
Abstract
GJB2 was originally identified in severe, non-syndromic sensorineural hearing loss (SNHL), but was subsequently associated with mild and moderate SNHL. Given the increasing utilisation of genetic testing pre-conceptually, prenatally, and neonatally, it is crucial to understand genotype-phenotype correlations. This study evaluated the nature and frequency of GJB2 variants in an Australian paediatric population with varying degrees of SNHL ascertained through newborn hearing screening. Audiograms from individuals with GJB2 variants and/or a GJB6 deletion (GJB6-D13S11830) were retrospectively reviewed (n = 127). Two-thirds were biallelic (homozygous/compound heterozygous) for pathogenic/likely pathogenic variants of GJB2 and/or GJB6 (n = 80). The most frequent variant was c.109 G > A, followed by c.35delG and c.101 T > C. Compared to biallelic carriage of other GJB2 variants, c.109 G > A positive individuals (homozygous/compound heterozygous) were more likely to have mild HL at their initial and latest audiograms (p = 0.0004). Biallelic carriage of c.35delG was associated with moderately-severe or greater SNHL at both initial and latest audiograms (p = 0.007). The c.101 T > C variant presented with milder SNHL and U-shaped audiograms (p = 0.02). In this agnostically identified cohort, mild SNHL predominated in GJB2/GJB6 carriers in contrast to previous studies targeting individuals with significant loss. Consequently, c.109 G > A, associated with milder phenotypes, was the most frequent. This study provides valuable data to support prognostic confidence in genetic counselling.
Similar content being viewed by others

Introduction
Sensorineural hearing loss (SNHL) is the most common congenital sensory disorder, affecting 1 in 500 newborns [1]. It can adversely affect language development, cognition, psychosocial wellbeing and quality of life, educational attainment, and economic independence at various stages of life [2]. Approximately 50% of congenital hearing loss is Mendelian, with 30% of individuals having a recognised syndrome and 70% regarded as non-syndromic [3].
Non-syndromic hearing loss (NSHL) is heterogeneous with approximately 75% of early onset cases being inherited in an autosomal recessive manner [4]. Seventy-eight of the 124 NSHL genes are autosomal recessive [5], and the most frequently implicated gene is GJB2 (OMIM 121011), which is responsible for the protein gap junction protein beta-2 (connexin 26). However, a single GJB2 variant can lead to disease if coinherited with a variant in the contiguous gene GJB6, (OMIM 604418) gap junction protein beta-6 (connexin 30) in approximately 2% of cases [5, 6]. In addition, pathogenic variants in GJB2 can be associated with autosomal dominant inheritance in approximately 2% of cases [7].
Worldwide, GJB2 pathogenic variants account for 18–50% of prelingual NSHL [8]. In addition, GJB2 variants account for 30-50% of all cases of profound NSHL [9]. Widespread testing of GJB2 (and GJB6), reveals variable degrees of hearing loss (mild to profound), not always detectable at birth, which is usually bilateral, but occasionally unilateral, and can be progressive [3, 8].
Previous cohort studies identified a recurrent variant in GJB2 (c.35delG) estimated to account for approximately 60-70% of deafness in European, North African, Middle Eastern, Asian, North and South American populations [8, 10, 11]. A single study in an Australian paediatric population identified the c.35delG variant to be the most frequently implicated (38.03%) [12]. Other GJB2 variants have been implicated in other populations. Specifically, the c.235delC and c.109 G > A GJB2 variants are more frequently implicated in hearing loss in East Asian countries including Japan, Korea and China [10].
Mode of ascertainment affects the phenotypic spectrum associated with specific genes, where they are originally described in the most severe cases and, through wider testing practices are subsequently associated with more variable phenotypes, thus broadening the phenotypic spectrum [13, 14]. In some cases, variants are identified in healthy individuals who might never develop symptoms [13]. Thus, context (both timing of testing and target population) will affect genotypic and phenotypic findings, and the clinical significance of the results. This is highly relevant to the GJB2 story which was originally identified with predominantly severe/profound HL [15]. Nowadays, we are using genetic testing generally and GJB2 specifically in population screening. Many countries, including Australia, now have mature newborn hearing screening programs with high population coverage that result in identification of infants with mild congenital HL [16]. In addition, reproductive carrier screening has become more affordable, and many commercially available panels include GJB2 [17]. Therefore, it is vitally important to publish results from a range of contexts to ensure that clinicians have access to data from individuals with milder or minimally apparent phenotypes to ensure prognostic confidence in the likely spectrum of outcomes for the individuals undergoing screening [18].
