
Abstract
Background
To investigate trends in the prevalence of reduced visual acuity (VA), a proxy measure for myopia, in an urban district in China.
Methods
Data were extracted from the dataset of the 2002 and 2018 Annual Survey on Students’ Constitution and Health from Yuhua District, Changsha City, China. Children aged 6–15 years were included in the study. VA was measured using a LogMAR tumbling E chart. The prevalence of reduced VA was calculated by age and gender. The chi-square test was used to compare the differences between groups.
Results
The final VA analysis included 26217 children in 2002 and 45510 children in 2018. The overall prevalence of reduced VA increased from 28.3% in 2002 to 46.5% in 2018 (P < 0.001). The prevalence of reduced VA started to increase markedly from the age of 14 years in 2002, while in 2018 it started to increase markedly from the age of 9 years. The prevalence of severely reduced VA increased in all age groups from 2002 to 2018 and increased with age (all P < 0.001). In 2002, over 50% of children in all age groups had normal VA. By 2018, the prevalence of normal VA decreased from 61.4% in those aged 6 years to 31.9% in those aged 15 years.
Conclusions
The prevalence of reduced VA among children aged 6–15 years in Yuhua District has become more common with age, and there has been a marked increase in the prevalence of reduced VA from 2002 to 2018. The remarkable epidemic of reduced VA started 5 years earlier in 2018 than in 2002. Evidence from the present study suggests that interventions should be launched before the age of 9 years.
Similar content being viewed by others


Introduction
Myopia is the most common eye disease affecting the eyesight of children and adolescents [1]. It increases the risk of eye complications, including retinopathy, glaucoma, retinal detachment, and blindness [2, 3]. Many epidemiological studies have confirmed that near work is a major risk factor associated with myopia. Other commonly associated factors include a high educational level of children and parents, females, and less outdoor activity [4,5,6].
In East Asia, such as the Chinese mainland, Taiwan, and Korea, where nearly 80% of adolescents are affected by myopia, the myopia epidemic has become a public health threat [7, 8]. Therefore, it is one of the main priorities of the five vision 2020 initiatives launched by the World Health Organisation (WHO) [9]. China, with its rapid economic development and transitions in behaviour and lifestyle, is one of the countries with the highest rates of childhood myopia in the world [10]. The Chinese government now pays more attention than ever before to the eyesight health of children and adolescents.
Using visual examination data from the dataset of 2002 and 2018 Annual Survey on Students’ Constitution and Health from Yuhua District, Changsha City, China, this study aimed to investigate trends in the prevalence of reduced visual acuity (VA), a proxy measure for myopia, in an urban district in China.
Methods
Study subjects
Changsha, the capital of the Hunan province of central China, has more than 3.5 million residents living in six urban districts. It has a well-developed elementary and secondary education system, all school-aged children complete 9 years of compulsory education in elementary school (6 years) and secondary school (3 years). We performed the analysis using data extracted from the dataset of the 2002 and 2018 Annual Survey on Students’ Constitution and Health from Yuhua District, Changsha City, China. The random cluster sampling method was used to select elementary and secondary schools from the Yuhua District. All students from the selected schools underwent visual examinations according to the manual of the National Student Constitution and Health Survey (Chinese version). Children aged less than 6 years or older than 15 years from the dataset were excluded from the analysis. We collected general information including name, gender, age, and the name of the school of all participants.
VA determinations
VA was measured using a retroilluminated LogMAR chart with tumbling E optotypes (Precision Vision). The specific measurement method was as follows: (1) The fourth line from the bottom (6/6) was set at the same height as the eye being tested. (2) Both eyes were examined separately, first the right eye, and then the left eye. (3) Measurements started at a distance of 5 m, starting from the fourth line from the bottom (6/6), using a staircase protocol, four of the five optotypes identified were considered as correct. (4) The VA equals the lowest line reading successfully. (5) If the top line was not read, the child would move forward until he could read. The protocol of VA examinations was the same in both surveys. Presenting and best-corrected VA were not measured.
