
Abstract
Genetic testing can provide valuable information to mitigate personal disease risk, but the use of genetic results in life insurance underwriting is known to deter many consumers from pursuing genetic testing. In 2019, following Australian Federal Parliamentary Inquiry recommendations, the Financial Services Council (FSC) introduced an industry-led partial moratorium, prohibiting life insurance companies from using genetic test results for policies up to $AUD500,000. We used semi-structured interviews to explore genetic test consumers’ experiences and views about the FSC moratorium and the use of genetic results by life insurers. Individuals who participated in an online survey and agreed to be re-contacted to discuss the issue further were invited. Interviews were 20–30-min long, conducted via video conference, transcribed verbatim and analysed using inductive content analysis. Twenty-seven participants were interviewed. Despite the moratorium, concerns about genetic discrimination in life insurance were prevalent. Participants reported instances where life insurers did not consider risk mitigation when assessing risk for policies based on genetic results, contrary to legal requirements. Most participants felt that the moratorium provided inadequate protection against discrimination, and that government legislation regulating life insurers’ use of genetic results is necessary. Many participants perceived the financial limits to be inadequate, given the cost-of-living in Australia. Our findings indicate that from the perspective of participants, the moratorium has not been effective in allaying fears about genetic discrimination or ensuring adequate access to life insurance products. Concern about genetic discrimination in life insurance remains prevalent in Australia.
Similar content being viewed by others


Introduction
Genetic tests can provide consumers with valuable information to mitigate their risk of disease or enable early detection and/or treatment. As the utility and prevalence of genetic testing increases, ethical, legal, and social issues (ELSI) that arise with genetic testing should also be monitored. An ELSI consideration of global concern is the potential for genetic discrimination (GD). This is particularly relevant for risk-rated insurance underwriting. International research demonstrates that many consumers who have undergone or been offered genetic testing are concerned about insurance implications of genetic testing, and in some cases choose not to have testing or participate in genomic research studies [1,2,3,4,5,6,7,8].
Use of genetic tests by Australian life insurers and concerns about genetic discrimination
In Australia, health insurance is community-rated; therefore, no individual characteristics, including genetic tests are used in underwriting [3]. However, under section 46 of the Disability Discrimination Act 1992 (Cth), risk-rated insurance companies (including life insurers) can legally use genetic test results to assess individual risk for insurance products, as long as they have actuarial data to justify doing so. This can lead to GD, and fear of such discrimination impacts uptake of genetic testing in Australia, both for clinical tests and research participation. One study found that when informed about potential life insurance implications, people were 50% less likely to proceed with genetic testing [9]. A recent survey of the Australian general public (n = 1060) found that although 92% of adults were willing to have genetic testing for medically actionable disease risk, 86% said their willingness would be negatively affected by the possibility of GD [10]. A study regarding attitudes towards genomic data sharing found that while 72% of participants were willing to donate identifiable genomic data for not-for-profit research, 83% expressed high concern about potential GD by life insurers [11].
Historical GD studies have reported numerous cases of adverse treatment of consumers by life insurers on the basis of genetic test results [12, 13]. A 2019 study by authors of this paper surveyed 174 consumers with cancer-predisposing variants and reported 49 instances of consumers with difficulties obtaining life insurance [14]. Half of those consumers had no symptoms or history of cancer and had taken proactive measures to mitigate future risk.
Global approaches to regulating genetic discrimination
Many countries have restricted the use of genetic test results to assess individuals for risk-rated insurance products. Canada adopted the Genetic Non-Discrimination Act (GNA) in 2017, which prohibits the use of genetic information in services including insurance [15], with no exceptions or financial limits. In the United Kingdom (UK), since 2001 an agreement has been in place between the insurance industry and government, that prohibits the use of genetic test results in underwriting policies [16]. This applies to all results except for Huntington’s disease, for which predictive results must be disclosed to insurers for death cover policies >£500,000. All other results are protected without any financial limit. Numerous other countries, including in Asia and much of Europe, have banned or restricted the use of genetic results by insurers [2, 17,18,19].
The 2008 Genetic Information Non-Discrimination Act (GINA) in the United States of America bans the use of genetic results in health insurance. Regulation of life insurers has been approached at the state level, with Florida recently introducing a ban on use of genetic results in life insurance [20]. Public awareness of these protections has been an ongoing challenge, with studies showing poor awareness of GINA and its protections [21,22,23].