There is significant genotypic and phenotypic variability in international studies, but limited data from Oceania. Of note, a recent systematic review identified that only 0.7% of publications about connexin gene variants were from Australia [11]. Thus, this study reviewed all GJB2 positive cases from the Queensland state laboratory, documented all GJB2 and GJB6 genotypes, and reviewed audiological and clinical data to identify possible genotype-phenotype correlations for a Queensland paediatric population with NSHL.
Methods
Study population and context
Queensland is an Australian state, where 99% of the 60 000 babies born each year, have newborn hearing screening as part of a state-government funded program (‘Healthy Hearing Program’). Screen positive individuals are referred for follow up diagnostic assessment in accordance with a state-wide protocol https://www.childrens.health.qld.gov.au/resources/our-work/healthy-hearing/queensland-health-screening-protocols-and-guidelines [19]. This study includes children diagnosed with a HL through this pathway or those diagnosed with SNHL in later childhood (either through the targeted surveillance program or external referral). Included individuals were seen in specialised paediatric ENT and/or medical hearing loss clinics at Queensland Children’s Hospital and other public hospitals statewide who had subsequent genetic testing with Pathology Queensland. All individuals had undergone genetic testing between November 2014 and December 2019. Medical and audiological records of this paediatric population were retrospectively reviewed. Ancestral background information was not routinely available; however, recent census data shows that whilst English and Australian ancestry is more common (33.6% and 31.2% respectively), approximately 17.4% of the population identify as Asian with breakdowns of 6.5% from Southern and Central Asia, 6.4% from North-East Asia and 4.5% from South-East Asia. Of note, First Nations peoples (Aboriginal and Torres Strait Islander peoples) were recorded at 3.2% of 2021 census [20].
Genetic testing
Pathology Queensland is a state-wide service offering genetic testing for individuals diagnosed with HL. Specifically, the entire coding region of GJB2 is sequenced (Sanger sequencing) for all patients and no further testing is conducted on individuals found to carry biallelic variants. When GJB2 heterozygosity is identified, there is subsequent screening for a single GJB6 deletion (del(GJB6-D13S11830) due to the interactive association. The study was confined to all patients that undertook GJB2 and GJB6 testing during the study period. Patients with no detected variants were excluded from the study.
Medical records were reviewed for all cases including homozygous/compound heterozygous and heterozygous cases or a single GJB2 variant in the presence of a GJB6 deletion. Variant pathogenicity was initially evaluated by reviewing ClinVar [21] and the Deafness Variation Database [22] to determine prior association with disease. For all variants not reported in ClinVar, a Varsome assessment [23] rated their likely pathogenicity using the American College of Medical Genetics and Genomics guidelines and best practices for expert interpretation of genomic data [24]. Based on these categories individuals were classified as autosomal dominant pathogenic variant, homozygous for pathogenic variants, compound heterozygous for two pathogenic variants, compound heterozygous for two variants (at least one pathogenic), digenic (one GJB2, one GJB6), heterozygous for pathogenic/likely pathogenic variants or heterozygous for VUS/likely benign/benign variant. The hearing profiles were included for all variant carriers, but statistical analyses (see below) were limited to individuals with biallelic pathogenic/likely pathogenic variants.
Hearing assessment
Information relating to the severity of HL and a description of the audiogram was collated. The sensorineural (permanent) component of the HL was used in the cases with mixed (both sensorineural and conductive) HL, and we aimed to exclude temporary conductive HL, but the distinction was not always apparent during early testing. Degrees of HL were based on the classification system outlined by Goodman and Clark and include normal (≤20 dB HL), mild (21–40 dB HL), moderate (41–55 dB HL), moderately severe (56–70 dB HL), severe (71–90 dB HL), and profound (>90 dB HL). A four-frequency average was used to determine the degree of hearing loss [25, 26]. The audiograms were also assessed for shape (rising, sloping/descending, flat, U-shaped), symmetry (symmetrical, asymmetrical) and stability (fluctuating, progressive, stable) [27, 28]. (See Supplementary Table 1 for definitions of descriptors). If the HL was asymmetrical, it was graded according to the better hearing side. Audiometric testing was performed using a variety of age-appropriate standardised techniques for paediatric populations https://www.childrens.health.qld.gov.au/resources/our-work/healthy-hearing/audiology-diagnostic-assessment-protocol [19]. In cases where consecutive reports were available, the stability of the HL was also documented, by comparing audiogram results from the initial and most recent hearing assessment. Only patients with copies of audiograms in their medical record were included in the study. Audiology data was confirmed and supplemented through review of the QChild database, Queensland’s newborn hearing screening data management system which contains demographic and clinical information from screening.