Normal VA was defined as equal to or greater than 6/6. Mildly reduced VA was defined as greater than 6/9 and less than 6/6. Moderately reduced VA was defined as greater than 6/18, equal to or less than 6/9. Severely reduced VA was defined as equal to or less than 6/18 [11].
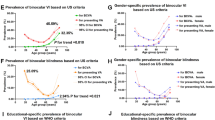
The definitions of VA categories in our study were different from those defined by the WHO and International Council of Ophthalmology (ICO) [7, 12]. In this study, the definition of reduced VA was based on an unaided distance VA of less than 6/6 in the worse eye. The WHO definition of visual impairment (VI) is based on presenting VA of less than 6/18 in the better eye, while that of the ICO is based on an unaided distance VA worse than 6/7.5 in the worse eye. The VI in the WHO definition is more severe than that recognised in the ICO definition. Our definition of moderately and severely reduced unaided VA covered the WHO categories of moderate and severe vision impairment and blindness, but was broader. According to WHO definitions, our definition of mild and moderate reduced VA is not VI. These methodological differences limit the comparison of our results with those of many other countries.
Statistical analysis
The prevalence of reduced VA and severely reduced VA were calculated by age and gender. The chi-square test was used to compare the differences between groups. The Cochran–Armitage test was used to examine the age trends for the prevalence of severely reduced VA. All statistical analyses were performed using SPSS version 22.0 (IBM, New York, USA). The figures were plotted using Microsoft Excel 2007. All P values were two-sided and P < 0.05 was considered significant for all tests.
Results
A total of 26,644 children in 2002 and 45,696 in 2018 were evaluated. A total of 427 children in 2002 and 186 children in 2018 were excluded from the analysis because of incomplete information. The final analysis included 26,217 children in 2002 and 45,510 children in 2018. There were no significant differences in age and gender between the two surveys (P > 0.05).
Table 1 shows that the overall prevalence of reduced VA increased from 28.3% (95% CI, 27.8–28.9%) in 2002 to 46.5% (95% CI, 46.0–46.9%) in 2018 (P < 0.001).
Table 2 shows the prevalence of reduced VA stratified by age and gender.
Reduced VA was more prevalent across age groups in 2018 than in 2002, except for the 6–8-year age group (P < 0.001). The prevalence of reduced VA increased from 24.8% in 2002 to 43.2% in 2018 for boys and from 32.3 to 50.2% for girls (P < 0.001).
Figure 1 shows that in 2002, the prevalence of reduced VA in the 6–10-year olds was very high and there was a decreasing trend from age 6 to 10 years. The prevalence of reduced VA in children aged 6–7 years in 2018 was decreased compared to 2002. In 2002 and 2018, the prevalence of reduced VA was higher among girls than boys in all age groups. In 2018, the prevalence of reduced VA started to increase markedly from the age of 9 years, while in 2002, it started to increase markedly from the age of 14 years.

Line graph represented the prevalence of reduced VA in children aged 6 to 15 years by year and sex.
Table 3 shows that the prevalence of severely reduced VA increased in all age groups from 2002 to 2018 and increased with age (all P < 0.001). The prevalence of severely reduced VA increased from 14.9% in 15-year olds in 2002 to 38.6% in 15-year olds in 2018 (all P < 0.001).
Figures 2 and 3 shows the percentages of students with normal, mildly, moderately, and severely reduced visual acuity in 2002 and 2018. In 2002, normal VA accounted for the majority of all age groups. In 2018, the proportion of normal VA in 15-year olds was only 31.9% (Figs. 2 and 3).

Percent bar chart represented the percentages of the four different vision conditions at each age.

Percent bar chart represented the percentages of the four different vision conditions at each age.
