
Abstract
Public engagement for Human Germline Genome Editing (HGGE) has often been called for, for example by the WHO. However, the impact of public engagement remains largely unknown. This study reports on public engagement outcomes in the context of a public dialogue project about HGGE in the Netherlands; the DNA-dialogue. The aim was to inquire opinions and opinion change regarding HGGE. A questionnaire was distributed on a national level (n = 2381) and a dialogue level (n = 414). The results indicate that the majority of the Dutch population agrees with the use of HGGE to prevent severe genetic diseases (68.6%), unlike the use to protect against infectious diseases (39.7%), or for enhancement (8.5%). No indications of change in these acceptance rates as a result of dialogue participation were found. The results did provide a tentative indication that participation in dialogue may lead to less negative opinions about HGGE (χ2(1) = 5.14, p = 0.023, OR = 0.56, 95% CI [0.34, 0.93]). While it was not a goal of the project to make people more accepting towards HGGE, this might be the effect of exposure to opinions that are less often heard in the global debate. We conclude that dialogue may lead to different outcomes for different people, depending on their characteristics and their entrance attitude, but does not appear to systematically direct people towards a certain opinion. The self-reported, impacts of dialogue participation included no impact, strengthening of opinion, enabling of forming a first opinion, more insight into the potential implications of HGGE, and a better understanding of other people’s perspectives.
Similar content being viewed by others

Introduction
The 2019 moratorium on heritable germline genome editing (HGGE) currently provides time, space, and momentum to engage the public and to be informed of their perspectives, while rules and regulations are still malleable [1,2,3,4]. From October 2019 to October 2020, a project called the ‘DNA-dialogue’ (www.dnadialoog.nl) organized twenty-seven dialogue meetings in The Netherlands for a variety of audiences, including healthcare professionals, lay public, and youth. Using animations of three different future scenarios of our society with(out) HGGE, ethical and social questions surrounding possible applications of HGGE were discussed [5]. More information on the DNA-dialogue project aims, methods, and the results of a qualitative observational study can be found in van Baalen et al. (2021) [6]. In this paper we report on the effects of public dialogue on opinion development.
The research within the DNA-dialogue project formed the first steps of a research for impact approach and consisted of a qualitative observational study [6], an online networks analysis [7], and a mixed methods questionnaire study. In case of disruptive technologies such as HGGE, the desired impact is to align the technology and its regulation with the needs and values of society [8]. This societal alignment requires engagement of the general public to identify their needs and values, allowing publics to inform future policy making regarding HGGE [9, 10].
Although the dialogue model of public engagement has been widely accepted as a science communication method that aims for mutual learning, impact evaluation is needed to refine practices and make them more evidence-based [11]. The dialogue model arose from criticism on the deficit model of public understanding, where science communication is an act of educating the public to make them more accepting of science. In the DNA-dialogue project, our aim was not to make people more accepting towards HGGE, but to stimulate opinion development. Given the deficit-dialogue history and the need for evidence-based science communication practices, we wanted to scientifically investigate the effects of public dialogue on acceptance and opinions.
To this end, we report on a selection of questions from the questionnaire, that provide insight into (change in): (1) acceptance of three different potential HGGE applications, (2) opinions about HGGE, and (3) self-reported impact of dialogue participation. Previous studies on HGGE opinions mainly focused on acceptance of various applications, showing a majority of positive attitudes towards applications for medical reasons and fatal diseases [12]. The current study replicated this approach and questioned participants’ opinions more openly to obtain a more general picture [13]. Previous studies evaluating the outcomes of dialogue participation are scarce. A study by Zorn, Roper [14] showed that dialogue on human biotechnology led to increased communicative self-efficacy, more mutual understanding among participants, and convergence of participants’ attitudes. The latter two may be the result of a realization among participants that the issue at hand is far more complex than originally thought [15].
Previously described methods to inquire public opinions and opinion change are respectively public opinion polling and deliberative polling. Whereas public opinion polling aims to measure the public’s perspectives regarding a topic at a single point in time, deliberative polling aims to measure how “raw public opinions” are transformed into “considered public opinions” after the public has deliberated on the topic [16, 17]. Aiming to inquire opinions and opinion change regarding HGGE, this study combined these methods, resulting in three different research settings which will be explained in the subjects and methods section below (see Table 1).
