
Abstract
Objective
To investigate the association between exposure to topical ophthalmic antibiotics during pregnancy and adverse neonatal outcomes.
Methods
In this retrospective cohort study, we identified pregnant women with hordeola, chalazia, blepharitis, or bacterial conjunctivitis from 2005 to 2018 using the Japanese Medical Data Centre Claims Database. From the eligible women, we extracted women who were dispensed no topical antibiotics during the first trimester (non-antibiotic group), women who were dispensed topical fluoroquinolones alone at least once (fluoroquinolone alone group), and women who were dispensed any single type of antibiotic (single-antibiotic group). We compared the frequency of congenital anomalies (CA), preterm birth (PB), low birth weight (LBW), and the composite outcome of these three between the fluoroquinolone and non-antibiotic groups and between the single-antibiotic and non-antibiotic groups, using propensity score adjustment.
Results
A total of 891 eligible women were identified. In the fluoroquinolone (n = 409) and non-antibiotic (n = 309) groups, CA occurred in 6.8% and 6.8%, PB in 2.4% and 3.2%, LBW in 2.9% and 3.2%, and the composite outcome in 10.5% and 11.3%, respectively. Analysis using propensity score adjustment showed no significant difference between the groups in the frequency of CA (adjusted odds ratio, 1.15; 95% confidence interval, 0.61–2.18), PB (0.80; 0.30–2.17), LBW (1.08; 0.45–2.63), or the composite outcome (1.12; 0.67–1.87). Comparison of the single-antibiotic and non-antibiotic groups showed similar results.
Conclusions
Topical ophthalmic antibiotics for hordeola, chalazia, blepharitis, or bacterial conjunctivitis during the first trimester were not associated with increased adverse neonatal outcomes.
Similar content being viewed by others

Introduction
Hordeola, chalazia, and blepharitis are disorders characterized by swollen red eyelids. These diseases are common in all ethnic groups and found across all ages, including women of child-bearing age (from late teens to 40s) [1,2,3]. Although the pathophysiology of the three diseases differs, their treatments are very similar. Treatment options include warm compresses, lid scrubs, lid massage, and antibiotics (topical or systemic), and these are often used in combination [1, 4, 5]. Antibiotics are expected to shorten the healing time [1] and relieve symptoms in moderate to severe cases [4]. Similarly, although bacterial conjunctivitis can occur in pregnant women and mostly resolves on its own, topical antibiotics are sometimes used to decrease the duration of symptoms [6]. However, topical antibiotics should be administered to pregnant women with caution because of their possible adverse effects on the foetus.
In many countries, fluoroquinolones are frequently chosen for treatment of ocular infections including hordeola, chalazia, blepharitis, and bacterial conjunctivitis [7,8,9]. Some studies have shown fluoroquinolone-associated teratogenicity in animals [10,11,12], while some meta-analyses of human patients have shown that fluoroquinolones were not associated with adverse neonatal outcomes such as congenital anomalies, preterm birth, and low birth weight [13, 14]. However, these previous studies focused on systemic administration of fluoroquinolones; the safety of topical administration remains unknown. Because eye drops or ointments do not undergo first-pass metabolism in the liver [15], they might affect foetuses differently than systemic administration.
We therefore aimed to clarify the association between the use of topical antibiotics such as fluoroquinolones during pregnancy and adverse neonatal outcomes such as congenital anomalies, preterm birth, and low birth weight using a large claims database in Japan.
Materials and methods
Data source
We used the Japanese Medical Data Centre (JMDC) Claims Database (JMDC Inc., Tokyo, Japan) to perform a retrospective cohort study [16]. In 2018, the JMDC collected health insurance claims data for >5 million people from ≥200 large Japanese companies. The JMDC database contains the following anonymized individual-level data on both outpatients and inpatients: unique identifiers; family identifiers; patient characteristics (age and sex); period from start to end of the insurance; relationship to the insured individual (main insured, spouse, or child); diagnoses based on the International Classification of Diseases, Tenth Revision (ICD-10); procedures performed based on Japanese original codes; and drugs prescribed based on the Anatomical Therapeutic Chemical Classification System (ATC). This study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of The University of Tokyo. The need for informed consent was waived because all data were fully de-identified.
