
Abstract
Research protocol
The protocol was developed as per the recommendations of the Cochrane-handbook and PRISMA and was registered in PROSPERO.
Literature search
Search was performed by using MeSH-Terms and keywords in PubMed, Scopus, Embase, Web of Sciences, Lilacs, and Cochrane databases and gray literature sources 15th July 2022. There were no limits regarding the year of publication and language. Hand-searching of included articles was also performed. Titles and abstracts and later full texts were screened as per strict inclusion and exclusion criteria.
Data extraction
Self-designed pilot-tested form was used.
Quality appraisal
Risk of bias was analyzed through Joanna-Brigg’s-Institute’s-critical appraisal checklist. The evidence analysis was done by using the GRADE approach.
Data analysis
Qualitative synthesis was performed for describing the study characteristics, details of sampling, and results of various questionnaires. It was discussed by the expert group and presented using KAP heat map. Meta-analysis was done by using Random Effects Model.
Results and interpretation
The risk of bias was found to be low in seven and moderate in one study. It was observed that >50% of parents knew about the urgency to seek professional advice after TDI. Only <50% of parents were confident of their ability to identify the injured tooth, clean the soiled avulsed tooth, and perform the replantation. Appropriate responses regarding immediate action after tooth avulsion were given by 54.5% (95% CI: 50.2–58.8, p = 0.042) of parents. The knowledge of the parents regarding the emergency management of TDI was found to be inadequate. The majority of them were interested in obtaining information about dental trauma first aid.
Similar content being viewed by others
Background
Traumatic dental injuries (TDI) have been regarded as one of the most prevalent noncommunicable diseases1. They have a higher predilection for two age groups which have also been termed peaks of incidence. The first peak occurs at 2–3/4 years of age and is common for both males and females. The second peak, more common in males, occurs at 9–10 years of age2. Petti et al. used the global population and the burden of diseases data of 2016 to extrapolate that about 180 million children must have suffered from an injury to primary teeth and about one billion in permanent dentition1. The prevalence of TDI in primary teeth has been reported as 22.7% (95 CI: 17.3–28.7%) and that of permanent teeth was reported as 15.2% (95 CI: 13.0–17.4%)1. This highlights that most of the individuals get injured before the age of 18 years when they are living with their parents or dependent upon them3. Several authors have also highlighted that home is one of the commonest sites where children get injured2,3.
International Association of Dental Traumatology (IADT) guidelines emphasized that the immediate management of most TDI is essential for long-term good survival of the traumatized tooth/teeth4,5,6,7. This becomes more prudent in the severe form of TDI such as tooth avulsion, and intrusive, extrusive, lateral luxations4,5,6,7. Andreasen et al. established that the survival of the tooth and its vital structures such as periodontal ligament (PDL) and pulp is dependent upon effective emergency management8,9,10. Since trauma can occur at any place, this treatment often has to be rendered by the people present in the vicinity of the injured child11. The stakeholders involved in such trauma scenarios are generally school teachers, sports coaches, and parents11. The better understanding of dental trauma first aid can play an important role in empowering these stakeholders for confident handling of TDI to children12. Education of the parents is even more important because they are the primary care providers and decision makers for the child’s well-being and must be able to take proactive steps for safeguarding their children from the adverse consequences of untreated/ improperly treated injuries13. The fracture of teeth, their discoloration and improper position, etc can psychologically affect the child. This can be easily prevented through onsite dental trauma first aid4,5,6,7.
Tewari et al. established that the knowledge of school teachers regarding the prevention and emergency management of TDI was inadequate, globally11. There are several studies that have evaluated the awareness levels of parents, especially mothers13,14,15,16,17,18,19,20 but the overall global scenario is yet to be deciphered. Hence, this systematic review (SR) aimed to evaluate the global status of the knowledge of the parents regarding the emergency management of TDI, and to provide the recommendations for future research.
