
Abstract
The delivery of rapid genomic sequencing (rGS) to critically unwell children in intensive care occurs at a time of immense pressure and stress for parents. Contact with families after result disclosure, particularly after hospital discharge, presents an opportunity to meet their psychological, medical and information needs as they evolve. This study explores the preferences and perspectives of health professionals and parents of genetics follow up after rGS. Semi-structured interviews were conducted with 30 parents, seven genetic counsellors (GCs) and four intensive care physicians with experience in rGS. Transcripts were analysed using reflexive thematic analysis. Current practices surrounding genetics follow up after rGS were highly variable, resulting in some families not receiving the ongoing care they needed. Reasons identified by families for wanting follow-up care represented only a subset of those identified by health professionals. While GCs routinely provided their details to allow parents to initiate further contact, this was not always sufficient for follow-up care. Health professionals identified both organisational and psychosocial barriers to conducting follow up. As rGS transforms the diagnostic pathway in rare disease, there is a need for a co-designed, standardised but flexible model for follow-up care with genetics professionals so that families’ evolving needs are met.
Similar content being viewed by others

Introduction
Evidence for the clinical utility of rapid genomic sequencing (rGS) for critically unwell infants and children has been extensively reported [1,2,3,4,5]. This has triggered calls for rGS to be considered the standard of care in this context [2, 3, 6]. However, challenges remain to be addressed before this can be realised [3].
Our previous research [7, 8] along with other studies [9,10,11,12,13] have raised concerns about parents’ ability to make informed decisions in this highly stressful and time-pressured environment. Despite displaying low levels of decisional regret [10, 14], parents are cognizant of the way their heightened emotional state impacts their ability to make an informed decision about rGS [8]. Furthermore, we found some parents report making rushed and pressured decisions about rGS for their critically unwell child [8], suggesting there may be an increased need for additional information and psychosocial support at a later time. While we, and others, have previously highlighted the value of pre- and post-test genetic counselling as an integral part of delivering rGS in a way that supports the information and psychological needs of families [8, 9, 11,12,13], limited research has explored post-test counselling practices.
Meeting with families again post-results disclosure (a ‘follow-up appointment’) in the ambulatory setting, after the period of critical illness, presents an opportunity to address some of the potentially unmet needs of parents after rGS. However, practices and perspectives of health professionals surrounding rGS follow up are not well understood. Furthermore, parents’ experiences of – and need for – contact with genetic health professionals after rGS have also not been explored. This study therefore aimed to investigate the preferences and perspectives of health professionals (genetic counsellors representing genetic services, and intensive care physicians representing intensive care) and parents about follow up after rGS.
Materials and methods
Context
Implementation of rGS in the Australian neonatal and paediatric intensive care setting has been evaluated in a multi-site study by the Australia Genomics Health Alliance Acute Care Flagship, the protocol and clinical outcomes for which are described elsewhere [4]. Briefly, participants of the wider clinical study were critically unwell infants or children suspected of having a monogenic condition and their families. As part of their clinical care, families were offered trio exome sequencing, with results returned approximately three to five days after consent. The clinical procedure involved either a genetic counsellor (GC) or clinical geneticist (or both) conducting pre-test counselling with parents to facilitate decision making regarding testing. Similarly, a genetics health professional (GC or clinical geneticist) disclosed the result; in exceptional circumstances where a genetics health professional was not available, another health professional involved in the care of the patient (e.g., the intensivist) disclosed the result. The study protocol did not include any prescription for contact with families following results disclosure, irrespective of which health professional disclosed the result.
Participants
Parents
Methods for recruitment of parents for this study have been described elsewhere [8]. Briefly, inclusion criteria for were all parents of children who participated in the Acute Care Flagship study between March, 2018 and December, 2018. Families were excluded if the treating team deemed them not appropriate to contact, decided on a case-by-case basis.
Genetic counsellors
All 16 GCs who participated in a previous phase of the study (described elsewhere, [7]) consented to be recontacted for a second interview. Recruitment continued until all GCs previously interviewed were contacted.
Intensivists
All intensivists (paediatric intensive care clinicians and neonatologists) involved in the wider study were invited to participate in an interview via the clinical leads at each site. The total number of intensivists involved in the delivery of rGS in Australia was unknown at the time of the study, therefore recruitment continued until all clinical leads were contacted.
