
Abstract
Background
To evaluate the spontaneous change in size over the time of idiopathic full-thickness macular holes (IFTMHs) using optical coherence tomography (OCT).
Methods
This retrospective observational study included 24 eyes of 24 consecutive patients waiting for IFTMH surgery. On OCT horizontal B-scan passing through the center of the fovea, the minimum linear diameter (MLD), the basal diameter (BD), and the presence of vitreomacular adhesion (VMA) were evaluated. The mean total and daily MLD and BD variations were calculated as both absolute and percentage values.
Results
The MLD and BD size increase was statistically significant (P < 0.0001). The MLD size increase was significantly greater for small (<250 μm) versus both medium (≥250 to ≤400 μm) and large (>400 μm) IFTMHs in all analysis: the total absolute (P = 0.0248), the daily absolute (P = 0.0186), the total percentage (P = 0.0020), and the daily percentage (P = 0.0008) variations. For the BD, the significance between the same groups was achieved only in the daily percentage change (P = 0.0220). The presence of VMA did not influence the amount of MLD and BD increase. The rate of increase was dependent on the size of hole at presentation (MLD: small: 1.67 microns per day; medium: 0.61 microns per day; large: 0.44 microns per day).
Conclusions
Both MLD and BD increase over the time in IFTMHs. There is a significantly greater rate of increase in hole size in smaller holes compared with larger. Therefore, prioritisation for small IFTMH may be justified.
Similar content being viewed by others


Introduction
Idiopathic full-thickness macular hole (IFTMH) has an incidence of between 7.4 and 7.9 per 100,000 individuals per year. With a predominance for women between the sixth and seventh decade of life, it commonly causes metamorphopsia and central vision loss [1, 2].
Previous studies have observed a progressive enlargement of IFTMHs over time, whereas spontaneous resolution is a rare event [3,4,5,6,7,8,9]. It is believed that the increase in size is due to both the hydration of the hole edges and cysts formation, and the secondary traction by the glial cell proliferation on the internal limiting membrane (ILM) surface [10, 11].
Spectral domain optical coherence tomography (SD-OCT) has been recognised as a valuable tool for assessing the IFTMH [12,13,14,15,16]. Its use has become increasingly important to predict both anatomical and functional outcomes and to aid preoperative surgical planning.
The aim of this article is to analyse the change in size over the time of IFTMHs using the SD-OCT imaging. In particular, we studied the mean variation of both the minimum linear diameter (MLD) and the basal diameter (BD) in pursuit of an average value of progression useful in predicting hole size at a specific time point. Prior studies have assessed the change in IFTMH size but, to the best of our knowledge, this is the first work that provides a daily mean value of this change [3,4,5,6,7,8].
Materials and methods
This retrospective observational study included 24 eyes of 24 consecutive patients with a diagnosis of IFTMH recruited between July 2015 and August 2017 at the Ophthalmology Department of St Thomas’ Hospital, London, UK. The study was conducted in accordance with the tenets of the Declaration of Helsinki and it was approved by the St Thomas Hospital Research and Ethics Committee.
The diagnosis of IFTMH was based on the optical coherence tomography (OCT) imaging and each studied eye was scanned at least twice before surgery. The number of days between the baseline and the follow-up examinations was also recorded.
The exclusion criteria were the following: non-idiopathic aetiology of the hole (i.e. traumatic or myopic), any corneal or lenticular opacity affecting the quality of OCT images, myopia ≥ 6D, previous history of glaucoma or ocular hypertension, previous ocular trauma, previous vitrectomy or retinal laser treatment, macular and retinal pathology of any cause (such as age-related macular degeneration, uveitis, retinal vascular diseases).
For each patient, the following data were collected from the case notes at both examinations: gender, age, laterality, lens status, and best-corrected visual acuity (BCVA) of the involved eye. BCVA was collected from Snellen acuity chart values and converted to logarithm of the minimal angle of resolution (LogMAR) scores for the purposes of statistical analysis. All OCT scans were acquired with Heidelberg Spectralis SD-OCT (Heidelberg Engineering, Heidelberg, Germany), software version 1.10.0.0. The standard imaging protocol used consisted of a volume scan of the macula covering a 6.0 mm × 6.0 mm area. This scan was composed of 25 horizontal B-scans acquired in an automated real-time (ART) mode for averaging 16 frames to improve image quality. The image alignment eye-tracking software (TruTrack; Heidelberg Engineering Inc.) and the AutoRescan function were used to optimize scan concordance.