Methods
Protocol and registration
The SR was performed according to the Cochrane handbook and reported as per the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)21,22,23. An a priori protocol was prepared after an expert group discussion, and registered in PROSPERO (CRD42021293430).
Eligibility criteria for study selection
Inclusion criteria
-
Studies related to the PICO of the research question (Table 1).
Table 1 Details of the Population (P), Intervention (I), Comparator (C), Outcome (O) elements of the research question, the search strategy, and inclusion & exclusion criteria. -
All descriptive, observational, Cohort studies, Cross-Sectional, Case-control studies, and Randomized/ Non-Randomized trials.
Exclusion criteria
-
The case reports, case series, letter to the editor, comprehensive and systematic reviews.
-
Studies with inadequate information regarding the questionnaire, the methods used for development and validation.
Information sources
The search was conducted independently by two reviewers (NT and SG) in PUBMED, Scopus, LILACS, Cochrane, Embase and Web of Science by on 15th July 2022 (Table 1). The gray literature was searched through Google Scholar and open Gray by the same reviewers. The reference search of the included articles was done manually for exploring all the available records related to the research question.
Search
The search strategy was defined as per the Population (P), Intervention (I), Comparator (C), and Outcome (O) elements of the research question and included MeSH terms, keywords, and use of Boolean operators ‘AND’ and ‘OR’ in different combinations. This was done without any limitation of language and time.
Screening and selection of studies
The searches were saved electronically in the EndNote reference management software (EndNote-TMX9 Clarivate Analysis, USA) and duplicates were removed by using the same. The details of search strategy and inclusion/exclusion criteria have been summarized in Table 1 and the search strategy results for different search engines in the online Supplementary Information. Scrutiny of the titles and abstract was independently performed by NT and SG with a high level of agreement as reflected by Cohen’s Kappa value of 0.92. Full texts of the selected articles were downloaded and subjected to scrutiny by NT and SG. This step showed high level of agreement (Cohen’s Kappa value of 0.95). In any event of disagreement in any of these steps, the senior reviewer (VM) was consulted for consensus.
Data extraction
Expert group discussion was held to formulate a data extraction sheet and it was pre-tested in a sample of 5 studies. Two reviewers SG and SS performed the data extraction independently to record the information related to study demographics, study design (type, duration, sampling strategies), details of the questionnaire (source, language, questions, validity, and reliability of questionnaire and mode of administration), details of the results and conclusion. A strategy to contact the authors for obtaining more details had also been formulated but it was not required in the present review.
Study quality assessment
The risk of bias in the included studies was assessed by two reviewers (SG and SS) by using Joanna Brigg’s Institute (JBI) critical appraisal checklist for analytical cross-sectional studies. The agreement of reviewers for data extraction and ROB analysis was also found to be good with Cohen’s Kappa values ranging from 0.85–0.97. Any disagreement was resolved by consulting the senior reviewer (VM).
Qualitative synthesis
The details of questions from the studies were used to develop a “KAP-HEAT Map”, on the basis of the number of studies which included a question11,12,24,25,26. This visual map included the questions which were common to 3 or more studies (1/3 of the included studies). The map was coded into five different colors which represented the level of awareness among parents related to a question (dark blue-not included, white-< 25%, light yellow- 25–50%, dark yellow- 51–75%, and red- >75%11,12,24,25,26.
Meta-analysis and evidence grading
KAP heat map also helped in deriving data for meta-analysis. The level of awareness of the questions common to five or more studies and with homogeneity in the outcome assessment and interpretation were analyzed by using the random effects model. The analysis was performed by Comprehensive Meta-analysis Software (New Jersey, USA) by NT. Same software was used for assessing the publication bias by using Funnel plot and Egger’s test. The strength of evidence regarding the outcomes of meta-analyses was assessed on the basis of the recommendations of GRADE for non-randomized studies.