The Australian Insurance Moratorium
Following an inquiry into the life insurance industry, the Australian Parliamentary Joint Committee on Corporations and Financial Services (PJC) recommended that life insurers implement a ban on using genetic results in life insurance underwriting, similar to that in the UK, and that the Australian Government consider whether legislation is required in the future [24]. The Australian Government did not respond to these recommendations. However, the Financial Services Council (FSC)—the peak body for Australian life insurance companies at the time - introduced an industry-led, self-regulated moratorium prohibiting insurance companies from requesting or using genetic test results for policies up to $AUD500,000 [25], effective from July 2019. In 2023, Australian life insurers moved from the FSC and formed the Council of Australian Life Insurers (CALI). CALI is now responsible for self-regulating the Life Insurance Code of Practice, which incorporates the moratorium initially introduced by FSC.
Concerns regarding industry self-regulation have been raised by several Australian Government inquiries in the past five years [24, 26]. We have reported elsewhere that both health professionals [27, 28] and genetic researchers [29] believe government regulation is required, and authors of this paper have called on the Australian Government to implement independent regulation on the use of genetic information [29]. Following these calls but prior to the publication of this manuscript, the Australian Government announced in November 2023 a consultation into the use of genetic test results in life insurance underwriting [30, 31]. The consultation paper included three possible policy options – do nothing; implement a total or partial legislative ban on life insurers accessing or using genetic results in underwriting; or legislate financial limits, above which life insurers will be allowed to ask for and use applicant’s genetic results. That consultation closed on 31 January 2024, and the Government is currently considering its policy response.
It is critical to monitor whether the FSC moratorium is achieving its goal of ensuring consumer access to life insurance, and meeting the aims of the PJC recommendations, including reducing the fear of GD and hesitation surrounding genetic testing. The Australian Government (via the Medical Research Future Fund) funded the Australian Genetics and Life Insurance Moratorium: Monitoring the Effectiveness and Response (A-GLIMMER) project to conduct this task from 2020–2023 [32, 33]. The present study is a part of the A-GLIMMER project and adds to the findings of an earlier paper from the A-GLIMMER project which reports findings from a survey with consumers [34]. Our research question in the present study was to explore at a deeper level the understanding, views, and experiences of consumers regarding the FSC moratorium and the use of genetic test results in life insurance underwriting. Here we report the analysis of qualitative interviews with consumers who have undergone or been offered genetic testing.
Materials and methods
Through the broader A-GLIMMER project, an online survey (Supplementary file S1) was conducted with consumers who had taken or been offered a genetic test for disease risk, to explore their opinions and experiences about genetic testing and the FSC moratorium. The findings of that survey, spanning experiences before and after the FSC moratorium’s introduction, have been published separately [34]. To gain a more detailed and contextualised understanding of consumers’ experiences and views, we invited a sub-set of survey respondents to participate in qualitative interviews [35].
Survey respondents who had undergone predictive or diagnostic testing were eligible to participate. Predictive testing refers to testing in individuals with no known symptoms of disease; diagnostic testing takes place where symptoms are already apparent. Diagnostic testing can lead to predictive cascade testing of relatives for many conditions, and diagnostic testing is frequently the method by which at-risk families are first identified. Accordingly, the views and experiences of individuals who have undergone either predictive or diagnostic testing are directly relevant to an understanding of the impact of GD, and discrimination fears, on patients and families. People who were offered but had not yet undertaken (or had declined) genetic testing were also eligible to participate. The views of people who are deciding whether to have or have declined genetic testing are also critical to understanding the impact of GD.
To be eligible, participants had to be over the age of 18 years, live in Australia, and be able to read and speak English. Only individuals who consented to being contacted further in the online survey, and provided viable contact data, were invited to participate.
Recruitment
Participants were initially recruited to the online survey through consumer support groups, and invitations shared by social media and email [34]. All survey participants who indicated they were willing to be contacted further were eligible for the present study. Potential participants were invited for interview via email, and purposive sampling was used to select participants whose experiences would be most relevant in answering the research question. Participants who reported experiences of discrimination since the moratorium’s introduction in July 2019 were prioritised, to ensure cases of GD, which can be difficult to capture, were explored and reported. Secondly, we prioritised participants who reported that GD considerations and/or the moratorium’s existence had influenced their decision to have genetic testing and/or to apply for life insurance (either positively or negatively). Additionally, we endeavoured to recruit participants with a range of views, to explore different perspectives. For example, despite the strong majority view on some issues in the quantitative data [34], such as the need for further regulation of the use of genetic test results by insurers, we purposely invited several participants who had expressed a contrary view.