Patient selection
We used data from 2005 to 2018 and identified neonates born during this period. We linked neonates to their mothers using family identifiers. Using ICD-10 codes, we categorized the neonates into the following three gestational age groups: preterm birth (22–27 weeks), preterm birth (28–36 weeks), and full-term birth (≥37 weeks) (Supplementary Table 1). The start of pregnancy for these three categories was defined as 6, 7, and 9 months before the month of delivery, respectively [17]. The first trimester was defined as the first 3 months of pregnancy (gestational weeks 0–13) (Fig. 1).

Identification of first trimester.
The exclusion criteria were as follows: (1) mothers with an insurance period of <6 months before the start of pregnancy because we needed information on potential confounders during that period, (2) neonates with a follow-up period of <6 months after birth because we needed information on neonatal adverse outcomes during that period [18], and (3) mothers whose insurance status was “main insured” (not a dependent) because they may quit their jobs and change insurance around childbirth, leading to difficulty in follow-up.
We then identified women who were diagnosed with hordeola or chalazia (corresponding to ICD-10 code H00), blepharitis (H01), and bacterial conjunctivitis (B99, H102, and H131) during the first trimester. The first trimester is vital for normal foetal development because birth anomalies occur during this period [18, 19]. We thus excluded women exposed to known teratogenic drugs during the first trimester (Supplementary Table 2) [20].
Outcomes
Outcomes included congenital anomalies, preterm birth, low birth weight, and the composite of the three outcomes during the 6 months after delivery (Supplementary Table 1) [19]. We did not regard minor anomalies that may not be associated with medication use during pregnancy as outcomes, as reported in a previous study [18].
Exposure
The eligible women were divided into the non-antibiotic and antibiotic groups. The non-antibiotic group comprised women who were not dispensed any type of topical antibiotics during the first trimester. From the antibiotic group, we extracted patients who were dispensed any single type of topical antibiotic during the first trimester (the single-antibiotic group). Furthermore, we extracted patients who were dispensed topical fluoroquinolones alone at least once and were not dispensed any other type of topical antibiotics during the first trimester (the fluoroquinolone alone group). Dispensation of antibiotics including eye drops and ointment was identified using ATC codes or brand names (Supplementary Table 3). Because only one kind of antibiotic eye drop (sulpha drug) is sold over the counter in Japan, this study likely included few women who actually used antibiotics but were misclassified into the non-antibiotic group.
Potential confounders
Potential confounders included the following [20,21,22,23,24,25]; (1) maternal age, (2) year of birth, (3) disorders during pregnancy (multiple pregnancy, hypertensive disorders of pregnancy, gestational diabetes, and maternal infection), (4) other chronic comorbidities (anaemia, hypertension, diabetes mellitus, gastroduodenal ulcer, thyroid disorders, asthma, atopy, epilepsy, endometriosis, and depression and anxiety), and (5) medications (systemic antibiotics, topical ophthalmic corticosteroids, ophthalmic or systemic antihistamines, and metoclopramide) during the first trimester. ICD-10 and ATC codes were used to identify these potential confounders (Supplementary Table 4). Any woman with relevant ICD-10 and ATC codes from 6 months before the start of pregnancy to the month of delivery were considered to have these chronic comorbidities, as described previously [19]. The use of medications was considered present if the medications were dispensed during the first trimester.
Statistical analysis
The baseline characteristics were compared (1) between the fluoroquinolone alone group and the non-antibiotic group and (2) between the single-antibiotic group and the non-antibiotic group. The t-test was used for continuous variables such as age, and the χ2 test was used for categorical variables such as the presence of hypertension.
We conducted propensity score (PS) adjustment analyses to compare the adverse neonatal outcomes (1) between the fluoroquinolone alone group and the non-antibiotic group and (2) between the single-antibiotic group and the non-antibiotic group. First, we performed logistic regression analyses in which the use of topical fluoroquinolones alone (or any single antibiotic) was the response variable and the potential confounders were explanatory variables. Second, we estimated the causal effect of topical fluoroquinolones alone (or any single antibiotic) on adverse neonatal outcomes by constructing a logistic regression model with PS adjustment. In this model, adverse neonatal outcomes were regressed on the use of topical fluoroquinolones alone (or any single antibiotic) and the estimated PS. We used PS adjustment analyses rather than conventional logistic regression because PS analyses are more robust and more unbiased than conventional logistic regression when the number of events per confounder is small [26].