Data analysis
All genetic and phenotypic data (extracted from patient medical records and QChild) were exported into Microsoft Excel. A descriptive statistical analysis was performed. Fisher exact statistical tests were used to determine whether specific genotypes were more frequently associated with milder or more severe audiological phenotypes as well as other audiological descriptors. Specific genotype-phenotype analysis was performed for individuals who had pathogenic or likely pathogenic variants that were inherited in a homozygous, compound heterozygous or autosomal dominant manner. Moderately-severe, severe and profound HL were grouped together due to sample size limitations. A p value < 0.05 was considered statistically significant.
Results
Study population
Of the 625 individuals with GJB2+/− GJB6 sequencing through Pathology Queensland during the study period (2014 to 2019), 134 had variants detected and sufficient audiological information. After review of patient medical records and QChild, seven patients had other known identifiable causes for their HL (three with absent cochlear nerves, two with enlarged vestibular aqueducts, one with Waardenburg syndrome and another with a chromosome 15q11.1 deletion) and were excluded. This left a total of 127 patients for analysis.
Demographics
The final 127 cohort consisted of 72 males and 55 females. The mean age at genetic testing was 1.8 years with the range between 2 months and 17 years. The median age of genetic testing was 4 months with 68% of the cohort having the testing under 12 months of age. Specific information about ancestral background was not consistently available.
Genetic Findings
In the cohort of 127 patients, 36 different GJB2 variants were identified in a homozygous (n = 45/127, 35.4%), compound heterozygous (n = 36/127, 28.3%), 1 digenic (heterozygous for GJB2 combined with the GJB6 del(GJB6-D13S11830) deletion) and autosomal dominant (n = 1) or heterozygous (n = 44/127, 34.6%) state. Of the 36 individuals with compound heterozygous variants, 3 had only one of the variants rated as pathogenic. Of the 44 individuals with heterozygous variants, 22 had variants that were pathogenic or likely pathogenic and 22 had variants that were of unknown significance, benign or likely benign. These 47 individuals were included in the demographic analysis but were treated separately in the genotype-phenotype analysis.
In total, only 80 individuals were biallelic for pathogenic/likely pathogenic variants including one heterozygous with autosomal dominant inheritance.
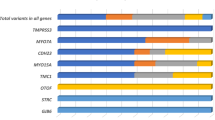
Three recurrent variants, c.109 G > A p(Val37Ile), c.35delG p.(Gly12Valfs*2), and c.101 T > C p.(Met34Thr) accounted for 48.4% (n = 77/159), 31.4% (n = 50/159) and 15.5% (n = 25/159) of all pathogenic or likely pathogenic variant alleles respectively. Furthermore, the c.109 G > A variant accounted for the majority of homozygous cases (n = 32/45, 71.1%). (See Fig. 1b). Table 1 demonstrates the distribution of the variants in the cohort for the 80 individuals with biallelic variants. Details of the remaining 47 individuals are presented in Supplementary Table 2.

a Whole cohort. b Homozygous group.
A single patient carried del(GJB6-D13S11830), in conjunction with a GJB2 c.101 T > C variant. The autosomal dominant variant, c.551 G > A, was identified in a case whose mother also had SNHL and had been previously reported in association with DFNA3 [29].
Biallelic cases: Hearing profiles
The specific genotype-phenotype analysis was performed on 80 individuals with biallelic or an autosomal dominant variant. The mean age at testing for this group was 1.8 years with a median age at testing of 4 months. The most frequent loss in the better ear was mild 43/80 (53.8%), with 10/80 initially coded as normal in the better hearing ear (12.5%), 11/80 moderate (13.8%), 7/80 moderately severe (8.8%), 2/80 severe (2.5%) and 6/80 profound (7.5%) (Fig. 1a). For the initial hearing assessments, one patient had missing data, but was included because their subsequent audiogram was available. 60/80 patients had subsequent audiogram data available to evaluate change in hearing over time. Proportions of children in the severity categories was similar between initial and latest assessments. (Supplementary Figure 1). Note that overall hearing was defined by the better hearing ear. 60 of the 80 patients in this group had information about stability and 49 of those had stable hearing profiles (49/60 = 81.6%) with most having mild HL (n = 25/60, 41.6%). Two patients had fluctuating hearing profiles with mild HL on their latest test (n = 2/60, 3.3%). Both individuals were homozygous for the c.109 G > A variant. The other 9 individuals (n = 9/60, 15%) had progressive HL. Further information can be found in Table 2a.