Data collection
Qualitative semi-structured interviews with health professionals were used to explore their practices and preferences for the delivery of rGS in intensive care, part of which centred on the provision of follow-up care; that is, contacting, speaking to, and/or meeting with the parents of their patients following results disclosure. Interviews with parents explored their experiences of the delivery of rGS for their critically unwell child, from pre-test counselling and consent, through results delivery and follow-up care.
All interviews were conducted by FL via telephone, videoconference, or in-person, using an interpreter where required. The interview guides are included as Supplementary Material. Results from earlier interviews with GCs and of parents’ experiences with decision making for rGS have been reported previously ([7] and [8], respectively).
Parent interviews were conducted with one or both parents, together or separately, depending on participant preference and availability. Interviews were audio-recorded and transcribed verbatim. For the interview involving an interpreter, only the English portions were transcribed (i.e., the interviewer and interpreter speaking). To maintain anonymity, pseudonyms were assigned to parents and children and numeric IDs assigned to health professionals.
Data analysis
Interviews were analysed concurrently with data collection using reflexive thematic analysis [15], involving familiarisation (becoming immersed in the data), generating codes (labelling sections of the transcript), constructing candidate themes (grouping codes and data into coherent themes), and revising and defining these themes through further coding and discussion. Initial codes were generated from topics in the interview guide and informed by the literature, with further codes generated inductively from transcripts. All transcripts were coded and discussed by FL and BM to ensure rigor, with themes reviewed and refined by FL, BM, AN and CG. Iterative data analysis was managed using NVivo 12 qualitative data analysis software [16].
In quotes presented in this paper, an ellipsis (…) reflects where a significant part of speech has been removed, and square brackets represent where a word has been replaced for clarity or to protect participant anonymity.
Results
Participant characteristics
Parents
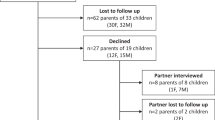
Twenty-three interviews with 30 parents of 20 patients were conducted between 10 and 21 months after rGS results disclosure. Participant characteristics have been described previously [8]. Important to note for the data presented in this paper, nine (45%) patients received a diagnostic rGS result, four (20%) received an uncertain result, and seven (35%) received no diagnosis from rGS. Fourteen (70%) families were from Victoria, three (15%) from Queensland and three (15%) from New South Wales. Fourteen (70%) children were alive at the time of interview. One child had been discharged prior to rGS results delivery.
Genetic counsellors
Seven of the 16 GCs who completed an interview in 2018 participated in a second interview in 2020. Reasons for not participating included: too busy (n = 2); on leave (n = 1); or had not continued to work in the intensive care setting (n = 6). The GCs interviewed represented a range of clinical experience, areas of genetic counselling practice, and locations across Australia (Table 1).
Intensivists
Four intensivists participated, working in either the neonatal intensive care unit (NICU) (n = 3, 75%) or paediatric intensive care unit (PICU) (n = 1, 25%). Three (75%) practiced in Victoria (at two different hospitals) and one (25%) in New South Wales. All were regularly involved in the delivery of rGS at their site.
Current follow-up practices
Health professionals’ current practices for following up families after rGS in intensive care are summarised in Table 2. Neither intensivists nor GCs reported any universal standard approach for follow up of patients after rGS, resulting in variation in practices between hospitals and individual clinicians.
Overwhelmingly, health professionals felt that follow up should be personalised to each individual family and their own unique circumstances, as well the clinical needs of the child.
“…follow up needs to be individualised to the patient and their family and what their needs are.” [Intensivist 2]
“I believe in that kind of individualised approach to everything…[because] it’s patient-centred care…” [GC 4, 11-20 rGS cases seen]
Parents’ reports of receiving follow up regarding their child’s rGS result (diagnostic, non-diagnostic or uncertain) were mixed; some parents had ongoing contact with the medical genetics team (clinical geneticist and/or GC) and multiple follow-up contacts, whereas others had not heard from the medical genetics team since results disclosure. None of the parents interviewed reported follow up with their intensive care team related to rGS, and there are appeared to be no pattern of follow up related to diagnostic outcome.