Results
Search results
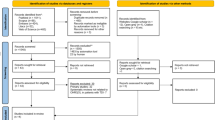
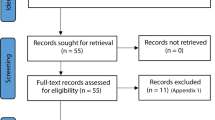
The search revealed a total of 2328 records from databases and 19 through other sources. After the removal of duplicates, titles abstracts of 1301 of them were screened, which resulted in 32 articles for full text assessment. Final scrutiny resulted in the inclusion of eight articles in the SR13,14,15,16,17,18,19,20. The details of search results, excluded studies and the reasons for exclusion are given in Fig. 1 and the online Supplementary Information.

The details of the searches, scrutiny and selection, along with the reasons for the exclusion.
Quality assessment
Risk of bias was found to be low in all the studies except Ahmed et al. which had moderate risk20. The paucities regarding the strategies to deal with confounding factors were identified in four studies13,15,17,20 and a lack of clarity regarding inclusion criteria was seen in one study (Table 2)20.
Study characteristics
The studies had been published between 2014 to 2020 with three from 202018,19,20. Among them, three had been performed in Saudi Arabia17,18,20, two in India13,15, and one each in Kuwait16, United Arab Emirates19 and Brazil14. All the studies except Murali et al.13 and Costa et al.14 were cross-sectional in design15,16,17,18,19,20. All the studies reported a lack of awareness and inadequate knowledge among parents regarding the management of dental trauma and/or dental avulsion (Table 3)13,14,15,16,17,18,19,20.
Questionnaire characteristics
The mode of distribution of the questionnaire in the majority of studies was self-administration16,17,18,20, followed by personal interviews in two studies13,14. The mode of distribution was not mentioned in the two studies15,19. The questionnaire was available in two or more languages in three studies13,15,19, one language in two studies16,18. English language was the main language in three studies and used in combination with Tamil13, Hindi, and Bengali15 and Arabic19, Arabic had also been used in two other studies16,18. The sources of Questionnaires had been mentioned in only three studies15,16,18. The questionnaires had used objective questions13,14,15,16,17,18,20 while this detail was not available in one study (online Supplementary Information)19. The knowledge of parents was assessed by all the studies except one which evaluated the perception of parents14. Along with this, the attitude was evaluated in three studies13,15,18 and practice in one study13. The number of questions varied from 5 to 3313,14,15,16,17,18,19,20, the validity was not reported in three studies15,17,19 and reliability was not reported in one study (online Supplementary Information)13.
Sampling characteristics
The sampling strategy had not been mentioned in four studies13,14,15,20 while others had simple random (n = 2)16,19, stratified cluster random (n = 1)17, and convenience sampling (n = 1)18. The sample size had been statistically justified in four studies16,18,19,20 and it ranged from 15013 to 336717 parents. The parents had been recruited from the out-patient departments (OPD) (n = 2)13,15, health care centers (PHC) (n = 2)14,17, dental specialty centers (n = 3)17,18,19 and directly from the community in one study20. Five studies had included both the parents15,16,18,19,20 whereas the other three had been done in mothers13,14,17. There was variability in the age groups of parents, however, the majority of them ranged between 20–40 years. Costa et al14 included 15–18 years old pregnant women as one of the groups while three of them had an age category of 51–60 years too13,19,20. The marital status, details of off-springs and employment status had been mentioned in the study done by Al-Sehaibany et al.17 and Alharbi et al.18. Most of the parents were married with two children in both the studies17,18. Large number of parents were working (n = 244) in the study done by Al-Sehaibany et al.17 while Alharbi et al.18 had reported that most of the parents were unemployed (n = 2503). The majority of the parents were graduates or had a professional degree in four of the included studies16,17,18,19 while the education level was less than graduation in the other four studies13,14,15,16. The details of socio-economic status were given in two studies and it was reported as middle income status (online Supplementary Information)17,18.