Ten of 80 (12.5%) patients demonstrated hearing that was coded as ‘normal’ in the better hearing ear at their initial hearing test. The genotype and further information about HL in these individuals is presented in Table 2b. The majority of these individuals had progression of their HL.
Heterozygous cases: Hearing profiles
The hearing profiles in heterozygous cases can be seen in Supplementary Table 2, Fig. 1a and Supplementary Figure 1b. Of the 47 individuals with heterozygous variants and those with variants of uncertain significance or likely benign, the hearing profiles were similar between the initial and latest assessment with nine not having follow up audiogram data. The proportions of SNHL severity at the initial time point were 15/47 (31.9%) normal in the better ear (more detail in Table 2) mild 21/47 (44.7%), moderate 8/47 (17%) and one each of moderately-severe (2.1%), severe (2.1%) and profound (2.1%) (Supplementary Figure 1b).
HL progression was assessable in 97 individuals (from both biallelic and heterozygous groups) who had audiograms at multiple time points and sufficient information to code HL stability. Progressive HL was seen in 15 total; 9/60 (15%) in the homozygous/compound heterozygous/AD group and 6/37 (16.2%) in the heterozygous/VUS/likely benign group. Genotypes of those individuals are presented in Table 2a and include the autosomal dominant variant, homozygous and compound heterozygous c.35delG and c.109 G > A as well as several other genotypes.
Biallelic cases: genotype-phenotype associations
The three most common variants had sufficient sample size for Pearson’s chi-squared or Fisher’s exact statistical test analysis for association between genotype and phenotypic characteristics and were all present in homozygous, compound heterozygous and heterozygous states (More detail in Table 1). Figure 1a demonstrates the degree of initial HL by zygosity and 1b demonstrates the degree of initial HL for the three most frequent variants in homozygous state. The most frequent variant, c.109 G > A, had sufficient numbers for analysis for phenotypic associations with both homozygous state and combination of homozygous/compound heterozygous, and c.35delG and c.101 T > C had sufficient numbers for this analysis of homozygous/compound heterozygous state.
Fisher exact statistical test analysis found that patients who were homozygous for c.109 G > A were much more likely to have mild HL and less moderately severe/severe/profound for both their initial and latest hearing tests (p = 0.0004 and 0.006 respectively) than the rest of the cohort. Individuals who were homozygous/compound heterozygous for the c.109 G > A variant were also significantly more likely to have mild HL (versus moderately-severe/severe/profound HL) as compared to those not carrying the c.109 G > A variant for both the initial (p = 0.00004) and most recent audiogram data (p = 0.0004) (Table 3).
Individuals who were homozygous/compound heterozygous for the c.35delG variant had significantly more moderately-severe/severe/profound HL than those with other genotypes at both time points (p = 0.007 and 0.007 respectively) (Table 3).
Individuals who were homozygous/compound heterozygous for the c.101 T > C variant had significantly more U-shaped and sloping audiograms than other audiogram configurations at the most recent time point (p = 0.02) (Table 4). There were no other significant associations between genotype and any of the other audiology descriptors (audiogram shape, symmetry or stability).
Genotype-Phenotype association: progressive HL and ‘normal’ hearing
Of the 10 individuals who were homozygous/compound heterozygous who had normal hearing in the better ear on the initial audiogram (Table 2b), 6 were homozygous for c.109 G > A. There were 2 individuals who were compound heterozygous for c.35delG/c.101 T > C who had unilateral HL at the initial time point and bilateral U-shaped HL at the most recent time point. Six of the 15 individuals with progressive HL (Table 2a) had at least one variant that was c.35delG.
Discussion
This study reports variant data from a geographical region which has been understudied to date. State-wide newborn screening (99% coverage), and follow-up GJB2/6 testing in screen positive individuals revealed biallelic and heterozygous carriage in association with predominantly mild hearing loss. The most frequent variant, c.109 G > A, has been described with mild phenotypes, and may partially explain the increase in mild hearing loss detected on newborn screening. Consistent with the literature, the c.35delG variant was associated with more severe HL, while the c.101 T > C variant was associated with milder HL and U-shaped audiograms. This information provides a more complete picture of the phenotypic spectrum of GJB2/6 associated HL which provides short-term prognostic data and can inform pre- and post-natal counselling for individuals and families found to carry these variants.