“We met with [the clinical geneticist and genetic counsellor] six months [after results disclosure]…” [Ayden, father of Alex, diagnosis]
“I had a couple of phone calls, and some emails, and [the clinical geneticist and genetic counsellor] talked us through that and gave us recommendations. They liaised with our GP, as well, to help him link in and know how to set up things up…” [Penny, mother of Parker, diagnosis, deceased]
“…there was no follow up, it was just ‘there’s nothing, sorry’…there was no information or data or follow up or anyone to contact around how we could find out further information or put anything in place for future testing.” [Natalie, mother of Nicholas, no diagnosis, deceased]
“Before [the] test also they spoke with us, then after test also they spoke with us. Then after that I haven’t seen any doctor of genetic testing.” [Odette, mother of Oliver, diagnosis]
The purposes of follow up are varied
Both intensivists and GCs identified a variety of reasons for meeting or talking with families again after the delivery of a result from rGS (Table 3).
Parents wanted further contact with their medical genetics team after receiving a result from rGS; reasons for this aligned with those information and medical needs identified by health professionals.
“…we had a lot more questions about certain things on our follow-up genetics appointment than we probably had for that first [meeting] …” [Astrid, mother of Alex, diagnosis]
“…because the other things are gradually coming into control, so for us it’s like ‘right, we want to know more, we want to know what the research is doing, we want to know what future treatment options look like’, all those sorts of things. Of more focus to us now.” [Logan, father of Lyla, uncertain result]
“…definitely follow up needs to happen, in any which way or form. You know, what happens next? Is that it? Do we never, do they never look at her DNA again or do they? Will they run her DNA again in six months’ time, 12 months’ time? Do we have to ask for the DNA to be run again? Who pays for that? Do we pay for that? Do the hospital pay for that? All these questions.” [Jenny, mother of Jessica, no diagnosis, deceased]
Initiating follow up
Some parents wanted to meet with the medical genetics team soon after results disclosure, whereas others wanted the ability to get back in contact on their own terms.
“…I probably would have liked another face-to-face appointment after we’d had a chance to process the information…” [Eleanor, mother of Edward, diagnosis]
“Even an email address that they can email later, a person that they can go back to and say ‘hey, can I have another meeting when you guys are free, I’ve got a whole heap of questions.’” [Kayla, mother of Kate, uncertain result]
Some GCs routinely provide their work contact details to families, allowing them to get in contact when they desired or felt necessary. This was either instead of or on top of follow up initiated by the medical genetics team.
“I think them having your number…so they can contact you and say ‘I’m freaking out, please call me’, [because] I have some families that do that repeatedly. That’s fine, and I call them back.” [GC 6, 100 + rGS cases seen]
“Generally the genetics team will have a standard, you know, book people in six months later or 12 months later for a review, but I think I’m finding a lot of people are contacting us earlier than that to sort of check in or talk about pregnancy planning in the future…” [GC 5, 21-50 rGS cases seen]
However, other GCs felt this alone was not appropriate; these GCs felt that families would be reluctant to contact them, and that they instead should be the ones to initiate follow-up contact.
“…it shouldn’t be the parents’ responsibility to initiate [follow up], because some would feel reluctant or wouldn’t know that they could.” [GC 2, 11-20 rGS cases seen]
“I think that if follow up isn’t offered, unless families…have questions hanging over them that they can’t get rid of, they’re unlikely to seek it out for themselves.” [GC 7, 11-20 rGS cases seen]
Parents also reflected on this practice; despite having the GC’s contact details, parents felt it was sometimes easier to look for information themselves online.
“[GC] did say that we could get in touch and ask any questions we have, but if you’ve got questions and you do reading you generally find the answers, so it wasn’t anything that I felt like I needed to write to [the GC] about immediately, or anything like that.” [Astrid, mother of Alex, diagnosis]
Additionally, some families – none of whom had received a diagnosis – were unclear how meeting with a GC following their child’s result would provide value.
“…even genetic counselling, I’m not even sure if, because if there’s no genetic component, how could that help?” [Kayla, mother of Kate, uncertain result]
“…with genetic counsellors, if there is no results, what can they help us with in the future?” [Jenny, mother of Jessica, no diagnosis, deceased]
Barriers to follow up
Genetic counsellors reported that barriers and challenges to delivering genetic counselling follow up after rGS included organisational and workplace barriers, as well as concerns for families’ emotional and social wellbeing (such as not wanting parents to feel harassed or distract from other support services) (Table 4).