Details of the questions
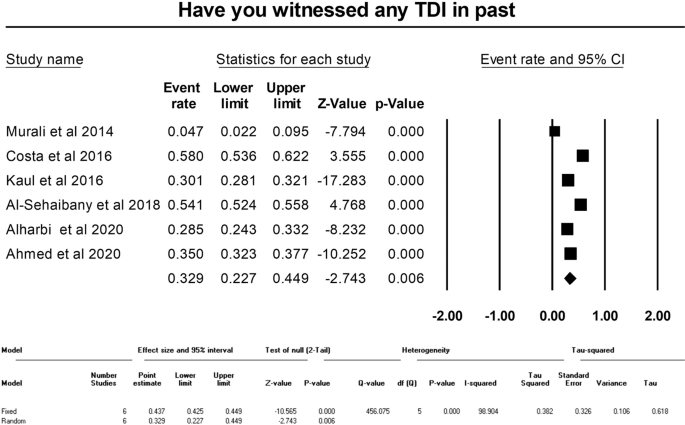
The questions included in three or more studies were used for making the “KAP-Heat Map” (Fig. 2). It was observed that 25–50% of the parents had witnessed any form of TDI in three15,18,20 and 50–75% in two of the six studies which included this question14,17. While only 4.7% of parents had witnessed it in one study13. When the parents had been enquired whether they had obtained any information about TDI in past, three of the four studies which included this question reported that 25–50% of the parents had responded in affirmation15,17,19 while it was <25% in the study done by Alyahya et al.16. The source was reported as a dentist in Alyahya et al.16 and Al-Sehaibany et al.17, while the information was obtained by “friends” in Alharbi et al. (online Supplementary Information)18. The appropriateness of immediate action after avulsion of tooth was correctly responded by 50–75% of the parents in four of the five studies15,17,18,19 and 25–50% in Murali et al.13. Three of the included studies had enquired about parent’s ability to identify the injured tooth with two studies reporting the correct response rates as 25–50%15,17 and 50–75 % in one study each20. Correct method of cleaning the soiled avulsed tooth was enquired in four studies and was known to 25–50% of the parents in three15,16,18 and 50–75% in one study13. When the parents were asked if they can perform the replantation of the avulsed tooth in their child, <25% of them responded in affirmation in two15,19 and 25–50% in the other two studies which included this question16,20. Awareness regarding the immediate or early replantation of avulsed tooth was known to 25–50% of the parents in all the three studies which had enquired about it16,17,18. Similarly, <25% of them were aware of the appropriate storage medium for the avulsed tooth in five15,16,17,19,20 and 25–50% in two of the seven studies which had enquired about it18,20. The question about the urgency to seek professional advice after TDI was included in five studies with 50–75% of the parents replying correctly in three studies13,16,18 more than 75% in one study15 and 25–50% in one study20. Dentists were reported as the first choice of the professionals to be contacted after TDI by >75% of the parents in three of the four studies which enquired about it15,16,18. It was 25–50% in the study done by Ahmed et al.20. More than 75% of the parents in all three studies which enquired about it, reported that they wanted to obtain more information about the management of TDI (Fig. 2)15,17,20. The questions included only in one or two studies have been detailed separately in the online Supplementary Information. The majority of parents responded negatively when asked “What did you do for the trauma?”20, “Can you identify the type of tooth injury?”14, “Have you (mother) ever had any dental trauma?”13 in one study each.

The question stems included in 3 or more studies (Blue: question not included, red: > 75%, dark yellow: 50–75%, lemon yellow: 25–50%, light yellow: < 25% sports persons and coaches giving correct responses. Width of columns was proportional to the number of studies which included the question stems.