Ascertainment in this study differs from most previously reported literature which genetically evaluated individuals being considered for cochlear implants i.e., typically severe levels of HL [30, 31]. In those studies, the most common variants were c.35delG and c.235delC which were identified in populations from European and Asian backgrounds, respectively. The c.109 G > A variant has been reported previously, especially from Asian ancestry cohorts [32], where the minor allele frequency is 0.08 [33]. Thus, it is unsurprising that it is prevalent in our agnostically ascertained cohort where the sensitive equipment used for universal newborn hearing screening and aABR (automated auditory evoked brainstem response) as a screening method can lead to capturing patients that may have mild, transient and/or fluctuating hearing profiles.
An artefact of newborn screening is the detection of mild hearing loss. As mild HL is being increasingly diagnosed at an earlier age [34], this presents prognostic and management uncertainty for both families [35] and clinicians [16]. This study provides evidence for a genetic basis for many mild HL cases adding to the emerging body of literature describing genotypes in mild and moderate HL cohorts [36, 37].
Prior publications have noted milder HL in association with either c.101 T > C or c.109 G > A alleles [38]. The pathogenic classifications of both variants were initially controversial, but an international consensus paper classified both as pathogenic with variable expressivity and incomplete penetrance [39]. Consistently, in this Australian cohort this variant is associated with a milder phenotype. This phenotypic information is valuable for clinicians and families presented with these results in infancy, prenatally or as part of reproductive carrier screening [40].
Previous research has shown that a heterozygous GJB2 variant is detected in 10-50% of individuals with HL [41], which can complicate and limit clinical interpretation and management. Additionally, some studies have indicated that carriers of certain variants have been reported to be more likely than ‘non-carriers’ to develop HL when exposed to other environmental factors or genetic defects [42]. In the current study, heterozygosity was identified in 37% of the cohort and the associated HL phenotype was highly variable ranging from normal (in the better ear) to profound. These findings align with previous publications [38] and may be due to (i) the GJB2 variant being coincidental, with HL secondary to variants in another NSHL gene, (ii) failure to detect a second, possibly intronic functionally significant variant in GJB2, (iii) the GJB2 variant modifies the expression of other variants in related HL genes or (iv) the GJB2 variant being coincidental and the HL stemming from a non-genetic aetiology. Comprehensive panel testing and/or whole genome sequencing may help identify the first two possibilities [43], and further research could possibly elucidate the third.
It is important to appreciate that classification of HL in this study is relative to the better hearing ear. Thus, our study detected individuals with normal hearing and asymmetric hearing loss where the hearing of the contralateral ear could range from mild to profound. The fact that genetic testing was offered in these cases implies that the HL was, at the time of testing, considered to be clinically indicated and/or socially significant to the individual or their families. While HL in some cases may have been complicated by transient, conductive overlay, the findings from the present study support that GJB2 variants can be associated with asymmetric HL [8]. The identification of these asymmetric cases (where one ear is classified as ‘normal’ hearing) may be reduced from this point forward given recommendations to only offer genetic testing in cases of bilateral HL [44]. However, a uniform and consistent approach to genetic testing for patients with NSHL is important to mitigate the risk of uncertain findings. Furthermore, this could potentially reduce the financial and psychological costs associated with inappropriate genetic testing.
The natural history in this cohort was predominantly stable but shows both improvements and progression over time. These findings are consistent with those previously reported in the literature [8, 45]. However, it should be noted that audiogram results become more accurate with increasing age in children, thus fluctuation/progression may reflect the young age of this cohort. Importantly, U-shaped HL was identified more frequently at subsequent time points than initial assessments and was associated with c.101 T > C. There is a paucity of literature on U-shaped (mid-frequency) HL, an uncommon audiometric finding, more commonly diagnosed in older individuals [46]. Although U-Shaped HL has not been formally associated with GJB2 generally and the c.101 T > C variant specifically, in reviewing previously published audiograms in c.101 T > C positive individuals [47], we identified cases of U-Shaped HL. This is clinically significant because this mid-frequency loss is associated with greater difficulty understanding speech in a noisy environment such as a classroom setting. Thus, children may function differentially in quiet and noisy environments, which could mask detection, thus increasing the risk of social problems and fatigue, especially if it is a deterioration [48].
Cumulatively, these results demonstrate a broad phenotypic association with GJB2 variants and some genotype-phenotype associations which can provide prognostic value. This data from a population wide cohort, provides prognostic information for preconception, prenatal and paediatric counselling of couples and families carrying these variants. For example, Freeman et al.’s [49] discussion of views regarding genetic testing for deafness in reproductive settings, highlighted that the recent American College of Medical Genetics and Genomics practice guidelines [40] recommended the inclusion of GJB2 variants in prenatal genetic screening on the basis of prevalence and NSHL being categorised as ‘moderately severe’ [50]. If such guidelines were adopted in Australia, the information in studies like this would be invaluable in counselling.