Discussion
The delivery of rGS for critically unwell children in intensive care is a time of immense pressure and stress for parents, impacting their ability to make decisions and integrate complex information [8]. This study examines, for the first time, follow-up care after rGS (or any genetic testing) in intensive care. Our findings emphasize the importance of follow-up contact between families and their child’s medical genetics team in this context. Contact with families after rGS result disclosure presents an opportunity to address families’ evolving psychological, medical and information needs in the ambulatory setting. However, we demonstrated that current approaches to follow up cannot be relied on to meet parents’ needs, despite parents and health professionals having aligned intentions about, and goals for, follow up.
The need for genetics follow up after rGS
Despite the purported benefits of ongoing support following genetic testing in the paediatric outpatient setting [17], our data show that current practices, as reported by parents and health professionals, around follow up of children after rGS in intensive care are highly variable. Recent research in the Australian context suggests that practices for recontacting patients are also ad-hoc in other genetics subspecialties such as familial cancer, with most services relying on patients initiating recontact [18]. With no universal standard approach in place, some families do not receive the ongoing care they need.
It was the practice of some GCs in this study to leave responsibility with parents to contact them after rGS; while this was intended to be sensitive to differing family circumstances, it can leave parents with unmet needs. Additionally, it was evident that parents may not recognise that they could actively recontact their GC (instead of waiting to be recontacted) or were not aware of how it may help them – findings that mirror observations from a paediatric outpatient setting [19]. Reasons identified by families in this study for wanting further contact with their medical genetics team appear to align with many of the reasons identified by health professionals; however, some reasons for ongoing care identified by health professionals (such as the need for surveillance screening and psychosocial support) were not recognised by parents. This lack of understanding about both the opportunity and purpose of further contact with their medical genetics team means parents may be less likely to initiate such contact themselves.
Despite these barriers, research in the outpatient setting shows that patients value having access to a named person whom they can contact in their clinical genetics service following their appointment [20]. In contrast, our study showed that not all parents found that solely being given their health professional’s contact details was valuable, and that despite parents having their health professional’s contact details, they often did not initiate contact. This disparity in findings may suggest that, while parents want to be able to contact their clinical genetics service (or individual genetics health professional) when they are ready, some families may require their genetics health professional to be more proactive and initiate this connection.
Genetics follow-up after rGS should be standardised, but flexible
Despite the clear need for individualised care in this context, some parents reported not receiving any genetics follow-up care at all. Our findings from health professionals would suggest that this is because follow up is not standard for all families, rather than a failure of existing policy or procedure. To better support a family-centred approach to the delivery of rGS, it should be standard to offer follow-up care. Effective procedures and processes to address barriers to follow-up contact also need to be put in place. As rGS becomes more widely used and is initiated by a variety of medical specialists [21, 22], further consideration should be given to how and when to connect families with genetics health professionals.
This proposal presents a tension between the need to standardise procedures and the need to ensure that the approach is tailored to each individual child and family’s needs. A balance could be reached by implementing a minimum standard of care to ensure families receive – or are at least actively offered – follow up which is tailored to each family’s needs; for example, a phone call some weeks or months after results delivery to explore their needs at that time and offer an appointment then or in the future. This proposed minimum standard of care would provide a ‘safety net’ for families who would otherwise have had no follow-up support or arrangements put in place, whilst also supporting families who require a greater level of individualisation.
While this study provides evidence of a need for such an approach, further research is needed to establish its finer details. The role of the genetic counsellor in follow-up care after rGS is only just emerging. Different models of rGS in intensive care are being implemented around the world, with variation in the role genetics health professionals play. Irrespective of the model of delivery, follow-up genetics care should be carefully considered to meet the additional information needs that families may have following rGS. Particular attention should be paid to the care of families with a deceased child, and to those whose child remains in long-term inpatient care. Development of this model of care should utilise principles of co-design involving such key stakeholders, and its evaluation should stay attuned to the ever-evolving technology on which it is based.
Study limitations and further research
Clinical geneticists were not included in this study due to time and resource constraints so aspects of genetics follow-up care may not have been captured.
As interviews with parents occurred between 10 and 21 months post-rGS results disclosure, it is possible that some families either did not recall their follow-up care or had not yet attended a follow-up appointment with the genetics service.
Additionally, due to the geographic dispersion of families and health professionals, some families discussed healthcare teams who are not represented in this study, and families’ perceptions therefore do not necessarily reflect the health professionals interviewed.