Meta-analysis
Meta-analysis could be performed for three of the questions regarding witnessing of TDI in past, immediate action after tooth avulsion, and best storage media for storage of avulsed tooth. The pooled percentage of affirmative responses of the parents regarding witnessing TDI was 32.9% (95% CI: 22.7–44.9, random effects model, p = 0.006) (Fig. 3). The immediate action after tooth avulsion was known to 54.5% (95% CI: 50.2–58.8, random effects model, p = 0.042) of the parents (Fig. 4). The appropriate response rate regarding the storage medium for the avulsed permanent tooth was 21.3% (95% CI: 16.8–26.5, Random effects model, p < 0.001) (Fig. 5). All the meta-analyses displayed significant heterogeneity (I2 values ranging from 90.33 to 98.90) and publication bias (depicted in the Funnel plots and Egger’s test) (Figs. 3–5, online Supplementary Information).
The pooled correct response percentage for question regarding best storage media for storage of avulsed tooth.
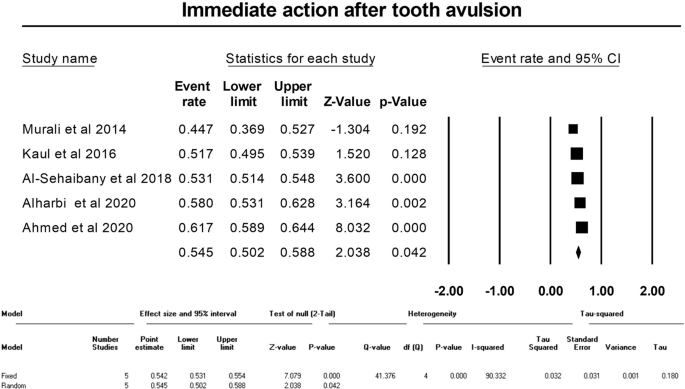
The pooled correct response percentage for question regarding immediate action after tooth avulsion.
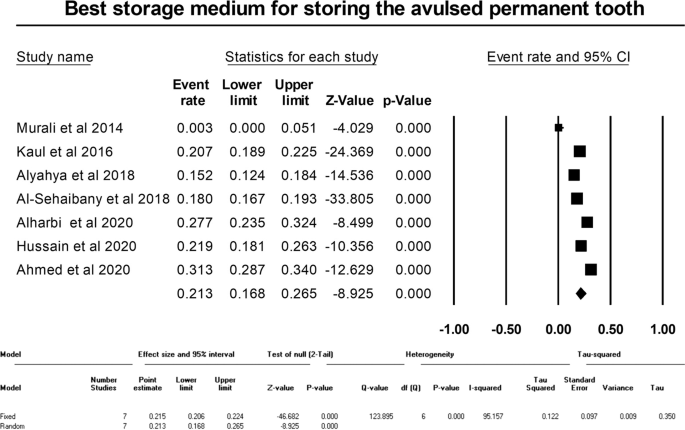
showing the pooled correct response percentage for question regarding best storage media for storage of avulsed tooth.
Grading of evidence
The strength of evidence regarding the outcomes of all the meta-analyses was graded to be very low (Table 4). This was done on the basis of the non-randomized nature of the included studies, the presence of heterogeneity, the presence of imprecision, the presence of publication bias and the presence of plausible confounding factors.
Discussion
Children and adolescents are highly vulnerable to injuries2,3. The changes in lifestyles have seen the advent of newer causative modalities of TDI27. As a result, it is important to educate the parents towards the basics of prevention and emergency management of TDI20. This serves dual purposes, firstly they will be able to attend to the emergency situation faced by their child more effectively and without panic, and secondly, they will be capable of understanding the importance of comprehensive dental treatment and follow-up for reducing the risks of adverse consequences of TDI13,14,15,16,17,18,19,20. IADT has clearly laid down the instructions that can be given to the parents when contacted during tooth avulsion6. The pandemic of COVID 19 also saw an increased involvement of parents in the health care of their children, even partnering in managing emergencies28. Evidence mapping in dental traumatology had highlighted that there is a paucity of evidence analysis in its preventive domain29. Previous works addressing this aspect tried to elucidate the global status of knowledge regarding prevention and emergency management of TDI among its stakeholders such as school teachers, sports persons and coaches, dental professionals, and non-dental health care professionals11,12,24,25. Hence it was envisaged that similar status for the parents will help in understanding their level of awareness and developing strategies for educating them.