Strengths of this study include the agnostic mode of ascertainment which allowed for identification of a broad phenotypic spectrum. The centralisation of newborn screening, pathology and clinical data allowed for comprehensive phenotypic characterisation. Limitations include a finite sample size, which necessitated the grouping of moderately-severe, severe and profound HL in the analysis. We acknowledge that the impact on quality of life would be different between these groups. Other limitations include a lack of detailed data about other potentially contributing factors for HL and the fact that testing was limited to GJB2 coding variants and a single GJB6 deletion.
Future directions to further assist clinicians in providing genetic counselling in this area could include longer follow-up to clarify stability over time, broadening the phenotype to include developmental outcomes including speech and language development and response to intervention e.g., documenting outcomes of children who have required cochlear implants, and comprehensive panel testing for HL. Cumulatively, this information would provide clinicians and families with greater prognostic and management certainty at the time of diagnosis.
Conclusion
This study provides valuable insights for managing and counselling individuals with GJB2/GJB6 variants from a population health perspective. The phenotypic spectrum in biallelic individuals in this cohort is milder than has been previously reported, likely due to the agnostic ascertainment. Conversely, our study identified a portion of heterozygous carriers experienced hearing loss, which ranged from mild to moderate. The publication of the full spectrum of presentations offsets the prior publication of more severe presentations, which has potentially skewed the overall perception of the severity of the condition. Given the increasing interest in pre-conception carrier testing for deafness, larger cohort data is crucial to provide personalised, accurate genetic counselling.
References
Rouse SL, Florentine MM, Taketa E, Chan DK. Racial and ethnic disparities in genetic testing for hearing loss: a systematic review and synthesis. Hum Genet. 2022;141:485–94.
World Health Organisation. World report on hearing. Geneva; 2021.
Brewer CC, King KA. Genetic hearing loss: the audiologist’s perspective. Hum Genet. 2022;141:311–4.
Van Camp G, Willems PJ, Smith RJ. Nonsyndromic hearing impairment: unparalleled heterogeneity. Am J Hum Genet. 1997;60:758–64.
Van Camp G, Smith RJ. Hereditary Hearing Loss Homepage [updated 30 August 2021. Available from: https://omim.org/entry/220290.
Putcha GV, Bejjani BA, Bleoo S, Booker JK, Carey JC, Carson N, et al. A multicenter study of the frequency and distribution of GJB2 and GJB6 mutations in a large North American cohort. Genet Med. 2007;9:413–26.
DeMille D, Carlston CM, Tam OH, Palumbos JC, Stalker HJ, Mao R, et al. Three novel GJB2 (connexin 26) variants associated with autosomal dominant syndromic and nonsyndromic hearing loss. Am J Med Genet A. 2018;176:945–50.
Chan DK, Chang KW. GJB2-associated hearing loss: systematic review of worldwide prevalence, genotype, and auditory phenotype. Laryngoscope. 2014;124:E34–53.
Michalski N, Petit C. Central auditory deficits associated with genetic forms of peripheral deafness. Hum Genet. 2022;141:335–45.
Tsukada K, Nishio SY, Hattori M, Usami S. Ethnic-specific spectrum of GJB2 and SLC26A4 mutations: their origin and a literature review. Ann Otol Rhinol Laryngol. 2015;124:61S–76S.
Adadey SM, Wonkam-Tingang E, Twumasi Aboagye E, Nayo-Gyan DW, Boatemaa Ansong M, Quaye O, et al. Connexin Genes Variants Associated with Non-Syndromic Hearing Impairment: A Systematic Review of the Global Burden. Life (Basel). 2020;10.
Dahl H-HM, Ching TYC, Hutchison W, Hou S, Seeto M, Sjahalam-King J. Etiology and audiological outcomes at 3 years for 364 children in Australia. PLoS One. 2013;8:e59624.e.
Wilczewski CM, Obasohan J, Paschall JE, Zhang S, Singh S, Maxwell GL, et al. Genotype first: Clinical genomics research through a reverse phenotyping approach. Am J Hum Genet. 2023;110:3–12.
Ranola JMO, Tsai GJ, Shirts BH. Exploring the effect of ascertainment bias on genetic studies that use clinical pedigrees. Eur J Hum Genet. 2019;27:1800–7.
Kelsell DP, Dunlop J, Stevens HP, Lench NJ, Liang JN, Parry G, et al. Connexin 26 mutations in hereditary non-syndromic sensorineural deafness. Nature. 1997;387:80–3.
