
Abstract
Data sources OVID Medline, EMBASE, and SCOPUS databases from 1991 till 2018. Manual search of the reference lists of review and related articles.
Study selection Prospective and retrospective clinical studies reporting survival rate of dental implants placed at sites of failed implants. The selection was limited to studies that comprised at least 15 partially edentulous patients and 20 dental implants. Only papers published in English language were included.
Data extraction and synthesis The first and second authors independently reviewed the literature and agreed on abstracted data. The Newcastle-Ottawa scale for cohort studies was used to assess quality and risk of bias in the selected studies. The primary outcome was the survival rate of replacement dental implants. The survival rate of replacement implants in relation to surface design (smooth versus rough) and implant sites (anterior versus posterior) were considered as secondary outcomes.
Results The mean survival rate of replacement dental implants was 86.3%. The follow-up period ranged from less than one year to more than five years. Rough-surfaced implants showed a significantly higher survival rate compared to smooth-surfaced implants (90% versus 68.7%). It was not possible to assess the impact of patient- or treatment-related factors on survival rate of replacement dental implants.
Conclusions Replacement dental implants have a high survival rate but it is less than that for initial implant placement. In retreatment, a higher survival rate is associated with rough-surfaced implants. It seems that initial implant failures are mostly related to modifiable risk factors.
Similar content being viewed by others

A Commentary on
Oh S L, Shiau H J, Reynolds M A.
Survival of dental implants at sites after implant failure: A systematic review. J Prosthet Dent 2019; DOI: 10.1016/j.prosdent.2018.11.007. [Epub ahead of print] PubMed PMID: 31027959.

GRADE rating
Commentary
Despite the high success rate of dental implants,1,2 failures may take place. This can be at the early stages following implant surgical insertion (preloading failure) or at late stages when in function (post-loading failure). Research shows that various factors are implicated in early and late failure of dental implants.3,4 When failure develops, the design of the planned/existing fixed/removable prosthetic dental restoration will need to be altered. With such a critical complication, a decision to replace failed implants becomes tempting for both patients and clinicians. However, it is not yet clear what chance there is for a successful outcome from such an intervention.
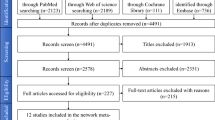
The current review aimed to systematically evaluate the success rate of replacement implants and the factors affecting the outcome of retreatment. The authors searched three large databases for prospective and retrospective clinical studies published in the English language in the period between 1991 and 2018. The inclusion was limited to publications that reported on at least 15 partially edentulous patients and 20 implants. The Newcastle-Ottawa scale for cohort studies was used as a tool to evaluate the risk of bias among the selected articles. Factors related to failure of replacement implants were analysed.
Following screening of the literature, eight clinical cohort studies were included in the final analysis. These were of retrospective design and reported the survival rate for 673 replacement implants provided for 557 patients. It was concluded that the average survival rate for the replacement implants was 86.3% after a follow-up between less than one year and more than five years. The authors found that rough-surfaced implants exhibited significantly higher survival rates than smooth-surfaced implants (90% versus 68.7%). No association was established between patient- or treatment-related factors and the survival rate of replacement implants.
In 2016, Zhou et al.5 published a systematic review on the same topic and included seven studies for the final assessment. The calculated survival rate for the implants placed in failed sites after the initial failure was 88.84% with a mean follow-up of 41.59 ± 16.77 months. A slightly higher survival rate was associated with replacement implants of wider diameters and improved surfaces. To enhance the potential for success, Zhou et al.5 recommended that any risk factors should be evaluated and modified, if possible, ahead of any steps for implant retreatment. When we look at the current review and the review of Zho et al.,5 we can notice that both picked up six of the same studies for final analysis. This explains the similar conclusions for the two reviews.
While it is clear the authors made great effort to prepare this review, there are many concerns that question the accuracy of the findings. We can note that the included studies were all clinical cohort studies of retrospective design. The shortcomings of retrospective studies, such as selection and recall bias and missing data items, are well-known to researchers.6 Hence, it was not surprising the overall quality score for the selected studies using the Newcastle-Ottawa scale was 4.6 ± 0.52, indicating moderate risk of bias. Another problem with this review is the heterogeneity of the selected studies. This can be recognised on review of Tables 2 and 3 in the article. The reader can notice wide variations among the selected studies in terms of design and assessed variables such as patient characteristics, timing of initial failure, location of failed implants and follow-up time. A considerable amount of missing information and variability in reported survival rates of replacement implants can also be noted. Also, the authors indicated disagreement between the included studies about the definition of implant failures. Moreover, the majority of the reported replacement implants were inserted at sites of preloading failure and only two studies evaluated the impact of implant surface modification on the survival rate of the implants. No control groups or control for age and gender were considered among the selected studies. The aforementioned points illustrate potentially considerable sources of bias which may undermine confidence in the precision of the conclusions offered.
Overall, this systematic review points to a big gap in our knowledge regarding the factors that control and affect the survival rate of retreatment implants. Longitudinal multicentre prospective cohort studies of good design and adequate sample size are needed if solid evidence is to be established regarding the survival of replacement implants and the best approach for their placement.
References
Pjetursson B E, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res 2012; 23 (Spec Iss): 22-38.
Lee C T, Chen Y W, Starr J R, Chuang S K. Survival analysis of wide dental implant: systematic review and meta-analysis. Clin Oral Implants Res 2016; 27: 1251-1264.
Sakka S, Baroudi K, Nassani M Z. Factors associated with early and late failure of dental implants. J Investig Clin Dent 2012; 3: 258-261.
Al-Sabbagh M, Bhavsar I. Key local and surgical factors related to implant failure. Dent Clin North Am 2015; 59: 1-23.
Zhou W, Wang F, Monje A, Elnayef B, Huang W, Wu Y. Feasibility of dental implant replacement in failed sites: a systematic review. Int J Oral Maxillofac Implants 2016; 31: 535-545.
Euser A M, Zoccali C, Jager K J, Dekker F W. Cohort studies: prospective versus retrospective. Nephron Clin Pract 2009; 113: c214-c217.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nassani, M. What is the survival rate of dental implants placed at sites of failed implants?. Evid Based Dent 20, 95–96 (2019). https://doi.org/10.1038/s41432-019-0047-0
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41432-019-0047-0