This research took place within the Australian healthcare system. While findings are therefore not generalisable to experiences in other countries and healthcare settings, similar challenges and opportunities are likely to present themselves. Hospitals, health systems and countries yet to implement rGS in critical settings should therefore deliberately consider their plans for follow-up genetics care after testing, especially where clinical genetics services are not involved in pre- and post-test counselling.
The small number of health professionals recruited for this study means that data saturation was not reached and therefore the findings reported here may not be exhaustive of all perspectives of this population. Particularly, the small number and lack of geographical diversity of intensivists is a limitation of this study. However, the number of health professionals involved in the delivery of rGS in intensive care in Australia remains small, and therefore recruitment is inherently limited. As rGS becomes more widely adopted, further research investigating the perspectives of a greater number and variety of health professionals – including clinical geneticists and other medical specialists – would be beneficial.
Transcripts of interviews with non-English-speaking participants were only of the interpreter’s words. While this single interview did not raise different or additional perspectives to those conducted in English, further targeted research is needed to explore the experiences of those who are navigating rGS in an unfamiliar language. Inclusion of parents from a wide range of demographic circumstances will be critical for the co-design of standard-of-care follow up.
Conclusion
rGS transforms the diagnostic pathway in rare disease and follow-up genetics care is essential to meet the post-test psychological, medical and information needs of families. Current practices are variable and development and evaluation of a standardised model for follow up of families after rGS is desperately needed to guide health professionals and services. A model of care that remains flexible and sensitive to family needs is likely to best address this gap.
Though the need for genetics follow up may not be unique to rGS in acute care, the particular challenges of this setting make it an imperative. Furthermore, the ongoing implementation of rGS into intensive care settings around the world provides an opportunity to address this need concurrently with technology adoption. Co-design will be a critical step to ensure development and implementation of a model of care that addresses the specific challenges of this context.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
References
Dimmock D, Caylor S, Waldman B, Benson W, Ashburner C, Carmichael JL, et al. Project Baby Bear: Rapid precision care incorporating rWGS in 5 California children’s hospitals demonstrates improved clinical outcomes and reduced costs of care. Am J Hum Genet. 2021;108:1231–8.
Freed AS, Clowes Candadai SV, Sikes MC, Thies J, Byers HM, Dines JN, et al. The impact of rapid exome sequencing on medical management of critically ill children. J Pediatr. 2020;226:202–12.e1.
Kingsmore SF, Cakici JA, Clark MM, Gaughran M, Feddock M, Batalov S, et al. A randomized, controlled trial of the analytic and diagnostic performance of singleton and trio, rapid genome and exome sequencing in ill infants. Am J Hum Genet. 2019;105:719–33.
Australian Genomics Health Alliance Acute Care Flagship. Feasibility of ultra-rapid exome sequencing in critically ill infants and children with suspected monogenic conditions in the Australian public health care system. JAMA. 2020;323:2503–11.
Petrikin JE, Cakici JA, Clark MM, Willig LK, Sweeney NM, Farrow EG, et al. The NSIGHT1-randomized controlled trial: Rapid whole-genome sequencing for accelerated etiologic diagnosis in critically ill infants. NPJ Genom Med. 2018;3:6.
Stark Z, Ellard S. Rapid genomic testing for critically ill children: Time to become standard of care? Eur J Hum Genet. 2022;30:142–9.
Lynch F, Nisselle A, Gaff CL, McClaren B. Rapid acute care genomics: Challenges and opportunities for genetic counselors. J Gen Couns. 2021;30:30–41.
Lynch F, Nisselle A, Stark Z, Gaff CL, McClaren B. Parents’ experiences of decision making for rapid genomic sequencing in intensive care. Eur J Hum Genet. 2021;29:1804–10.
Ayres S, Gallacher L, Stark Z, Brett GR. Genetic counseling in pediatric acute care: Reflections on ultra‐rapid genomic diagnoses in neonates. J Gen Couns. 2019;28:273–82.
Brett GR, Martyn M, Lynch F, de Silva MG, Ayres S, Gallacher L, et al. Parental experiences of ultrarapid genomic testing for their critically unwell infants and children. Genet Med. 2020;22:1976–85.
Clowes Candadai SV, Sikes MC, Thies JM, Freed AS, Bennett JT. Rapid clinical exome sequencing in a pediatric ICU: Genetic counselor impacts and challenges. J Gen Couns. 2019;28:283–91.