Manual measurements were performed independently on OCT images by two blinded expert investigators (J.R. and M.B.) using Spectralis SD-OCT software callipers, and the mean value was used for analysis. The B-scan passing through the fovea was chosen as reference image for measurements. The MLD and the BD were evaluated. The MLD was defined as the narrowest point in the mid retina parallel to the retinal pigment epithelium (RPE), while the BD as the basal aperture of the hole, just above the RPE, as previously described (Figs. 1, 2 and 3) [17]. Furthermore, the presence of vitreomacular adhesion (VMA), defined as a vitreous attachment on the hole edges, was also recorded. Holes were subsequently divided in three groups considering the baseline MLD and following the International Vitreomacular Traction Study (IVTS) Group criteria which define small (<250 μm), medium (≥250 to ≤400 μm) and large (>400 μm) full-thickness macular hole (FTMH) [18]. The mean MLD and BD values, in μm, were calculated for all eyes and for each size group. The mean total and daily MLD and BD variations, expressed as both absolute (μm) and percentage (%) values were calculated for all eyes and for each size group. Comparisons between the groups were also made.

MLD and BD increase measurement of a small IFTMH by using the horizontal OCT B-scan passing through the fovea. a Baseline: the MLD was 115 μm and the BD was 464 μm. b Follow-up after 139 days: the MLD was 371 μm and the BD was 958 μm. Thus, while at baseline the IFTMH was classified as small, at the follow-up visit it was classified as medium

MLD and BD increase measurement of a medium IFTMH by using the horizontal OCT B-scan passing through the fovea. a Baseline: the MLD was 296 μm and the BD was 670 μm. b Follow-up after 112 days: the MLD was 376 μm and the BD was 893 μm. In both observations this IFTMH was classified as medium

MLD and BD increase measurement of a large IFTMH by using the horizontal OCT B-scan passing through the fovea. a Baseline: the MLD was 542 μm and the BD was 1551 μm. b Follow-up after 105 days: the MLD was 676 μm and the BD was 1556 μm. In both observations this IFTMH was classified as large
Categorical variables were reported as count and percentage in each category, quantitative variables as mean, standard deviation, and range (minimum and maximum). Inter-observer agreement was assessed by the Lin’s concordance correlation coefficient (CCC) along with the 95% confidence interval calculated with the bias-corrected and accelerated bootstrap method considering 2000 resamplings (95% CI). Comparison of categorical variables between baseline and follow-up was performed with McNemar’s test. The absolute, percentage, and daily percentage change between baseline and follow-up of quantitative variables was analysed with the Wilcoxon signed rank test, and the comparison of the groups determined by the hole dimension at baseline was conducted with the Kruskal–Wallis test followed by the Dwass, Steel, Critchlow–Fligner method for multiple comparison in case of statistical significance. No other adjustment for multiple comparison was done. A bilateral p value < 0.05 was considered as indicative of statistical significance. The analysis was conducted with SAS 9.4 (AS Institute Inc., Cary, NC, USA) for Windows.
Results
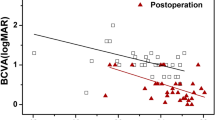
Twenty-four (13 right and 11 left) eyes of 24 consecutive patients with diagnosis of IFTMH were enroled in this study. There were 16 (66.7%) females and the mean age was of 70.63 ± 5.35 (range, 60–80) years. The mean period of time between the baseline and the follow-up examinations was 114.63 ± 31.85 (range, 69–170) days. The mean BCVA was 0.80 ± 0.13 (range, 0.5–1) LogMAR at baseline and 0.83 ± 0.14 (range, 0.5–1) LogMAR at follow-up examinations. The visual acuity decreased in seven (29.17%) patients over this period, with a statistical significant difference (P = 0.016) between the baseline and the follow-up examinations. Four (16.7%) eyes were pseudopakic and 20 (83.3%) were phakic preoperatively.
Regarding MLD and BD measurements, a high degree of agreement was found. The CCC at the baseline evaluation was 0.991 (95% CI: 0.983, 0.996) for the MLD and 0.995 (95% CI: 0.9888, 0.999) for the BD; at the follow-up evaluation, CC = 0.990 (95% CI: 0.979, 0.996) for the MLD, and CCC = 0.975 (95% CI: 0.909, 0.995) for the BD.