Sensitivity analyses were conducted to enhance the robustness of the main analysis results. In the first sensitivity analysis, we excluded women who were dispensed any topical antibiotics during the 3 months before the start of pregnancy to prevent contamination of the control group (unexposed women) with women who still had the topical antibiotics at hand after the start of pregnancy [27]. In the second sensitivity analysis, we excluded women who had received systemic antibiotics during the first trimester.
We used the statistical programming language R (R version 3.6.1; R Foundation for Statistical Computing, Vienna, Austria) for all statistical analyses. A significance level of 0.05 was used.
Results
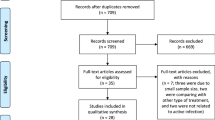
Hordeola, chalazia, or blepharitis were found in 955 (1.1%) of 84,803 mothers, 929 of whom were finally eligible for the current study (Fig. 2).

aNo topical ophthalmic antibiotics were dispensed during the first trimester. bAny single type of topical antibiotic was dispensed during the first trimester. cTopical fluoroquinolones alone were dispensed at least once and no other type of topical antibiotic was dispensed during the first trimester.
Table 1 shows the numbers of women who received each topical antibiotic. Of the 929 eligible women, 620 (67%) received ophthalmic topical antibiotics, and 309 (33%) women were not exposed to any topical antibiotics during the first trimester. Fluoroquinolones were most frequently dispensed (n = 500 [54%]), followed by aminoglycosides (n = 139 [15%]). A total of 522 (56%) women were dispensed one type of topical antibiotic, 409 (44%) of whom received fluoroquinolone alone (Fig. 2).
The baseline characteristics of the women in the fluoroquinolone alone group (n = 409) and the non-antibiotic group (n = 309) are shown in Table 2. Women in the non-antibiotic group were more likely to have skin infections and atopy and to receive oral antihistamines and corticosteroid ointment, and those in the fluoroquinolone alone group were more likely to receive systemic antibiotics and corticosteroid eye drops. Comparison of the baseline characteristics of the single-antibiotic and the non-antibiotic groups showed similar results.
Adverse neonatal outcomes for women in the fluoroquinolone alone group and non-antibiotic group are shown in Table 3. The proportions of neonates with congenital anomalies, preterm birth, low birth weight, and the composite outcome in the fluoroquinolone alone group and non-antibiotic group were 6.8% and 6.8%, 2.4% and 3.2%, 2.9% and 3.2%, and 10.5% and 11.3%, respectively.
After PS adjustment, there was no significant difference between the fluoroquinolone alone and non-antibiotic groups in the frequency of congenital anomalies (adjusted odds ratio [aOR], 1.15; 95% confidence interval [CI], 0.61–2.18; P = 0.67), preterm birth (aOR, 0.80; 95% CI, 0.30–2.17; P = 0.66), low birth weight (aOR, 1.08; 95% CI, 0.45–2.63; P = 0.86), or the composite outcome (aOR, 1.12; 95% CI, 0.67–1.87; P = 0.67) (Table 3).
Similarly, there was no significant difference between the single-antibiotic and non-antibiotic groups (Table 3).
The sensitivity analyses also showed similar results (Supplementary Tables 5 and 6).
Discussion
In the current study using a large claims database with PS adjustment for various confounders, adverse neonatal outcomes (congenital anomalies, preterm birth, low birth weight, and the composite outcome) were not significantly associated with exposure to topical ophthalmic antibiotics during pregnancy.
In the current study, the overall proportion of individuals with hordeola, chalazia, or blepharitis was 1.1%. A database study in the United Kingdom showed that hordeola/chalazia, blepharitis, and bacterial conjunctivitis were found in 3.7%, 0.6%, and 2.4% of a population without rosacea, respectively, during a 15-month observation period [28]. Because the current study defined the inclusion period as the first trimester (one-fifth of 15 months), the proportion of 1.1% is comparable.