The previous SRs assessing the knowledge levels had highlighted few of the problems associated with the synthesis of the qualitative research studies11,12. Hence the expert group for this SR took that into consideration and developed a protocol based upon the recommendations of evidence mapping, Cochrane handbook, and PRISMA guidelines21,22,29. The thoroughness of the literature search was ensured to address the research questions and no limitations of language or year of publication were considered. Inclusion and exclusion criteria ensured that only the studies involving parents (mother and/or father) were included and not the caregivers as that can add to the variations in the selected groups. Further, all the steps of the SR were performed by two experienced reviewers and the inter-examiner agreements were assessed. The strategy for solving the disagreement by consulting with a senior reviewer was also employed. Similarly, the extracted data was discussed by the expert group for better interpretation. These manoeuvres were considered important for increasing the reliability of the present SRs observations.
The strict inclusion criteria resulted in the exclusion of 97.54% of the articles during the screening of titles and abstracts and later 75% of those which were assessed during full-text evaluation. This might have also resulted in the exclusion of studies with high risk of bias. All the studies had been published in the last 8 years13,14,15,16,17,18,19,20 and all except one had originated from Asia14. This can be attributed to the criteria of including the studies which had used validated and/or reliable questionnaires, which was not an essential methodological characteristic in most of the studies done in past. The language of the questionnaire is related to the region of the study and the same was reflected in the present review, with English being the primary language in the majority of them13,15,19. It was observed that the sampling strategy was either not mentioned or not appropriate in most of the studies13,14,15,20, and the sample size had not been calculated in half of the studies13,14,15,17. These are important aspects of public health research and must be addressed in the future. The inclusion of > 50 years old parents was observed in several studies13,15,16,17,19,20. It was observed as a paucity and would have been better if the parents whose children were less than 14 years of age were included. Further, future researchers must also try to provide greater details of the study subjects such as education levels, occupation, and socio-economic status, which were deficient in several of the included studies.
KAP-Heat Map has been a useful adjunct in summarizing the details of the questionnaires in the previous SRs related to the assessment of knowledge11,12,24,25,26. The present review used the heat map of the questions included in three or more studies for creating the visual map of the knowledge status of parents and deriving the data for meta-analysis. Four of the studies exclusively evaluated the knowledge regarding emergency management of the avulsed permanent tooth15,16,18,20 and others too had several questions related to this injury13,14,17,19. More than half of the parents in the majority of the studies knew about the immediate actions to be performed after avulsion of tooth14,17,18,20, urgency to seek professional advice after TDI13,15,16,18. This reflected that the parents considered TDI as an emergency and their response was positive for the better care of their children. However, except for one study15, none of them reported having more than 75% of the parents with appropriate responses. It was good to see that more than 75% of the parents in one15 and more than 90% in two studies regarded dentists as the first choice of professionals to be contacted after TDI16,18. On the contrary, less than half of the parents in the majority of studies were confident of their ability to identify the injured tooth15,18, to clean the soiled avulsed tooth15,16,18 and to perform the replantation of the avulsed tooth in their child15,16,19,20. Similarly, 25–50% of the parents were aware of immediate or early replantation of avulsed tooth16,17,18 and <25% of them were aware of the appropriate storage medium for the avulsed tooth15,16,17,19. It was observed that though less than half of the parents in majority of studies had received any information about TDI in past15,16,17,19, more than 75% of them were interested in getting more information about management of TDI15,17,20. These trends and the pooled response percentages revealed by the meta-analysis highlight that the parents in the included studies did not have adequate knowledge regarding the key aspects of the emergency management of TDI. Though it was reported that they were keen on getting the information13,14,15,16,17,18,19,20. This matter must be given due importance by the dental and public health associations along with the associations of pediatric dentistry and dental traumatology, for developing validated modules and materials for educating parents globally. Mobile applications such as Tooth SOS and Injured tooth, and websites of traumatology associations such as IADT have tried to provide information to the public and content of similar nature can be used for increasing the awareness of the parents30. It was observed that none of the studies had enquired about the knowledge regarding the prevention of TDI. This must be part of the education modules for parents for making the play areas safe, reducing the sources of injury, and details about the use of mouth guards for their children. The major limitation of this SR is the heterogeneity observed among the primary studies and their nonadherence to the best practices of qualitative research and reporting, which also resulted in the very low strength of the evidence of the outcomes of the three meta-analyses. These must be addressed in future primary studies. SRs such as this one often suffers from problems in literature search and the existence of bias in selection. However, vigilant steps based on the best practices of evidence-based medicine were taken to reduce them.