One individual who had not completed the online survey contacted the research team independently to express interest in being included in the research. Given the aim of the qualitative study was to gather experiences and views of people who had undergone or been offered genetic testing, the study investigators checked the individual’s eligibility and sought written consent from the individual.
Data collection and analysis
The semi-structured interview guide included topics regarding participant understanding and opinions of the moratorium, motivations for genetic testing and experiences regarding GD. The interview guides were adapted for each participant, based on their initial survey responses (see Supplementary file S2 for one participant schedule). All interviews were audio-recorded and transcribed verbatim.
Inductive content analysis
Inductive content analysis was performed [36], using the program NVivo (Release 1.6.2). This approach seeks to gain meaning from the dataset without a pre-established framework of categories [36].
All transcripts were thoroughly reviewed by CM for content familiarisation and to ensure accuracy between the audio recording and transcript. Transcripts were coded broadly by CM. A subset of transcripts were independently reviewed by LG, and codes were discussed between authors to ensure consistency. A coding schema was established from the first 7 transcripts (Supplementary file S3) by collating codes into preliminary content categories. The remaining transcripts were coded (and the initial 7 re-coded) to these categories (see Supplementary file S4 for a coded transcript). Once all transcripts had been coded, CM performed second-round coding to ensure no new categories were present and that saturation had been reached. From these data, the preliminary categories were discussed and refined into the final categories presented.
This study received approval from the Monash University Human Research Ethics Committee (ID 22576).
Results
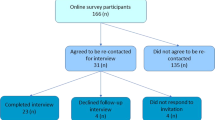
Of the 102 survey participants who consented to recontact, 39 were invited and 26 were interviewed. One additional interviewee, who met the inclusion criteria, was recruited through the recommendation of a study participant. Interviews were conducted between June and December 2022.
Total participant demographics (n = 27) are in Tables 1 and 2, with 52% female, and a mix of age groups, genetic testing types and associated conditions.
Inductive content analysis results
Initial analysis identified a preliminary list of 16 content categories and 12 sub-categories (see Supplementary file S3). The preliminary content categories were assessed and refined into five final representative categories, (Fig. 1) with 12 corresponding sub-categories. Verbatim quotes have been selected to represent each of these categories, and additional quotes have been included in tables accompanying the text to demonstrate the breadth of responses .

Summary of main categories identified.
Category 1: GD concerns affect genetic testing decisions (Table 3)
Despite the FSC moratorium, participants reported that concerns about their ability to access life insurance affected genetic testing decisions (Subcategory 1.1).
“That was really my primary concern because I’ve got two young kids now too, so I didn’t want to make myself as the primary income earner, uninsurable purely because of a genetic test.”
[Aaron, Lynch syndrome (untested), 41y]
Some participants mentioned at-risk relatives declining genetic testing because of GD fears.
“Even in my extended family there’s loads – there’s quite a few people who haven’t done genetic testing because they don’t want to be denied insurance cover… They’re not getting regular scans. They’re putting their health on the back foot because of all this. This is ridiculous.”
[Vivienne, Hereditary breast and ovarian cancer (positive test result), 34y]
Some participants also reported GD concerns affected their decisions around life insurance applications - some reported not bothering to apply for life insurance policies, because they believed or had been advised that they would be unsuccessful (Subcategory 1.2).
Several participants reported concerns about their genetic results affecting their children’s future access to life insurance directly impacting family communication about testing (Subcategory 3).
“Both of my girls now are probably at the age where they should be tested, but I’m not letting them get tested until they start working and they’re able to pay for life insurance.”
[Jill, Lynch syndrome (positive test result), 53y]
Category 2: Consideration of risk mitigation/management (Table 3)
Participants commonly described risk mitigation as a key reason for having genetic testing. Many were concerned that insurance companies were using genetic test results to underwrite policies, but not considering management and mitigation (Subcategory 2.1).
“My lifestyle, with my medication, quite possibly puts me at a lower risk level than what some other person who doesn’t take reasonable care of their health… basing your risk just on your condition and not on how it’s being managed is wrong.”
[Ian, Familial hypercholesterolaemia (positive test result), 53y]
Many participants also mentioned concerns with insurers taking a “blanket approach” to declining cover or penalising applicants with genetic test results. (Subcategory 2.2).
“I felt that it was pretty unfair to take this blanket approach … based on the limited knowledge of those genetics at the time. And I would imagine the even more limited knowledge of those genetics in the underwriters.”
[Chris, Mitochondrial disease (positive test result), 50y]
Some participants, who held a minority view, stated that insurance companies should be able to consider genetic tests in their underwriting, though there was still an expectation that risk-reducing measures would be taken into account as well .