At baseline, 12 (50.0%) were classified as small, 7 (29.2%) as medium, and 5 (20.8%) as large IFTMHs, whereas at the follow-up visit 4 (16.7%) were classified as small, 9 (37.5%) as medium, and 11 (45.8%) as large IFTMHs, with a statistical significant difference (P = 0.019) between the two observations (Figs. 1, 2, and 3).
The mean MLD and BD values for the totality of IFTMHs and for each size group and their daily and total increase between the two examinations, expressed as both absolute and percentage values, are shown in Table 1.
With regard to the mean MLD and BD values, all factors were statistically significant different between the three IFTMHs size subgroups except for the BD at the follow-up examination (Table 1).
The MLD and BD for the entire group was statistically significant for both the absolute and the percentage variations (P < 0.0001). By contrast, comparing the increase between each IFTMHs size group values, the change was significantly larger for the MLD of small IFTMHs than that of both medium and large IFTMHs, whereas for the BD the significance was achieved only in the daily percentage change (Table 1).
Considering the presence of VMA, this was recognisable in eight (33.3%) patients. The presence of VMA did not influence the amount of MLD and BD increase over the whole period (P = 0.520 and P = 0.976, respectively) and the daily change (P = 0.520 and P = 0.783, respectively).
Discussion
IFTMHs are defined as an anatomic defect of the fovea characterised by the interruption of all neural retinal layers from the ILM to the RPE due to vitreomacular traction [18]. Until Kelly and Wendel first reported in 1991 that vitrectomy was successful in the closure of macular holes, IFTMH had long been regarded as an incurable disease [19, 20]. Since then, different surgical techniques have been developed to treat this pathology, including intravitreal injection of ocriplasmin [17, 21]. As SD-OCT allows to obtain detailed images of the anatomy of the macula, it has become an increasingly useful tool to help clinicians in choosing the best surgical option for IFTMHs and to predict the postsurgical outcome.
In literature, many different methods of measuring FTMHs on OCT scans have been described, including macular hole inner opening, MLD, BD, hole form factor, macular hole index, diameter hole index, and tractional hole index [12,13,14, 16]. However, Wakely et al. demonstrated that there is no real advantage to be gained by calculating derived indices from the basic ophthalmic measurements, as they were originally proposed to reflect changes in macular morphology and tractional forces, thought to be acting upon the macula during the hole formation [16]. They stated that macular hole inner opening is probably the hardest variable to measure reliably and consistently. MLD exhibited the lowest level of model discrimination with respect to the key outcome measure of anatomical success and preoperative BD was easy to measure and strongly associated with anatomical and visual outcomes: they could then be used as fairly effective predictors of postoperative outcomes [16]. For this reason, we decided to consider only MLD and BD as useful parameters to evaluate IFTMHs changes.
In our study, we analysed the natural evolution of a series of IFTMHs using the SD-OCT images by examining the average, total, and daily change of both MLD and BD parameters over a period of time. As it is well known that surgery is variably postponed from the diagnosis of IFTMH, we believe that this information could be useful for clinicians in prioritising their chosen technique at the moment of the surgical procedure and to predict both the anatomical success and the postoperative visual outcome. Indeed, it has been reported that the preoperative macular hole size may determine the chosen surgical technique and that a smaller preoperative macular hole attains a higher rate of closure rate and a better prognosis for visual rehabilitation [12,13,14,15,16,17, 22, 23].
In our study, we observed a significant MLD and BD increase in all patients. The rate of increase was dependent on the size of hole at presentation (MLD: small: 1.67 microns per day; medium: 0.61 microns per day; large: 0.44 microns per day). There was statistical significance for both the absolute variation value and the percentage change. No spontaneous resolution of the holes were observed among our patients. The literature reports a closure rate of between 2.7 and 8.6% [6, 9]. Two different mechanisms have been proposed to explain the progressive enlargement of a full-thickness macular hole. The hydration theory hypothesizes that the hydration of the hole edges with cysts formation could be one of the forces triggering the enlargement [10]. A second theory suggests that glial cells may proliferate onto the ILM surface creating a secondary traction, leading to the enlargement and preventing the healing of the hole by releasing only the vitreous traction [11].
Previous works have found an enlargement of IFTMHs in a percentage of patients ranging from 33.6 to 85% over a period of 1–6 years [3, 5,6,7]. However, these observations were made using fundus photograph and fluorescein angiogram images rather than the more precise measurement using the SD-OCT [3, 5,6,7].