Conclusion
The knowledge of the parents regarding the emergency management of TDI was found to be inadequate. Less than half of parents were confident of their ability to identify the injured tooth, to clean the soiled avulsed tooth, and perform the replantation of the avulsed tooth in their child. Similarly, less than half were aware of immediate or early replantation of the avulsed tooth and less than a quarter knew about the appropriate storage medium for the avulsed tooth. The majority of them were interested in obtaining information about dental trauma first aid. The included studies were mostly from Asia and had a high level of variability in their methodological and outcome assessment characteristics.
References
Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent Traumatol. 2018;34:71–86.
Andreasen JO. Traumatic injuries of the teeth. The CV Mosby. Co: St. Louis; 1972.
Glendor U. Epidemiology of traumatic dental injuries-a 12 year review of the literature. Dent Traumatol. 2008;24:603–11.
Levin L, Day PF, Hicks L, O'Connell A, Fouad AF, Bourguignon C, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: general introduction. Dent Traumatol. 2020;36:309–13.
Bourguignon C, Cohenca N, Lauridsen E, Flores MT, O'Connell AC, Day PF, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020;36:314–30.
Fouad AF, Abbott PV, Tsilingaridis G, Cohenca N, Lauridsen E, Bourguignon C, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2020;36:331–42.
Day PF, Flores MT, O'connell AC, Abbott PV, Tsilingaridis G, Fouad AF, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol. 2020;36:343–59.
Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 traumatically avulsed permanent incisors. 1. Diagnosis of healing complications. Endod Dent Traumatol. 1995;11:51–8.
Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 2. Factors related to pulpal healing. Endod Dent Traumatol. 1995;11:59–68.
Andreasen JO, Borum MK, Andreasen FM. Replantation of 400 avulsed permanent incisors. 3. Factors related to root growth. Endod Dent Traumatol. 1995;11:69–75.
Tewari N, Goel S, Rahul M, Mathur VP, Ritwik P, Haldar P, et al. Global status of knowledge for prevention and emergency management of traumatic dental injuries among school teachers: a systematic review and meta-analysis. Dent Traumatol. 2020;36:568–83.
Tewari N, Johnson RM, Mathur VP, Rahul M, Goel S, Ritwik P, et al. Global status of knowledge for prevention and emergency management of traumatic dental injuries in sports persons and coaches: a systematic review. Dent Traumatol. 2021;37:196–207.
Murali K, Krishnan R, Kumar VS, Shanmugam S, Rajasundharam P. Knowledge, attitude, and perception of mothers towards emergency management of dental trauma in Salem district, Tamil Nadu: a questionnaire study. J Indian Soc Pedod Prev Dent. 2014;32:202–6.
Costa VP, Amaral CC, Goettems ML, Pinheiro RT, Demarco FF. Maternal perception of the occurrence of traumatic dental injuries in children: a cohort study of south Brazil. Int Dent J. 2016;66:163–8.
Kaul R, Jain P, Angrish P, Saha S, Patra TK, Saha N, et al. Knowledge, awareness and attitude towards emergency management of dental trauma among the parents of Kolkata-An institutional study. J Clin Diagn Res. 2016;10:ZC95–101.