“I don’t think there should be any exceptions… I dare say most people with a genetic disease it’s not their fault, but we live in a commercial world.”
[Harry, Autosomal dominant polycystic kidney disease (positive test result), 62y]
“I know it’s controversial, but I think – because a life insurer’s job is to assess risk, and I think that [genetic results] is key information to doing that. And because there are things that you can do for most things to reduce your risk, I think that it would only be fair that life insurers also take into account the measures that you’re taking to reduce your risk. But I get it. It’s hard, you get discriminated against. But that’s essentially what pricing for life insurance is."
[Trisha, Lynch syndrome (positive test result), 38y]
Category 3: Distrust of insurance industry and self-regulation (Table 4)
Many participants expressed distrust of the insurance industry, with several noting the poor history of self-regulation (Subcategory 3.1).
“Any industry-led model has never been particularly successful, and even more so in the human or the financial services in the world… I do think it should be in legislation; at the very least it should be in an act of parliament that declares the sanctity of the genetic information.”
[Rosie, Hereditary breast and ovarian cancer (negative test result), 56y]
“There’s so many examples of industry led agreements that just aren’t worth the paper they’re written on.”
[Natalie, Porphyria (untested), 43y]
Some participants expressed concern that the insurance industry is driven solely by financial motivations (Subcategory 3.2).
“I have no confidence whatsoever in the insurance industry to manage themselves because I don’t believe their interest are with me as the individual. (…) They’re with their shareholders. That’s why government should bloody mandate it.”
[Aaron, Lynch syndrome (untested), 41y]
“The Government you would hope would have the greater good in mind and the public good rather than from the point of view of a company with shareholders.”
[Frank, Huntington’s disease (negative test result), 41y]
Participants shared concerns about lack of certainty around the FSC moratorium continuing in the future. (Subcategory 3.3).
“If it’s not really legislated, then they can just pull out of it at any point in time. I don’t trust them to honour it.”
[Jill, Lynch syndrome (positive test result), 53y]
One participant, however, did not believe government regulation is needed, stating that insurers should be able to ask for what information they need to be aware of the risk.
“From a commercial point of view they should be able to make that decision, but that’s their decision rather than a government saying, “you must do this, you must provide all those details”
[Harry, Autosomal dominant polycystic kidney disease (positive test result), 62y]
Category 4: Financial limits are inadequate (Table 4)
Many participants mentioned that the moratorium’s financial limits are not high enough to cover their financial needs. Participants were worried that the current limits of $AUD500,000 for life insurance and $AUD4000/month for income protection would be insufficient to adequately care for their families’ needs (Subcategory 4.1).
“The dollar values need to reflect true dollar costs of the current Australian cost of living... I don’t know any of us that have got less than a million dollars’ worth of life insurance these days. $500,000 is two-fifths of stuff all.”
[Rosie, Hereditary breast and ovarian cancer (negative test result), 56y]
“I’d just still leave my family with a debt. (…)I think that’s the token effort is we’ll give you 500,000 (…) Maybe 500,000 10 years ago was good, but [now] it doesn’t buy you shit.”
[Oliver, Peutz-Jeghers syndrome (positive test result), 45y]
Some participants believed that there should be no financial limits at all to the protection offered (Subcategory 4.2). While most participants felt the financial limits were inadequate, a few participants noted that financial limits are a way for insurance companies to remain sustainable, and that ‘having some cover is better than no cover’ [Frank, Huntington disease (negative test result), 41y].
Category 5: Awareness of the FSC moratorium is lacking (Table 4)
Many participants reported that they were not previously aware of the FSC moratorium. The lack of awareness raised concerns around its effectiveness, some stating that they were not sure insurers or even genetic health professionals were aware of the agreement (Subcategory 5.1).
Some participants also pointed out that there is socioeconomic privilege in being aware of the FSC moratorium, and expressed concern for those without their resources or education (Subcategory 5.2).
“Others, that may not have the resources or even the level of education that maybe our family have, that don’t quite understand the nuances and the terminology and the wording and that kind of thing, that it can be quite biased towards the insurance companies.”
[Laura, Mitochondrial disease (positive test result), 61y]
This was echoed by another participant, who upon learning about the moratorium, wrote to her insurance company to dispute the exclusions put on her policy.