To the best of our knowledge, the only work which analysed the change in size of IFTMHs over the time by using SD-OCT was that of Madi et al. [8] They observed that over an average period of 8 weeks, 64% of patients had an increase of MLD, with a mean of 74 μm [8]. By contrast, we evaluated both the MLD and the BD. Ruiz-Moreno demonstrated that both of these were inversely correlated with the postoperative BCVA. Haritoglou and Kim found that a larger BD was associated with a poorer final BCVA, whereas neither found any significant correlation with MLD [15, 24, 25]. The MLD increase in just 64% of patients in the work of Madi could be explained by the shorter follow-up period compared with our data [8].
In our study, the same measurements were performed by two independent investigators and, as MLD and BD can be measured manually, this improved the reliability of the data. The measurements of the two examiners did not result in a statistically significant difference (CCC between 0.98 and 0.99) and a mean value was used to reduce the subjective error. By contrast, measuring IFTMH size variation over the time using values given by a single examiner may pose an increased possibility of a subjective error [2, 5,6,7,8].
We used the new IVTS classification system introduced by the IVTS Group to evaluate if the baseline MLD influenced the amount of the increase of both MLD and BD [18, 26]. Our data demonstrated that the increase of MLD of small IFTMH was greater than that of medium and large IFTMH. This observation is consistent with the findings of Madi et al. who highlighted that smaller holes had a greater likelihood of enlarging [9].
In regards to vitreomacular interface, we did not observe any vitreous separation over the follow-up period among patients who presented with VMA. This is in contrast with previous works, in which the percentage of patients with a complete vitreomacular detachment increased [3, 6, 8]. This could be due to both the length of follow-up and the number of patients in our work. We also found that the amount of IFTMHs enlargement was independent of the presence of VMA. This observation is in agreement with the findings of Philippakis et al. who did not find a relation between the progression of VMA and the enlargement of IFTMHs [27]. On the contrary, Hikichi and Madi found that that VMA was associated with a higher rate of progression [3, 8]. More studies are needed to clarify the impact of VMA in determining IFTMHs enlargement.
In conclusion, our work provides two useful parameters in choosing the best surgery for patients affected by an IFTMH who have to undergo surgery after a determinate time lapse from the initial assessment. This could be even more useful when a SD-OCT examination at the date of surgery is not available. This information could be helpful for clinicians to provide patients with accurate information about the rates of anatomical and functional success after surgery. However, the limitations of these parameters as predictors, the retrospective nature of the study, the limited number of subjects, and the short follow-up period must be taken into consideration. Therefore, a larger and longer prospective study on MLD and BD change over the time might be useful to strengthen our findings.
Summary
What was known before
IFTMHs usually enlarge over the time.
SD-OCT is a valuable tool to assess the characteristics of IFTMHs.
Many parameters on SD-OCT have been used to describe IFTMHs, including the MLD and the BD.
What this study adds
The MLD and the BD can be used to forecast the enlargement of IFTMHs over a certain period of time.
The best surgery for a IFTMH can be chosen knowing the initial MLD and BD and how much time elapsed from their assessment.
References
McCannel CA, Ensminger JL, Diehl NN, Hodge DN. Population-based incidence of macular holes. Ophthalmol. 2009;116:1366–9.
Forsaa VA, Lindtjørn B, Kvaløy JT, Frøystein T, Krohn J. Epidemiology and morphology of full-thickness macular holes. Acta Ophthalmol. 2018;96:397–404.
Hikichi T, Yoshida A, Akiba J, Konno S, Trempe CL. Prognosis of stage 2 macular holes. Am J Ophthalmol. 1995;119:571–5.
Hikichi T, Yoshida A, Akiba J, Trempe CL. Natural outcomes of stage 1, 2, 3, and 4 idiopathic macular holes. Br J Ophthalmol. 1995;79:517–20.
Kim JW, Freeman WR, El-Haig W, Maguire AM, Arevalo JF, Azen SP.Baseline characteristics, natural history, and risk factors to progression in eyes with stage 2 macular holes. Results from a prospective randomized clinical trial. Ophthalmol. 1995;102:1818–29.
Chew EY, Sperduto RD, Hiller R, Nowroozi L, Seigel D, Yanuzzi LA, et al. Clinical course of macular holes: the eye disease case-control study. Arch Ophthalmol. 1999;117:242–6.