Alyahya L, Alkandari SA, Alajmi S, Alyahya A. Knowledge and sociodemographic determinants of emergency management of dental avulsion among parents in Kuwait: a cross-sectional study. Med Princ Pract. 2018;27:55–60.
Al-Sehaibany FS, Alajlan R, Almubarak D, Almaflehi N, Aljabaa A, AlBarakati SF. Knowledge on management of traumatic dental injuries among Saudi mothers. Clin Cosmet Investig Dent. 2018;10:123–8.
Alharbi R, Aboalshamat K, Alrabghi KK, Alassiri A, Bashammakh A, Alghamdi A, et al. Assessment of parents’ knowledge and attitudes on emergency management of permanent avulsed teeth in Western Saudi Arabia. Open Dent J. 2020;14:396–402.
Hussain A, Hashim R, Khamees A. Knowledge of tooth avulsion first aid management among parents residing in UAE. Braz J Oral Sci [Internet]. 2020;19:e206950.
Ahmed MA, Khurshid Z, Almajed OS, Al Bash AF, Alnaim A, Al Muhaidib DN, et al. Awareness of parents about the emergency management of avulsed tooth in Eastern Province and Riyadh. Eur Endod J. 2020;5:145–9.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, (Eds.). JBI Manual for Evidence Synthesis. JBI, 2020. https://doi.org/10.46658/JBIMES-20-08.
Tewari N, Sultan F, Mathur VP, Rahul M, Goel S, Bansal K, et al. Global status of knowledge for prevention and emergency management of traumatic dental injuries in dental professionals: Systematic review and meta-analysis. Dent Traumatol. 2021;37:161–76.
Tewari N, Jonna I, Mathur VP, Goel S, Ritwik P, Rahul M, et al. Global status of knowledge for the prevention and emergency management of traumatic dental injuries among non-dental healthcare professionals: A systematic review and meta-analysis. Injury. 2021;52:2025–37.
Srivastav S, Duggal I, Duggal R, Tewari N, Chaudhari PK, Pandey RM. Parental response to the feeding behavior problems in children with cleft lip and palate: a systematic review. Spec Care Dentist. 2021;41:559–71.
Tewari N, Mathur VP. Smartphones: the new risk factor for traumatic dental and facial injuries in children. Dent Traumatol. 2020;36:76–8.
Luzzi V, Ierardo G, Bossù M, Polimeni A. Paediatric Oral Health during and after the COVID-19 Pandemic. Int J Paediatr Dent. 2021;31:20–6.
Tewari N, Mathur VP, Kaur A, Sardana D, Rahul M, Tamchos R, et al. Evidence mapping and quality assessment of systematic reviews in dental traumatology. Dent Traumatol. 2021;37:17–36.
Tooth SOS. International Association of Dental traumatology. Version 2.3.4. IADT-Dental Trauma. [updated: 24 Nov 2021; Cited: 13 Jan 2022]. San Diego. CA. Available from: https://play.google.com/store/apps/details?id=com.iadtapp.toothsos&hl=en_IN&gl=US.
Author information
Authors and Affiliations
Contributions
The idea was conceptualized by NT. The team comprising of all the co authors designed the protocol and the methods of the systematic review. The review of literature was conducted by NT, SG and supervised by VPM. The data extraction was performed by SG, SS and supervised by VPM. The quality analysis was performed by SS, SG. Interpretation was performed by all the authors and co authors. The initial draft of the manuscript was prepared by NT, KB and SG. It was revised by all the authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tewari, N., Goel, S., Srivastav, S. et al. Global status of knowledge of parents for emergency management of traumatic dental injuries: a systematic review and meta-analysis. Evid Based Dent 24, 91 (2023). https://doi.org/10.1038/s41432-023-00883-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41432-023-00883-7
This article is cited by
-
EBD spotlight: Global parental knowledge of dental trauma
BDJ Team (2023)