Hordeola, chalazia, and bacterial conjunctivitis spontaneously resolve without treatment in many cases, and they resolve with conservative therapy such as warm compresses in other cases [1, 6, 29]. In addition, blepharitis is not a vision-threatening emergency disease. Thus, if possible, the use of antibiotics in pregnant women should be avoided. However, antibiotics are expected to reduce such symptoms [4] and to help the disease resolve more quickly [1]. If marked swelling is present (indicating that the infection is severe) [1] or if a pregnant woman is experiencing severe pain, discomfort, or cosmetic deterioration [1, 2, 4], ophthalmologists must decide whether to prescribe antibiotics. It is therefore important to provide pregnant women with information on the safety of antibiotics.
In the current study, 66% of the eligible pregnant women with hordeola, chalazia, blepharitis, or bacterial conjunctivitis received topical antibiotics during the first trimester. This high proportion suggests that ophthalmologists attach more weight to improving symptoms and preventing spread of inflammation than to the risk of adverse effects on foetuses. Another possible explanation is that some women may not have yet realized that they are pregnant in the first trimester, and ophthalmologists thus routinely prescribe antibiotics.
Infectious eye diseases are most frequently treated with fluoroquinolones in Japan [7]. Additionally, fluoroquinolones reportedly lead the market for ophthalmic antibiotics in the United States and Brazil [8]. The current study showed similar trends in which fluoroquinolones achieved a dominant share.
Fluoroquinolones have been reported to cause harm to foetuses in animal models [10,11,12]. For example, topical ophthalmic ofloxacin had adverse effects on rabbit foetuses [30]. However, the dosage needed to cause embryocidal effect was 160 mg/kg per day, which is 1800 times higher than the maximum volume recommended for daily ophthalmic use [30]. One study showed that in humans, the maximum serum ofloxacin concentration after 10 days of topical fluoroquinolone use was only 1.9 ng/mL, which was less than 1/1000 of the serum concentration reported after administration of oral fluoroquinolones [30]. Thus, the current finding that topical fluoroquinolones were not significantly associated with adverse neonatal outcomes is plausible in terms of pharmacokinetics.
In the current study, congenital anomalies occurred in 7.5% of all eligible women, which is comparable with previous reports (3.0%–8.6%) [19, 31, 32]. Preterm births and low birth weight occurred in 2.7% and 4.1%, respectively, of the women in the current study; this is somewhat lower than the reported proportions in previous studies (preterm birth, about 4.7% from 2009 to 2014; [33] low birth weight, 8.3% in 2010 [34]). This may have been caused by doctors’ underreporting of these events. However, because there is little possibility that underreporting accumulated only in either the fluoroquinolone or non-antibiotic group, the validity of the causal inference would not be severely threatened.
This study had several limitations. First, we were unable to obtain information on the usage and dosage of dispensed eye drops. This prevented us from investigating dose-dependent effects. Second, misclassification bias might have been present; whether the women actually used the eye drops that were dispensed is unclear. These could lead to potential underestimation of the risks. However, we were able to eliminate recall bias by using a claims database, unlike self-reported data. Third, the sample size may not have been large enough to make firm causal inferences. If we assume a two-fold increase in the risk of congenital anomalies in the fluoroquinolone alone group compared with the non-antibiotic group, the statistical power will be >80%. However, analyses for other outcomes, such as preterm birth and low birth weight, would be underpowered. This indicates the need to interpret the current results with caution. Fourth, eye drops and ointment were analysed collectively because if they had been separately analysed, the sample size would have been even smaller. Fifth, the administrative claims database did not contain information on punctal occlusion, which is a useful way to reduce systemic absorption of eye drops. Sixth, abortion and miscarriage could not be identified in the database. This may have led to underreporting of congenital anomalies.
Despite these limitations, given that randomized controlled trials involving pregnant women are difficult to perform because of ethical problems, the current results provide us valuable practical data.
Conclusions
The use of ophthalmic topical antibiotics for hordeola, chalazia, blepharitis, or bacterial conjunctivitis during the first trimester was not associated with adverse neonatal outcomes (congenital anomalies, preterm birth, low birth weight, and the composite outcome). These findings will be valuable when ophthalmologists prescribe topical antibiotics to pregnant women.
Summary
What was known before
-
Fluoroquinolones are frequently used for treatment of ocular infections including hordeola, chalazia, blepharitis, and bacterial conjunctivitis.
-
Safety of topical administration during pregnancy remains unknown.