Casuso LA, Scott IU, Flynn HW, Gass DM, Smiddy WE, Lewis ML, et al. Longterm follow-up of unoperated macular holes. Ophthalmol. 2001;108:1150–5.
Madi HA, Dinah C, Rees J, Steel DH. The case mix of patients presenting with full-thickness macular holes and progression before surgery: implications for optimum management. Ophthalmol. 2015;233:216–21.
Sugiyama A. Reappraisal of spontaneous clousure rate of idiopathic full-thickness macular holes. Open Ophthalmol J. 2012;6:73–74.
Tornambe PE. Macular hole genesis: the hydration theory. Retina. 2003;23:421–4.
Schubert HD, Kuang K, Kang F, Head MW, Fischbarg J. Macular holes: migratory gaps and vitreous as obstacles to glial closure. Graefes Arch Clin Exp Ophthalmol. 1997;235:523–9.
Ip MS, Baker BJ, Duker JS, Reichel E, Baumal CR, Gangnon R, et al. Anatomical outcomes of surgery for idiopathic macular hole as determined by optical coherence tomography. Arch Ophthalmol. 2002;120:29–35.
Ullrich S, Haritoglou C, Gass C, Schaumberger M, Ulbig MW, Kampik A. Macular hole size as a prognostic factor in macular hole surgery. Br J Ophthalmol. 2002;86:390–3.
Kusuhara S, Teraoka Escano MF, Fujii S, Nakanishi Y, Tamura Y, Nagai A, et al. Prediction of postoperative visual outcome based on hole configuration by optical coherence tomography in eyes with idiopathic macular holes. Am J Ophthalmol. 2004;138:709–16.
Ruiz-Moreno JM, Arias L, Araiz J, García-Arumí J, Montero JA, Pinero DP. Spectral-domain optical coherence tomography study of macular structure as prognostic and determining factor for macular hole surgery outcome. Retina. 2013;33:1117–22.
Wakely L, Rahman R, Stephenson J. A comparison of several methods of macular hole measurement using optical coherence tomography, and their value in predicting anatomical and visual outcome. Br J Ophthalmol. 2012;96:1003–7.
Madi HA, Masri I, Steel DH. Optimal management of idiopathic macular holes. Clin Ophthalmol. 2016;10:97–116.
Duker JS, Kaiser PK, Binder S, de Smet MD, Gaudric A, Reichel E, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmol. 2013;120:2611–9.
Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol. 1991;109:654–9.
Wendel RT, Patel AC, Kelly NE, Salzano TC, Wells JW, Novack GD. Vitreous surgery for macular holes. Ophthalmol. 1993;100:1671–6.
OH H. Idiopathic macular hole. Dev Ophthalmol. 2014;54:150–8.
Cheng L, Azen SP, El-Bradey MH, Toyoguchi M, Chaidhawangul S, Rivero ME, et al. Effects of preoperative and postoperative epiretinal membranes on macula hole closure and visual restoration. Ophthalmol. 2002;109:1514–20.
Gupta B, Laidlaw DA, Williamson TH, Shah SP, Wong R, Wren S. Predicting visual success in macular hole surgery. Br J Ophthalmol. 2009;93:1488–91.
Haritoglou C, Neubauer AS, Reiniger IW, Priglinger SG, Gass CA, Kampik A. Longterm functional outcome of macular hole surgery correlated to optical coherence tomography measurements. Clin Exp Ophthalmol. 2007;35:208–13.
Kim SH, Kim HK, Yang JY, Lee SC, Kim SS. Visual recovery after macular hole surgery and related prognostic factors. Korean J Ophthalmol. 2018;32:140–6.
Gass JD. Idiopathic senile macular hole. Its early stages and pathogenesis. Arch Ophthalmol. 1988;106:629–39.
Philippakis E, Amouval F, Couturier A, Boulanger-Scemama E, Gaudric A, Tadayoni R. Size and vitreomacular attachment of primary full-thickness macular holes. Br J Ophthalmol. 2017;101:951–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Berton, M., Robins, J., Frigo, A.C. et al. Rate of progression of idiopathic full-thickness macular holes before surgery. Eye 34, 1386–1391 (2020). https://doi.org/10.1038/s41433-019-0654-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-019-0654-1
This article is cited by
-
Makulaforamen und vitreomakuläre Traktion
Die Ophthalmologie (2023)
-
Optical coherence tomography features and risk of macular hole formation in the fellow eye
BMC Ophthalmology (2021)