Discussion
In this population-based study on school children aged 6–15 years in Changsha, we found that there has been a significant increase in the overall prevalence of reduced unaided VA from 2002 to 2018. In 2002, 71.7% of children had normal VA, while only 53.5% had normal VA in 2018. Sun reported that the overall prevalence of reduced VA in Chinese students increased from 28.6 to 56.8% from 1985 to 2010 in mainland China [13]. Similar trends were observed in Taiwan and Singapore [8].
The prevalence of reduced VA in the 6–7-year olds in 2002 was higher than that in 2018 and there was a decreasing trend from age 6 to 10 in 2002. However, as can be seen from Fig. 2, the prevalence of moderately and severely reduced VA in the 6–7-year olds in 2018 has risen compared to 2002. This suggests that the overall vision among the 6–7-year olds has not really improved in 2018. The decreasing trend from age 6 to 10 in 2002 was mainly caused by the decrease in mildly reduced VA. It should be noted that the high prevalence of reduced VA in the 6–8-year olds may not be due to myopia. Studies that measure cycloplegic refraction show that the actual prevalence of myopia in the 6–8-year olds is much lower than our results [14]. Although unaided VA has been used as a justified measure of myopia in previous studies [11, 12, 15], cognitive difficulties may be present when vision tests are administered at a younger age. Therefore, we speculated that the higher prevalence of reduced VA in young children in 2002 and 2018 was caused by cognitive difficulties. The comparatively lower prevalence of reduced VA in the 6–7-year olds in 2018 was caused by cognitive improvement. Due to more intensive teaching in kindergartens, these children may be better prepared cognitively for schooling than in the past. Compared to 2002, our results indicated that the prevalence of severely reduced VA increased significantly across almost all age groups of children in Changsha in 2018, suggesting that there was no meaningful vision improvement in 2018.
Xiang et al. found that the prevalence of moderately and severely reduced VA was closely correlated with the prevalence of myopia measured by cycloplegic autorefraction [11]. Although cycloplegic refraction (the gold standard for myopia assessment) was not measured due to the large sample size, the observed trend of the increase in moderately and severely reduced VA was largely due to the increased prevalence of myopia. When comparing our results with previous studies using the same methodology, we found that the distribution of moderately and severely reduced VA across ages in Changsha in 2018 was similar to that pattern in Guangzhou in 2002. The prevalence of moderately and severely reduced VA in the 6–9-year olds in Changsha in 2002 was around 10%, while the prevalence in Guangzhou was 15–30%, similar to that in Changsha in 2018. The prevalence of moderately and severely reduced VA at age 15 in Changsha in 2002 was 30%, compared to about 75% in Guangzhou in 2002 and 60% in Changsha in 2018. Urbanisation and socioeconomic development are highly associated with increased myopia in China [12]. As economic development, urbanisation, and the expansion of the education system have occurred almost in parallel in China, the increasing intensity of education seems to be the most important factor that could have contributed to the increased myopia. Since Guangzhou is one of the biggest tier 1 cities in China, and Changsha is a rapidly developing new tier 1 city which has just been ranked as a new tier 1 city, the similar growth pattern between Changsha in 2018 and Guangzhou in 2002 suggests a continuing growth of myopia in Changsha in forthcoming years. Therefore, the government and health organisations should prepare for the urgent need for interventions.
We observed that girls had a higher prevalence of reduced VA and severely reduced VA than boys, which was consistent with findings from other studies [16,17,18]. In traditional Chinese culture, girls are expected to be quiet. They spend more time indoors doing near work while boys spend more time outdoors which may prevent the development of myopia [19]. The results also showed that the age-specific prevalence of severely reduced VA had an obvious trend that increased with age, which was in agreement with previous research results [20, 21]. Although the cumulative prevalence of severely reduced VA is expected to increase with age as myopia progresses, we speculated that the increased study intensity also contributed to the increased prevalence. As in China, the intensity of studying increases with age, and older children have to spend more time doing homework every day and less time playing outdoors. Studies have shown that the intensity of studying is the main environmental and behavioural factor of myopia [18].