“It’s [the moratorium] made a difference in my life, so I’m very thankful for that. But maybe the key is just to get it out there, to make sure that people are aware that they have those rights. Because if I didn’t look it up and then kind of question them, I would have probably just accepted [the exclusions]”
[Dani, Hereditary breast and ovarian cancer (positive test result), 43y]
Discussion
This study explored the views of people who have had or been offered genetic testing for disease risk on the FSC moratorium and their experiences with GD. Our results show low trust in the life insurance industry’s self-regulation, and strong support for legislation from the Australian Government. Even after the introduction of the moratorium, these consumers remained concerned about the implications of their genetic test results on life insurance, and these concerns affected decision-making about genetic testing. Participants also showed little knowledge of the moratorium, or were concerned about others not being informed about it.
Distrust of self-regulation
We have previously reported concerns about industry self-regulation of insurer use of genetic tests [27, 28, 37] and similar findings are reported here. Concerns about industry self-regulation have also been expressed through formal government inquiries, including the 2019 Australian Royal Commission into Misconduct in Banking, Superannuation and Financial Services Industry, which found that insurance companies were not always acting in utmost good faith, and misconduct occurred without wrongdoers being held accountable [26].
Participants in our study raised concerns that the self-regulated nature of the moratorium means the agreement could be revoked at any time, and that insurers are inherently focussed on their own financial interests rather than those of consumers, making self-regulation inappropriate. These views are consistent with the views of health professionals [27, 28] and researchers [29] previously surveyed through the A-GLIMMER study, who expressed strong majority views that government legislation is required on this issue.
Impact of discrimination concerns
The FSC moratorium acknowledges the concern of GD in life insurance and the importance of not dissuading the public from genetic testing [25]. However, our study provides concerning evidence that some participants and their at-risk family members continue to decline genetic testing because of GD fears. One participant’s reports of intentionally dissuading their children from testing because of potential insurance implications, despite awareness of the benefits of testing, are concerning.
Most participants in our study had already had genetic testing. This suggests the value they saw in genetic testing may have outweighed GD concerns for themselves, though many remained concerned about GD implications. Importantly, this suggests consumers may consent to genetic testing despite having significant fears of insurance implications, because of the health risks they face in not having testing. Similar findings arose from the A-GLIMMER study with genetic researchers, who reported that many individuals are afraid of insurance implications but continue with genetic testing despite them, if the need for a diagnosis outweighs the financial concerns [29]. This is consistent with international findings that significant proportions of people who had proceeded to have genetic testing did so despite being worried about the insurance implications of having the test [5,6,7].
Consideration of risk mitigation
Genetic testing for medically actionable diseases can allow for risk mitigation in the form of lifestyle, screening and/or preventive measures. Some individuals who have had predictive testing and can proactively manage their risks may be in a better preventative health position than those who decline testing. For example, familial hypercholesterolaemia (FH) is the most common cause of premature cardiovascular disease, but is largely undiagnosed in the general population [38]. When FH is well-managed, the overall risk of myocardial infarction can be reduced by 76%, similar to the general population [39]. Similarly, risk reduction surgery for individuals with a BRCA1/2 pathogenic variant can reduce breast and/or ovarian cancer risk to below general population levels [40].
The FSC moratorium states that insurance companies consider evidence-based treatment or preventative measures when underwriting policies [25]. The Disability Discrimination Act 1992 (Cth), also requires that insurance companies only discriminate on actuarial grounds, meaning all evidence of risk reduction must be considered. Our study showed low awareness of insurers’ obligation to consider risk management. Additionally, an earlier study found that only 15% of Australians knew how to lodge an official complaint if they felt they had been mistreated based on their genetics [12]. The poor transparency in insurers’ decision-making [37], and limited recourse to appeals for affected consumers [14, 41], further limit the efficacy of the FSC moratorium’s efficacy in providing consumer protection.
Inadequacy of financial limits
Concerns about the financial limits of the FSC moratorium’s protection confirm our previous findings in which health professionals reported that the financial limits were too low to adequately protect their patients’ financial needs [27, 28]. Researchers and financial advisers have similarly raised concerns about the low financial limits [29]. Arguably, the financial limits set by the FSC moratorium do not reflect Australia’s current cost of living. As of May 2022, the average weekly earnings in Australia were $AUD1,769.80 [42] and the average home loan was $AUD609,000 [43], both significantly higher than the FSC moratorium’s current limits. The Australian economic climate in the 12 months following has seen significant inflation, interest rate rises and cost of living pressures, further increasing the amount of insurance coverage required. Several participants in our study noted that they would require well over $AUD1million of coverage to be adequately covered.