Ching TYC, Saetre-Turner M, Marnane V, Scarinci N, Choik C, Tulloch K, et al. Audiologists’ perspectives on management of mild bilateral hearing loss in infants and young children. Int J Audio. 2022;61:752–60.
Kirk EP, Ong R, Boggs K, Hardy T, Righetti S, Kamien B, et al. Gene selection for the Australian Reproductive Genetic Carrier Screening Project (“Mackenzie’s Mission”). Eur J Hum Genet. 2021;29:79–87.
Vears DF, Savulescu J, Christodoulou J, Wall M, Newson AJ. Are we ready for whole population genomic sequencing of asymptomatic newborns? Pharmgenom Pers Med. 2023;16:681–91.
Fitzgibbons EJ, Keszegi S, Driscoll C, Beswick R. Childhood hearing loss detected beyond the newborn screen. Int J Audio. 2023;62:278–85.
Au>stralian Bureau of Statistics. Cultural diversity: Census 2021 [cited 2022 Sep 23]. Available from: https://www.abs.gov.au/statistics/people/people-and-communities/cultural-diversity-census/2021.
Landrum MJ, Lee JM, Benson M, Brown GR, Chao C, Chitipiralla S, et al. ClinVar: improving access to variant interpretations and supporting evidence. Nucleic Acids Res. 2018;46:D1062–d7.
Azaiez H, Booth KT, Ephraim SS, Crone B, Black-Ziegelbein EA, Marini RJ, et al. Genomic landscape and mutational signatures of deafness-associated genes. Am J Hum Genet. 2018;103:484–97.
Kopanos C, Tsiolkas V, Kouris A, Chapple CE, Albarca Aguilera M, Meyer R, et al. VarSome: the human genomic variant search engine. Bioinformatics. 2018;35:1978–80.
Li MM, Tayoun AA, DiStefano M, Pandya A, Rehm HL, Robin NH, et al. Clinical evaluation and etiologic diagnosis of hearing loss: A clinical practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2022;24:1392–406.
Goodman A. Reference zero levels for pure tone audiometers. ASHA 1965;7:262–3.
Clark JG. Uses and abuses of hearing loss classification. ASHA 1981;23:493–500.
Guo C, Huang SS, Yuan YY, Zhou Y, Wang N, Kang DY, et al. Hearing phenotypes of patients with hearing loss homozygous for the GJB2 c.235delc Mutation. Neural Plast. 2020;2020:8841522.
Pittman AL, Stelmachowicz PG. Hearing loss in children and adults: audiometric configuration, asymmetry, and progression. Ear Hear. 2003;24:198–205.
Weegerink NJ, Pennings RJ, Huygen PL, Hoefsloot LH, Cremers CW, Kunst HP. Phenotypes of two Dutch DFNA3 families with mutations in GJB2. Ann Otol Rhinol Laryngol. 2011;120:191–7.
Popov TM, Stancheva I, Kachakova DL, Rangachev J, Konov D, Varbanova S, et al. Auditory outcome after cochlear implantation in patients with congenital nonsyndromic hearing loss: influence of the GJB2 status. Otol Neurotol. 2014;35:1361–5.
Sinnathuray AR, Toner JG, Clarke-Lyttle J, Geddis A, Patterson CC, Hughes AE. Connexin 26 (GJB2) gene-related deafness and speech intelligibility after cochlear implantation. Otol Neurotol. 2004;25:935–42.
Dahl HH, Tobin SE, Poulakis Z, Rickards FW, Xu X, Gillam L, et al. The contribution of GJB2 mutations to slight or mild hearing loss in Australian elementary school children. J Med Genet. 2006;43:850–5.
Chen S, Francioli LC, Goodrich JK, Collins RL, Kanai M, Wang Q, et al. A genome-wide mutational constraint map quantified from variation in 76,156 human genomes. bioRxiv. 2022:2022.03.20.485034.
McKay S, Gravel JS, Tharpe AM. Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss. Trends Amplif. 2008;12:43–54.
Lin JJ, Gillam L, Smith L, Carew P, King A, Ching TYC, et al. Mild matters: parental insights into the conundrums of managing mild congenital hearing loss. Int J Audio. 2022;61:500–6.
Kim BJ, Oh DY, Han JH, Oh J, Kim MY, Park HR, et al. Significant Mendelian genetic contribution to pediatric mild-to-moderate hearing loss and its comprehensive diagnostic approach. Genet Med. 2020;22:1119–28.