Subjects and methods
Study design and participants
Participants were included between August 2019 and January 2021. First, public opinion polling with two independent samples of the Dutch population aimed to show national opinions and opinion changes over the DNA-dialogue project timespan. Although we would not be able to link these changes to specific events, we were interested in overall trends in the complex system of opinion development about HGGE. In case of a major event that would alter the opinions of Dutch citizens at large, these samples could also serve as reference samples for those on a dialogue level. The first sample (S1) was recruited in August 2019, before the start of the project. The second sample (S2) was recruited in April 2020, when most physical dialogues had been held and the further progress became uncertain due to the Covid-19 pandemic. Secondly, repeated cross-sectional approach included independent responses of a first sample (S3) of people who signed up for dialogue participation or showed an interest in the project, and a second sample (S4) of people who had participated in one of the 27 dialogue meetings or a spin-off dialogue. Given the challenge of getting people to fill out two questionnaires, before and after dialogue, we decided to include these cross-sectional samples in our analyses while controlling for confounders. In this way, the cross-sectional approach still provides an indication of opinion change as a result of dialogue participation. Thirdly, deliberative polling included a single sample (S5) of participants who filled out our questionnaire both before and after they had participated in a dialogue meeting. Participants in S4 and S5 visited one of 15/27 dialogues or a spin-off dialogue.
Participants in deliberative polling and the repeated cross-sectional polling were recruited via e-mail either by an intermediary from the organization (e.g., a teacher at a high school, or a patient organization representative) or they could indicate their interest to participate by leaving their e-mail address upon registration for a DNA-dialogue meeting. Registration for the questionnaire was also available on the DNA-dialogue website and participants could scan a QR-code linking to the questionnaire on-site at several DNA-dialogue meetings. Participants in public opinion polling were recruited via the commercial research company Motivaction. Motivaction distributed the questionnaire among members of their StemPunt research panel (ISO certified; www.motivaction.nl/panel-stempunt). We included around 1200 participants in each sample (S1 and S2). Participants had to be between 18 and 75 years of age and panel members who had participated in S1 were excluded from invitation to S2. To reduce selection bias, Motivaction used regression analysis to determine propensity scores expressing their panel’s deviations from the Dutch population on sex, age, educational level, region, lifestyle and value measurements, and interactions between these characteristics. In determining these deviations, the Golden Standard of Statistics Netherlands and the (bi-)annual lifestyle and value measurements of Motivaction were used as a reference [18]. Underrepresented groups received a higher propensity score, thereby increasing the chance of being selected. Within cleaned samples (S1 and S2), remaining deviations from the Dutch population were reported, allowing weighting of the data to correct for these deviations. To further prevent selection bias, invitations to participate did not reveal any information about the content of the questionnaire. Active panel members receive points for each questionnaire they complete, which can be exchanged for gift cards or donations to charity. Motivaction acts in accordance with the General Data Protection Regulation. The StemPunt research panel is registered with the Dutch Data Protection Authority. Exclusion criteria for all samples can be found in Table 1 and are further elaborated on in the Supplementary Material.
Measures
This study focusses on a selection of questions, the complete questionnaire (in Dutch) can be found elsewhere (see the Supplementary Material for the link). For all participants (S1–5), the questionnaire included questions on demographic characteristics, acceptance of various applications of HGGE, and a question on participants’ opinions.
Demographics
The demographic characteristics we present here have previously been studied with regard to acceptability of gene therapy [12]. Categories of educational level––high, intermediate and low- were determined according to the standard of the Central Bureau for Statistics [19].
Acceptance of HGGE
Questions a-c below measured agreement with applications of HGGE on a 5-point scale (1 = Strongly disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly agree). Participants indicated to what degree they agreed with altering the DNA of an embryo in these scenarios:
(a) “Someone who wishes to have a child has a severe heritable muscle disease. For a future pregnancy, doctors can alter the DNA of an embryo, to prevent the child from inheriting the severe muscle disease. Assume the technology is safe and effective.”
(b) “Someone who wishes to have a child is healthy. For a future pregnancy, doctors can alter the DNA of an embryo, to protect the child against severe infection diseases, such as HIV. Assume the technology is safe and effective.”