Some participants considered that financial limits may be necessary for the industry’s sustainability. However, no substantial evidence suggests this will be the case [44]. Canada has successfully banned the use of genetic test results in underwriting insurance without financial limits [45]. Substantial modelling commissioned by the Office of the Privacy Commissioner in Canada indicated that a complete ban would have negligible impact on insurers [46,47,48]. The UK Code [45] does not appear to have caused instability in the insurance market [44].
Poor awareness of the moratorium
Participants had limited awareness of the FSC moratorium. Consumers’ understanding of the life insurance implications of genetic testing is vital for individuals to make informed testing decisions. Further, as discussed above, awareness of the guidelines is necessary for protection of their rights in the process of gaining insurance.
Strengths of this study include structured interviews with consumers with a wide variety of experiences and genetic backgrounds, allowing for meaningful insight into consumer views about GD. We acknowledge the potential for response and selection bias in our study, as those who feel the most strongly about these issues may have responded to the original online survey and in turn been selected for this study. We purposively sampled several individuals with minority views to ensure they were captured in our qualitative analysis.
The deterrent effect of insurance fears on genetic testing has been demonstrated [9, 49, 50], but it is challenging to engage individuals who have declined genetic testing in research to explore their reasons. While we have reported some findings about such individuals, our study similarly struggled to recruit testing decliners. Further targeted research is required to reach individuals who have declined testing for insurance reasons and gain a deeper understanding of their decision-making.
Overall, our findings suggest that the FSC moratorium has not assuaged consumer fears regarding the risk of GD or access to life insurance. Improved access would require adequate protections to meet consumer needs, consumer awareness, and confidence that insurers would comply. Unfortunately, consumers continue to have concerns across these areas. Participants stated a strong preference for government regulation to ensure adequate protection against GD in life insurance and provide certainty to individuals considering genetic testing. The Australian Government is now considering its policy response to its public consultation into the use of genetic results in life insurance underwriting.
Data availability
Numerous data are made available via supplementary materials. Additional data can be made available on reasonable request.
References
Wauters A, Van Hoyweghen I. Global trends on fears and concerns of genetic discrimination: a systematic literature review. J Hum Genet. 2016;61:275–82.
Otlowski M, Taylor S, Bombard Y. Genetic discrimination: international perspectives. Annu Rev Genom Hum Genet. 2012;13:433–54.
Tiller J, Otlowski M, Lacaze P. Should Australia ban the use of genetic test results in life insurance? Front Public Health. 2017;5:330.
Chavarria-Soley G, Francis-Cartin F, Jimenez-Gonzalez F, Ávila-Aguirre A, Castro-Gomez MJ, Robarts L, et al. Attitudes of Costa Rican individuals towards donation of personal genetic data for research. Per Med. 2021;18:141–52.
Lee YM, McKillip RP, Borden BA, Klammer CE, Ratain MJ, O’Donnell PH. Assessment of patient perceptions of genomic testing to inform pharmacogenomic implementation. Pharmacogenet Genomics. 2017;27:179–89.
Rogith D, Yusuf RA, Hovick SR, Peterson SK, Burton-Chase AM, Li Y, et al. Attitudes regarding privacy of genomic information in personalized cancer therapy. J Am Med Inf Assoc. 2014;21:e320–325.
Waltz M, Cadigan RJ, Prince AER, Skinner D, Henderson GE. Age and perceived risks and benefits of preventive genomic screening. Genet Med. 2018;20:1038–44.
Wauters A, Van Hoyweghen I. Concerns about genetic discrimination after regulation: a qualitative study of the situation regarding BRCA and Huntington’s Disease in Belgium. Laws. 2018;7:17.
Keogh LA, van Vliet CM, Studdert DM, Maskiell JA, Macrae FA, St John DJ, et al. Is uptake of genetic testing for colorectal cancer influenced by knowledge of insurance implications? Med J Aust. 2009;191:255–8.
Tiller JM, Bakshi A, Brotchie AR, Green RC, Winship IM, Lacaze P. Public willingness to participate in population DNA screening in Australia. J Med Genet. 2022.
Vidgen ME, Kaladharan S, Malacova E, Hurst C, Waddell N. Sharing genomic data from clinical testing with researchers: public survey of expectations of clinical genomic data management in Queensland, Australia. BMC Med Ethics. 2020;21:119.
Taylor S, Treloar S, Barlow-Stewart K, Stranger M, Otlowski M. Investigating genetic discrimination in Australia: a large-scale survey of clinical genetics clients. Clin Genet. 2008;74:20–30.