Markova T, Alekseeva N, Lalayants M, Ryzhkova O, Shatokhina O, Galeeva N, et al. Audiological evidence of frequent hereditary mild, moderate and moderate-to-severe hearing loss. J Pers Med. 2022;12:1843.
Kenna MA, Feldman HA, Neault MW, Frangulov A, Wu BL, Fligor B, et al. Audiologic phenotype and progression in GJB2 (Connexin 26) hearing loss. Arch Otolaryngol Head Neck Surg. 2010;136:81–7.
Shen J, Oza AM, Del Castillo I, Duzkale H, Matsunaga T, Pandya A, et al. Consensus interpretation of the p.Met34Thr and p.Val37Ile variants in GJB2 by the ClinGen Hearing Loss Expert Panel. Genet Med. 2019;21:2442–52.
Gregg AR, Aarabi M, Klugman S, Leach NT, Bashford MT, Goldwaser T, et al. Screening for autosomal recessive and X-linked conditions during pregnancy and preconception: a practice resource of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2021;23:1793–806.
Del Castillo I, Moreno-Pelayo MA, Del Castillo FJ, Brownstein Z, Marlin S, Adina Q, et al. Prevalence and evolutionary origins of the del(GJB6-D13S1830) mutation in the DFNB1 locus in hearing-impaired subjects: a multicenter study. Am J Hum Genet. 2003;73:1452–8.
Abdurehim Y, Lehmann A, Zeitouni AG. Predictive value of GJB2 mutation status for hearing outcomes of pediatric cochlear implantation. Otolaryngol Head Neck Surg. 2017;157:16–24.
Lin YH, Wu PC, Tsai CY, Lin YH, Lo MY, Hsu SJ, et al. Hearing Impairment with monoallelic GJB2 variants: A GJB2 cause or non-GJB2 cause? J Mol Diagn. 2021;23:1279–91.
Sung V, Downie L, Paxton GA, Liddle K, Birman CS, Chan WW, et al. Childhood Hearing Australasian Medical Professionals network: Consensus guidelines on investigation and clinical management of childhood hearing loss. J Paediatr Child Health. 2019;55:1013–22.
Del Castillo FJ, Del Castillo I. DFNB1 Non-syndromic Hearing Impairment: Diversity of mutations and associated phenotypes. Front Mol Neurosci. 2017;10:428.
Birkenbeuel J, Abouzari M, Goshtasbi K, Moshtaghi O, Sahyouni R, Moshtaghi A, et al. Characteristics of mid-frequency sensorineural hearing loss progression. Otol Neurotol. 2019;40:e497–e502.
Snoeckx RL, Huygen PL, Feldmann D, Marlin S, Denoyelle F, Waligora J, et al. GJB2 mutations and degree of hearing loss: a multicenter study. Am J Hum Genet. 2005;77:945–57.
Tharpe AM, Seewald R. Comprehensive Handbook of Pediatric Audiology. San Diego, UNITED STATES: Plural Publishing, Inc; 2016.
Freeman L, Righetti S, Delatycki MB, Scully JL, Kirk EP. The views of people with a lived experience of deafness and the general public regarding genetic testing for deafness in the reproductive setting: A systematic review. Genet Med. 2022;24:1803–13.
Lazarin GA, Hawthorne F, Collins NS, Platt EA, Evans EA, Haque IS. Systematic classification of disease severity for evaluation of expanded carrier screening panels. PLoS One. 2014;9:e114391.
Acknowledgements
The authors would like to acknowledge Ben Lundie, Chiyan Lau for help extracting genetic data, Megan Moore and Jane Fitzgibbons for help extracting audiological data and Ella McGahan for help with formatting and proof reading.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial or not-for profit sectors. Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
RK: literature review, extracted, collated and cleaned data, performed descriptive statistics, drafted initial manuscript and edited revisions. RB: provided advice on design and development of study, reviewed and revised manuscript. MTG: curated variant impact, reviewed and revised manuscript. AML: supervised variant analysis, revised and edited drafts. CD: edited the draft. KL: conceptualised and designed the study, extracted clinical data, performed descriptive statistics, reviewed and revised manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was conducted in full conformance with principles of the ‘Declaration of Helsinki’ Good Clinical Practice and was approved by the Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee (Protocol Number HREC/20/QCHQ/65404).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kriukelis, R., Gabbett, M.T., Beswick, R. et al. The congenital hearing phenotype in GJB2 in Queensland, Australia: V37I and mild hearing loss predominates. Eur J Hum Genet (2024). https://doi.org/10.1038/s41431-024-01584-0
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41431-024-01584-0