Diamonstein CJ. Factors complicating the informed consent process for whole exome sequencing in neonatal and pediatic intensive care units. J Gen Couns. 2019;28:256–62.
Hill M, Hammond J, Lewis C, Mellis R, Clement E, Chitty LS. Delivering genome sequencing for rapid genetic diagnosis in critically ill children: Parent and professional views, experiences and challenges. Eur J Hum Genet. 2020;28:1529–40.
Cakici JA, Dimmock DP, Caylor SA, Gaughran M, Clarke C, Triplett C, et al. A prospective study of parental perceptions of rapid whole-genome and -exome sequencing among seriously ill infants. Am J Hum Genet. 2020;107:953–62.
Braun V, Clarke V, Hayfield N, Terry G. Thematic Analysis. In: Liamputtong P, editor. Handbook of Research Methods in Health Social Sciences. Singapore: Springer Singapore; 2019. p. 843–60.
QSR International Pty Ltd. NVivo qualitative data analysis software (released in March 2020). 2020. https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home.
Liang NSY, Adam S, Elliott AM, Siemens A, du Souich C, Study C, et al. After genomic testing results: Parents’ long-term views. J Gen Couns. 2022;31:82–95.
Vora BB, Mountain H, Nichols C, Schofield L. Opinions and experiences of recontacting patients: A survey of Australasian genetic health professionals. J Community Genet. 2022;13:193–9.
Ashtiani S, Makela N, Carrion P, Austin J. Parents’ experiences of receiving their child’s genetic diagnosis: A qualitative study to inform clinical genetics practice. Am J Med Genet. 2014;164:1496–502.
McAllister M, Payne K, MacLeod R, Nicholls S, Donnai D, Davies L. What process attributes of clinical genetics services could maximise patient benefits? Eur J Hum Genet. 2008;16:1467–76.
Franck LS, Kriz RM, Rego S, Garman K, Hobbs C, Dimmock D. Implementing rapid whole-genome sequencing in critical care: A qualitative study of facilitators and barriers to new technology adoption. J Pediatr. 2021;237:237–43 e2.
East KM, Cochran ME, Kelley WV, Greve V, Finnila CR, Coleman T, et al. Education and training of non-genetics providers on the return of genome sequencing results in a NICU setting. J Pers Med. 2022;12:405.
Acknowledgements
This study was completed in partial fulfilment of the requirements for the first author’s Doctor of Philosophy degree from the University of Melbourne. The authors thank the participants for their involvement.
Funding
This work was supported by the Victorian Government’s Operational Infrastructure Support Program and a grant from the Australian National Health & Medical Research Council (GNT1113531). FL was supported by a Melbourne Children’s Postgraduate Health Research Scholarship funded by the Royal Children’s Hospital Foundation, and by the Australian Government through the Medical Research Future Fund, as part of the Genomics Health Futures Mission (Grant number 76749). The Australian Genomics Health Alliance (Australian Genomics) project is funded by an NHMRC Targeted Call for Research grant (GNT1113531). The Acute Care Flagship project was also supported by a Royal Children’s Hospital Foundation grant (2017-906), and Sydney Children’s Hospital Network, Channel 7 Children’s Research Foundation Grant.
Author information
Authors and Affiliations
Contributions
FL contributed to the research design, recruited participants, performed and transcribed all interviews, coded all transcripts, and drafted the manuscript. BM and AN contributed to the research design, coded transcripts for concordance, and provided revisions to the manuscript. CG and ZS contributed to the research design and provided revisions to the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was reviewed and approved by the Human Research Ethics Committee of The University of Melbourne (HREC IDs 1646785.9 and 1853036). Participants provided voluntary, informed consent. The Australian Genomics Acute Care study received human research ethics committee approval from Melbourne Health (HREC/16/MH251).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lynch, F., Nisselle, A., Stark, Z. et al. Genetics follow up after rapid genomic sequencing in intensive care: current practices and recommendations for service delivery. Eur J Hum Genet 30, 1276–1282 (2022). https://doi.org/10.1038/s41431-022-01168-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41431-022-01168-w
This article is cited by
-
Rapid genomic testing in critically ill patients with genetic conditions: position statement by the Human Genetics Society of Australasia
European Journal of Human Genetics (2023)
-
2022: the year that was in the European Journal of Human Genetics
European Journal of Human Genetics (2023)