Barlow-Stewart K, Taylor SD, Treloar SA, Stranger M, Otlowski M. Verification of consumers’ experiences and perceptions of genetic discrimination and its impact on utilization of genetic testing. Genet Med. 2009;11:193–201.
Tiller J, Morris S, Rice T, Barter K, Riaz M, Keogh L, et al. Genetic discrimination by Australian insurance companies: a survey of consumer experiences. Eur J Hum Genet. 2020;28:108–13.
Bombard Y, Heim-Myers B. The Genetic Non-Discrimination Act: critical for promoting health and science in Canada. Cmaj. 2018;190:E579–80.
HM Government and Association of British Insurers: Code on Genetic Testing and Insurance. 2018. Accessed from: https://www.abi.org.uk/data-and-resources/tools-and-resources/genetics/code-on-genetic-testing-and-insurance/.
Joly Y, Dupras C, Pinkesz M, Tovino SA, Rothstein MA. Looking beyond GINA: policy approaches to address genetic discrimination. Annu Rev Genomics Hum Genet. 2020;21:491–507.
Kim H, Ho CWL, Ho C-H, Athira PS, Kato K, De Castro L, et al. Genetic discrimination: introducing the Asian perspective to the debate. npj Genom Med. 2021;6:54.
The Geneva Association: Genetics and Life Insurance: A View Into the Microscope of Regulation. Zurich, Switzerland: 2017. Accessed from: https://www.genevaassociation.org/sites/default/files/ga2017_globalageing_genetics_and_life_insurance_0.pdf.
Rothstein MA, Brothers KB. Banning genetic discrimination in life insurance — time to follow Florida’s lead. N Engl J Med. 2020;383:2099–101.
Allain DC, Friedman S, Senter L. Consumer awareness and attitudes about insurance discrimination post enactment of the Genetic Information Nondiscrimination Act. Fam Cancer. 2012;11:637–44.
Dorsey ER, Darwin KC, Nichols PE, Kwok JH, Bennet C, Rosenthal LS, et al. Knowledge of the Genetic Information Nondiscrimination act among individuals affected by Huntington disease. Clin Genet. 2013;84:251–7.
Parkman AA, Foland J, Anderson B, Duquette D, Sobotka H, Lynn M, et al. Public awareness of genetic nondiscrimination laws in four states and perceived importance of life insurance protections. J Genet Couns. 2015;24:512–21.
Commonwealth of Australia: Life Insurance Industry; in: Parliamentary Joint Committee on Corporations and Financial Services (ed). Canberra, 2018.
Financial Services Council: FSC Standard No. 11: Moratorium on Genetic Tests in Life Insurance, 2019.
Hayne K: Final Report - Royal Commission into Misconduct in the Banking, Superannuation and Financial Services Industry. Canberra: 2019.
Dowling G, Tiller J, McInerney-Leo A, Belcher A, Haining C, Barlow-Stewart K, et al. Health professionals’ views and experiences of the Australian moratorium on genetic testing and life insurance: a qualitative study. Eur J Hum Genet. 2022;30: 1262–8.
Tiller JM, Keogh LA, McInerney-Leo AM, Belcher A, Barlow-Stewart K, Boughtwood T, et al. A step forward, but still inadequate: Australian health professionals’ views on the genetics and life insurance moratorium. J Med Genet. 2022;59:817–26.
Tiller J, Gleeson P, McInerney-Leo AM, Keogh L, Nowak K, Barlow-Stewart K, et al. Final Stakeholder Report of the Australian Genetics and Life Insurance Moratorium: Monitoring the Effectiveness and Response (A-GLIMMER) Project. https://doi.org/10.26180/23564538 Melbourne, Australia: Monash University, 2023.
Australian Government the Treasury: Press conference, Mural Hall, Parliament House, Canberra: Release of consultation paper on treatment of genetic testing information for life insurance. 2023. Accessed from: https://ministers.treasury.gov.au/ministers/stephen-jones-2022/transcripts/press-conference-mural-hall-parliament-house-canberra.
Australian Government The Treasury: Consultation: Use of genetic testing results in life insurance underwriting, 2023. Accessed from: https://treasury.gov.au/consultation/c2023-467047.
Tiller J, McInerney-Leo A, Belcher A, Boughtwood T, Gleeson P, Delatycki M, et al. Study protocol: the Australian genetics and life insurance moratorium-monitoring the effectiveness and response (A-GLIMMER) project. BMC Med Ethics. 2021;22:63.