What this study adds
-
Fluoroquinolones were most frequently used during the first trimester.
-
Topical antibiotics during pregnancy were not associated with adverse neonatal outcomes.
References
Lindsley K, Nichols JJ, Dickersin K. Interventions for acute internal hordeolum. Cochrane Database Syst Rev Online. 2010;9: CD007742.
Gilchrist H, Lee G. Management of chalazia in general practice. Aust Fam Physician. 2009;38:311–4.
Lindsley K, Matsumura S, Hatef E, Akpek EK. Interventions for chronic blepharitis. Cochrane Database Syst Rev. 2012;5:CD005556.
Amescua G, Akpek EK, Farid M, Garcia-Ferrer FJ, Lin A, Rhee MK, et al. Blepharitis preferred practice pattern®. Ophthalmology. 2019;126:P56–P93.
Fayers T, Loh GK, Cordeiro MF, Lee V, Jain R, Fayers PM. Overprescribing of antibiotics by UK ophthalmologists. Eye. 2018;32:240–2.
Azari AA, Barney NP. Conjunctivitis: a systematic review of diagnosis and treatment. JAMA. 2013;310:1721.
Deguchi H, Kitazawa K, Kayukawa K, Kondoh E, Fukumoto A, Yamasaki T, et al. The trend of resistance to antibiotics for ocular infection of Staphylococcus aureus, coagulase-negative staphylococci, and Corynebacterium compared with 10-years previous: A retrospective observational study. PLOS ONE. 2018;13:e0203705.
Kollross B, Gelfuso GM, Cunha-Filho M, Gratieri T, Kollross B, Gelfuso GM, et al. Topical ophthalmic antimicrobials: unfulfilled demands and possibility of new investments in Brazil and in the United States. Braz J Pharm Sci. 2019; 55. http://www.scielo.br/scielo.php?script=sci_abstract&pid=S1984-82502019000100573&lng=en&nrm=iso&tlng=en . Accessed 6 Aug 2020.
Jadhav PR, Moghe VV, Deshmukh YA. Drug utilization study in ophthalmology outpatients at a tertiary care teaching hospital. ISRN Pharmacol. 2013;2013. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3884865/. Accessed 6 Aug 2020.
Förster C, Rücker M, Shakibaei M, Baumann-Wilschke I, Vormann J, Stahlmann R. Effects of fluoroquinolones and magnesium deficiency in murine limb bud cultures. Arch Toxicol. 1998;72:411–9.
Da L, La H, Dg B. Quinolone-induced arthropathy in the neonatal mouse. Morphological analysis of articular lesions produced by pipemidic acid and ciprofloxacin. Fundam Appl Toxicol J Soc Toxicol. 1995;28:59–64.
Shakibaei M, Baumann-Wilschke I, Rücker M, Stahlmann R. Ultrastructural characterization of murine limb buds after in vitro exposure to grepafloxacin and other fluoroquinolones. Arch Toxicol. 2002;75:725–33.
Yefet E, Schwartz N, Chazan B, Salim R, Romano S, Nachum Z. The safety of quinolones and fluoroquinolones in pregnancy: a meta-analysis. BJOG Int J Obstet Gynaecol. 2018;125:1069–76.
Bar-Oz B, Moretti ME, Boskovic R, O’Brien L, Koren G. The safety of quinolones—a meta-analysis of pregnancy outcomes. Eur J Obstet Gynecol Reprod Biol. 2009;143:75–8.
Vaajanen A, Vapaatalo H. A single drop in the eye – effects on the whole body? Open Ophthalmol J. 2017;11:305–14.
Kimura S, Sato T, Ikeda S, Noda M, Nakayama T. Development of a database of health insurance claims: standardization of disease classifications and anonymous record linkage. J Epidemiol. 2010;20:413–9.
Spong CY. Defining “Term” pregnancy: recommendations from the defining “Term” pregnancy workgroup. JAMA. 2013;309:2445–6.
Bérard A, Sheehy O, Kurzinger M-L, Juhaeri J. Intranasal triamcinolone use during pregnancy and the risk of adverse pregnancy outcomes. J Allergy Clin Immunol. 2016;138:97–104.
