GZ, Wu XY, Zhou M. Bilateral acute retinal necrosis: a case series. Retina. 2020;40:145–53.
Palay DA, Sternberg P Jr, Davis J, Lewis H, Holland GN, Mieler WF, et al. Decrease in the risk of bilateral acute retinal necrosis by acyclovir therapy. Am J Ophthalmol. 1991;112:250–5.
Lau CH, Missotten T, Salzmann J, Lightman SL. Acute retinal necrosis features, management, and outcomes. Ophthalmology. 2007;114:756–62.
Hillenkamp J, Nölle B, Bruns C, Rautenberg P, Fickenscher H, Roider J. Acute retinal necrosis: clinical features, early vitrectomy, and outcomes. Ophthalmology. 2009;116:1971–15.
Acknowledgements
The authors thank Jianhong Dong and Zhijian Jiang (Shanghai Xuhui Central Hospital) for collecting data, and thank all patients involved in the study for their contributions in sample collection.
Funding
This work was supported by the National Natural Science Foundation of China (Grant no. 81770944 and 81700862), Grant from Science and Technology Commission of Shanghai Municipality (Grant no. 16411953700 and 18411965100), Xuhui District Health and Family Planning Commission Key Disease Joint Project (XHLHGG201807).
Author information
Authors and Affiliations
Contributions
BL and ZW contributed equally to the paper. BL and MZ designed the study. The main part of the paper was drafted by BL and ZW. The paper was revised by QC, GX and MZ. Clinical data were collected, interpretated and added to the paper by BL, QS, RG, YZ and RJ. PCR analysis were conducted by ZW.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lei, B., Wang, Z., Shu, Q. et al. Observation of varicella zoster virus-induced acute retinal necrosis: viral load detection and visual outcome. Eye 36, 1209–1216 (2022). https://doi.org/10.1038/s41433-021-01609-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01609-8
This article is cited by
-
False negative result of polymerase chain reaction in very early stages of acute retinal necrosis
Journal of Ophthalmic Inflammation and Infection (2023)