Tiller J, Winship I, Otlowski MF, Lacaze PA. Monitoring the genetic testing and life insurance moratorium in Australia: a national research project. Med J Aust. 2021;214:157–159.e151.
Tiller J, Bakshi A, Dowling G, Keogh L, McInerney-Leo A, Barlow-Stewart K, et al. Community concerns about genetic discrimination in life insurance persist in Australia: A survey of consumers offered genetic testing. Eur J Hum Genet. 2024;32:286–94.
Vishnevsky T, Beanlands H. Qualitative research. Nephrol Nurs J. 2004;31:234–8.
Vears DF, Gillam L. Inductive content analysis: a guide for beginning qualitative researchers. Focus Health Prof Educ. 2022;23:111–27.
Newson AJ, Tiller J, Keogh LA, Otlowski M, Lacaze P. Genetics and insurance in Australia: concerns around a self-regulated industry. Public Health Genomics. 2017;20:247–56.
Watts GF, Sullivan DR, van Bockxmeer FM, Poplawski N, Hamilton-Craig I, Clifton PM, et al. A model of care for familial hypercholesterolaemia: key role for clinical biochemistry. Clin Biochem Rev. 2012;33:25–31.
Versmissen J, Oosterveer DM, Yazdanpanah M, Defesche JC, Basart DC, Liem AH, et al. Efficacy of statins in familial hypercholesterolaemia: a long term cohort study. Bmj. 2008;337:a2423.
Domchek SM, Friebel TM, Singer CF, Evans DG, Lynch HT, Isaacs C, et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. Jama. 2010;304:967–75.
Otlowski M, Taylor S, Barlowstewart K, Stranger M, Treloar S. The use of legal remedies in Australia for pursuing allegations of genetic discrimination: findings of an empirical study. Int J Discrim Law. 2007;9:3–35.
Average Weekly Earnings, Australia. Australian Bureau of Statistics, 2022. Accessed from: https://www.abs.gov.au/statistics/labour/earnings-and-working-conditions/average-weekly-earnings-australia/latest-release.
Lending indicators: Australian Bureau of Statistics, 2022. Accessed from: https://www.abs.gov.au/statistics/economy/finance/lending-indicators/latest-release.
Golinghorst D, de Paor A, Joly Y, Macdonald AS, Otlowski M, Peter R, et al. Anti-selection & genetic testing in insurance: an interdisciplinary perspective. J Law Med Ethics. 2022;50:139–54.
Prince AER. Comparative perspectives: regulating insurer use of genetic information. Eur J Hum Genet. 2019;27:340–8.
Office of the Privacy Commissioner of Canada: Statement on the use of genetic test results by life and health insurance companies, 2014.
Hoy M, Durnin M. The Potential Economic Impact of a Ban on the Use of Genetic Information for Life and Health Insurance: Office of the Privacy Commissioner of Canada, 2012.
Macdonald A: The actuarial relevance of genetic information in the life and health insurance context. Ottawa: Office of the Privacy Commissioner, 2011.
Keogh LA, Niven H, Rutstein A, Flander L, Gaff C, Jenkins M. Choosing not to undergo predictive genetic testing for hereditary colorectal cancer syndromes: expanding our understanding of decliners and declining. J Behav Med. 2017;40:583–94.
Keogh LA, Otlowski MF. Life insurance and genetic test results: a mutation carrier’s fight to achieve full cover. Med J Aust. 2013;199:363–6.
Funding
The project is supported by a grant from the Australian Government’s Medical Research Future Fund (MRFF), ref 76721. AML is funded by a National Health and Medical Research Council (NHMRC) Early Career Fellowship (ID 1158111). PL is supported by a National Heart Foundation Future Leader Fellowship (ID 102604). Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
JT conceived the project, designed the methodology, supervised CM and critically reviewed the manuscript. CM collected and analysed data and wrote the first draft of the manuscript. LG assisted with methodology, supervised CM and critically reviewed the manuscript. LK, AML, KBS, TB, PG, MD, IW, KN, MO, and PL assisted with study design, reviewed and contributed to development of methodology and provided critical review of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This project was granted approval by the Monash University Human Research Ethics Committee on 13 August 2021, ID number 22576, and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Muller, C., Gallacher, L., Keogh, L. et al. “Uninsurable because of a genetic test”: a qualitative study of consumer views about the use of genetic test results in Australian life insurance. Eur J Hum Genet 32, 827–836 (2024). https://doi.org/10.1038/s41431-024-01602-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41431-024-01602-1
This article is cited by
-
Hitting the heights with CiteScore
European Journal of Human Genetics (2024)