To our knowledge, this is the first study focussing on the vision of elementary and secondary school students in central China. However, there were some limitations to this study. First, because of the large sample size, we did not perform any form of refraction. We used unaided VA as an alternative measure of myopia. Although this method is useful for monitoring changes in the prevalence of myopia, it has some limitations. For one, it is not appropriate for children from the ages of 3 up to around 8–9 years due to cognitive difficulties in distinguishing directions. For another, testing an eye properly requires a child to have each eye tested separately and not “cheat” by peeking through the closed eye or try to remember the order of the letters from the first eye tested. Alternative tests that minimise cognitive challenges, such as HOTV tests [22], need to be promoted. Second, rather than using a national representative sample, we used a sample from an urban district in China; therefore, our results may not reflect the trends of reduced VA in rural China. In addition, the prevalence rate in Yuhua District could be different from the national prevalence rate in China, because there are regional differences. However, the main purpose of our study was to investigate trends in the prevalence, and our findings should be able to reflect the trends in urban China.
Conclusion
The prevalence of reduced VA among children aged 6–15 years in Yuhua District has become more common with age, and there has been a marked increase in the prevalence of reduced VA from 2002 to 2018. The remarkable epidemic of reduced VA started 5 years earlier in 2018 than in 2002. Evidence from the present study suggests that interventions should be launched before the age of 9 years.
Summary
What was known before
-
China, with its rapid economic development and transitions in behaviour and lifestyle, is one of the countries with the highest rates of childhood myopia in the world.
-
The Chinese government now pays more attention than ever before to the eyesight health of children and adolescents.
What this study adds
-
The purpose of this study was to investigate trends in the prevalence of reduced visual acuity (VA), a proxy measure for myopia, in an urban district in China.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
References
Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86:63–70. https://doi.org/10.2471/blt.07.041210.
Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt. 2005;25:381–91. https://doi.org/10.1111/j.1475-1313.2005.00298.x.
Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379:1739–48. https://doi.org/10.1016/S0140-6736(12)60272-4.
Wu LJ, Wang YX, You QS, Duan JL, Luo YX, Liu LJ, et al. Risk factors of myopic shift among primary school children in Beijing, China: a prospective study. Int J Med Sci. 2015;12:633–8. https://doi.org/10.7150/ijms.12133.
Saw SM, Chan YH, Wong WL, Shankar A, Sandar M, Aung T, et al. Prevalence and risk factors for refractive errors in the Singapore Malay Eye Survey. Ophthalmology. 2008;115:1713–9. https://doi.org/10.1016/j.ophtha.2008.03.016.
Rose KA, Morgan IG, Smith W, Burlutsky G, Mitchell P, Saw SM. Myopia, lifestyle, and schooling in students of Chinese ethnicity in Singapore and Sydney. Arch Ophthalmol. 2008;126:527–30. https://doi.org/10.1001/archopht.126.4.527.
Bourne RRA, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e888–97. https://doi.org/10.1016/S2214-109X(17)30293-0.
Morgan IG, French AN, Ashby RS, Guo X, Ding X, He M, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2018;62:134–49. https://doi.org/10.1016/j.preteyeres.2017.09.004.
He M, Abdou A, Naidoo KS, Sapkota YD, Thulasiraj RD, Varma R, et al. Prevalence and correction of near vision impairment at seven sites in China, India, Nepal, Niger, South Africa, and the United States. Am J Ophthalmol. 2012;154:107–16. https://doi.org/10.1016/j.ajo.2012.01.026.
Dolgin E. The myopia boom. Nature. 2015;519:276–8. https://doi.org/10.1038/519276a.
Xiang F, He M, Zeng Y, Mai J, Rose KA, Morgan IG. Increases in the prevalence of reduced visual acuity and myopia in Chinese children in Guangzhou over the past 20 years. Eye (Lond). 2013;27:1353–8. https://doi.org/10.1038/eye.2013.194.