Bérard A, Sheehy O, Zhao J-P, Gorgui J, Bernatsky S, de Moura CS, et al. Associations between low- and high-dose oral fluconazole and pregnancy outcomes: 3 nested case–control studies. Can Med Assoc J. 2019;191:E179–87.
Sheehy O, Zhao J-P, Bérard A. Association between incident exposure to benzodiazepines in early pregnancy and risk of spontaneous abortion. JAMA Psychiatry. 2019;76:948.
Goldenberg RL, Culhane JF, Iams JD, Romero R. Preterm Birth 1 Epidemiology and causes of preterm birth. Lancet. 2008;371:75–84.
Aldridge TD, Hartmann KE, Michels KA, Velez Edwards DR. First-trimester antihistamine exposure and risk of spontaneous abortion or preterm birth. Pharmacoepidemiol Drug Saf. 2014;23:1043–50.
Liang Z, Yin M, Ma M, Wang Y, Kuang Y. Effect of maternal advanced endometriosis on risk of congenital malformations for infants born after in vitro fertilization and frozen–thawed embryo transfer: analysis of 28,600 newborns. Front Endocrinol. 2019;10:763.
Lee BK, Magnusson C, Gardner RM, Blomström Å, Newschaffer CJ, Burstyn I, et al. Maternal hospitalization with infection during pregnancy and risk of autism spectrum disorders. Brain Behav Immun. 2015;44:100–5.
Ilan M, Rafael G, Gideon K, Eyal S, Arnon W, Amalia L. The safety of metoclopramide use in the first trimester of pregnancy. N Engl J Med. 2009;8:2528–35.
Cepeda MS. Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. Am J Epidemiol. 2003;158:280–7.
Huybrechts KF, Hernández-Díaz S, Straub L, Gray KJ, Zhu Y, Patorno E, et al. Association of maternal first-trimester ondansetron use with cardiac malformations and oral clefts in offspring. JAMA. 2018;320:2429.
Spoendlin J, Voegel JJ, Jick SS, Meier CR. A study on the epidemiology of rosacea in the U.K. Br J Dermatol. 2012;167:598–605.
Wu AY, Gervasio KA, Gergoudis KN, Wei C, Oestreicher JH, Harvey JT. Conservative therapy for chalazia: is it really effective? Acta Ophthalmol. 2018;96:e503–09.
International Council of Ophthalmology. Section 21 Ophthalmological Preparations. https://www.who.int/selection_medicines/committees/expert/19/applications/Ofloxacin_21_AC_Ad.pdf?ua=1 . Accessed 13 Aug 2020.
Egbe AC. Birth defects in the newborn population: race and ethnicity. Pediatr Neonatol. 2015;56:183–8.
Brent RL, Beckman DA. Environmental teratogens. Bull N. Y Acad Med. 1990;66:123–63.
Sakata S, Konishi S, Ng CFS, Watanabe C. Preterm birth rates in Japan from 1979 to 2014: analysis of national vital statistics: preterm birth rates in Japan. J Obstet Gynaecol Res. 2018;44:390–6.
Takemoto Y, Ota E, Yoneoka D, Mori R, Takeda S. Japanese secular trends in birthweight and the prevalence of low birthweight infants during the last three decades: a population-based study. Sci Rep. 2016;6:31396.
Funding
This work was supported by grants from the Ministry of Health, Labour and Welfare, Japan (19AA2007) and the Ministry of Education, Culture, Sports, Science and Technology, Japan (20H03907 and 17H05077). The sponsor or funding organization had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
YH had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: YH, H Yamana, DS, KM, H Yasunaga, and MA. Acquisition, analysis, and interpretation of data: YH, H Yamana, HM, and H Yasunaga. Drafting of the manuscript: YH, NM, H Yamana, DS, H Yasunaga, and MA. Critical revision of the manuscript for important intellectual content: YH. Statistical analysis: YH, H Yamana, DS, KM, and H Yasunaga. Obtained funding: H Yamana. Administrative, technical, or material support: None. Study supervision: H Yasunaga and MA.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hashimoto, Y., Michihata, N., Yamana, H. et al. Safety of topical ophthalmic antibiotics in pregnant women with hordeola, chalazia, blepharitis, or bacterial conjunctivitis: propensity score analyses. Eye 36, 1066–1073 (2022). https://doi.org/10.1038/s41433-021-01586-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01586-y