Jan C, Xu R, Luo D, Xiong X, Song Y, Ma J, et al. Association of visual impairment with economic development among Chinese school children. JAMA Pediatr. 2019;173:e190914. https://doi.org/10.1001/jamapediatrics.2019.0914.
Sun H, Li A, Xu Y, Pan C. Secular trends of reduced visual acuity from 1985 to 2010 and disease burden projection for 2020 and 2030 among primary and secondary school students in China. JAMA Ophthalmol. 2015;133:262–8. https://doi.org/10.1001/jamaophthalmol.2014.4899.
He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern china. Invest Ophthalmol Vis Sci. 2004;45:793–9. https://doi.org/10.1167/iovs.03-1051.
Leone JF, Mitchell P, Morgan IG, Kifley A, Rose KA. Use of visual acuity to screen for significant refractive errors in adolescents: is it reliable? Arch Ophthalmol. 2010;128:894–9. https://doi.org/10.1001/archophthalmol.2010.134.
Lyu Y, Zhang H, Gong Y, et al. Prevalence of and factors associated with myopia in primary school students in the Chaoyang District of Beijing, China[J]. Jpn J Ophthalmol. 2015;59:421–9. https://doi.org/10.1007/s10384-015-0409-x.
Li Y, Liu J, Qi P. The increasing prevalence of myopia in junior high school students in the Haidian District of Beijing, China: a 10-year population-based survey[J]. BMC Ophthalmol. 2017;17:88. https://doi.org/10.1186/s12886-017-0483-6.
You QS, Wu LJ, Duan JL, Luo YX, Liu LJ, Li X, et al. Factors associated with myopia in school children in China: the Beijing childhood eye study. PLoS ONE. 2012;7:e52668. https://doi.org/10.1371/journal.pone.0052668.
He M, Xiang F, Zeng Y, Mai J, Chen Q, Zhang J, et al. Effect of time spent outdoors at school on the development of myopia among children in China. JAMA. 2015;314:1142–8. https://doi.org/10.1001/jama.2015.10803.
Guo Y, Duan JL, Liu LJ, Sun Y, Tang P, Lv YY, et al. High myopia in greater Beijing school children in 2016. PLoS ONE. 2017;12:e187396. https://doi.org/10.1371/journal.pone.0187396.
Hashim SE, Tan HK, Wan-Hazabbah WH, Ibrahim M. Prevalence of refractive error in malay primary school children in suburban area of Kota Bharu, Kelantan, Malaysia. Ann Acad Med Singap. 2008;37:940–6.
Thomas J, Rajashekar B, Kamath A, Gogate P. Diagnostic accuracy and agreement between visual acuity charts for detecting significant refractive errors in preschoolers. Clin Exp Optom. 2020;103:347–52. https://doi.org/10.1111/cxo.12962.
Acknowledgements
The authors thank the subjects in the study and appreciate all of the support of the data collectors. We are also like to thank Editage for English language editing.
Author information
Authors and Affiliations
Contributions
STX and SZ contributed equally to designing this article, performing the statistical analyses, and drafting the manuscript. XL provided critical revision of the manuscript. YZ and LPL participated in the design of the study. LHX and RTK helped completed the acquisition of data. All authors read and gave final approval of the version to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Consent to publish
All authors approved the final manuscript for submission and gave consent for publication.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Hunan Children’s Hospital. Informed written consent was obtained from a legal guardian of each child involved in our study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xiang, S., Zhao, S., Li, X. et al. The prevalence of reduced visual acuity in children from an urban district in China from 2002 to 2018. Eye 35, 2550–2555 (2021). https://doi.org/10.1038/s41433-020-01269-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-020-01269-0
This article is cited by
-
Trajectories of spherical equivalent refraction from grades 1 to 4 in Chinese children
BMC Public Health (2023)