(c) “Someone who wishes to have a child is healthy. For a future pregnancy, doctors can alter the DNA of an embryo, to increase the intelligence of the child. Assume the technology is safe and effective.”
Opinions about HGGE
Respondents were asked to describe what they thought about altering the DNA of embryos in max. three key words. The answers were clustered and categorized, resulting in five opinion groups: positive, negative, mixed (positive and negative), descriptive (positive nor negative), or indeterminable (no opinion was stated, e.g., “don’t know”, “no opinion”, “?”, or “-“. Two researchers (BV and DH) coded the answers independently, with good interrater reliability (κ = 0.80, p < 0.001). In case of disagreement, the researchers discussed until consensus was reached. This mostly concerned words that are given a value in public debate, but are neutral on their own, such as unnatural, innovative, preventive, and expensive. After discussion these words were considered descriptive.
Impact of participation
Participants in S4 and S5 were asked how their visit to a DNA-dialogue meeting had changed their perspective of HGGE.
The local Medical Ethical Committee (METC) exempted this study from the medical research involving human subjects act (WMO) (number: MEC-2019-0368).
Data analyses
Descriptive analyses were used for demographic characteristics, acceptance rates ((strongly) disagree, neutral, (strongly) agree) and categorized opinion rates (positive, negative, mixed, descriptive, indeterminable). Demographic characteristics were compared (S1–S2 and S3–S4) using Chi-square tests (Fisher’s Exact tests when the assumptions were not met). Propensity weighting as specified above was used on the most recent public opinion polling (S2) sample to obtain population estimates of acceptance and opinions rates. To evaluate changes in acceptance rates, public opinion polling and repeated cross-sectional data on acceptance (scale 1–5) were compared (S1–S2 and S3–S4) using independent t-tests, while deliberative polling (S5) data were compared using paired t-tests. To compare categorized opinions, dummy variables were created (e.g., positive yes = 1, no = 0) and Chi-square tests (Fisher’s Exact tests when the assumptions were not met) were used for the independent samples (S1–S2 and S3–S4), and McNemar tests for the paired samples (S5). Given that repeated cross sectional measures are prone to internal validity threats, analyses with adjusted samples were performed to rule out confounding demographic characteristics. Finally, the self-reported impact of dialogue participation on HGGE perspectives was analyzed using a thematic analysis. Initial themes were identified and coded by DH and subsequently checked by BV. IBM SPSS Statistics version 25.0 was used for data analyses and the significance level was set at 0.05, two sided.
Results
The five final sample sizes are depicted in Table 1.
Demographics
Table 2 shows the sample characteristics for S1–5. Age ranged from 15 to 91 years (both in S3). S2 public opinion polling respondents had significantly lower genetic knowledge than S1 respondents (χ2(2) = 14.16, p = 0.001). S3 and S4 cross-sectional respondents differed in age and educational level. S4 respondents were both more often younger than 24 years of age (χ2(7) = 65.12, p < 0.001) and had lower educational level (χ2(2) = 11.27, p = 0.004) than S3 respondents.
Acceptance of HGGE
Population estimates
Inspection of percentages of (dis)agreement with three HGGE applications in S2 revealed that germline modification for a severe muscular disease showed the highest acceptance rate (70.0%), followed by application for an infectious disease (39.0%) and application for intelligence (7.3%; see Fig. 1). Using propensity weighting, the acceptance of application for a severe muscular disease was estimated to be slightly lower in the Dutch population (68.6%), while the acceptance of application for an infectious disease and for intelligence was estimated to be slightly higher (respectively 39.7 and 8.5%) compared to S2 (see Fig. 1).

The three potential applications are: (1) to prevent a child from inheriting a severe muscular disease, (2) to protect against a severe infectious disease such as HIV, and (3) to increase intelligence. Percentages are depicted for the most recent public opinion poll (S2) and population estimates (calculated by means of propensity weighting).
Effect evaluation of the DNA-dialogue project
Secondly, the acceptance of these various applications was compared between S1 and S2, between S3 and S4, and within S5 (see Table 1 for sample descriptions). Mean acceptance scores and t-test results are depicted in Table 3. Between S1 and S2 and within S5, acceptance did not significantly differ. Acceptance of application for a severe muscular disease was slightly higher at S4 compared to S3 (t (197.67) = −2.27, p = 0.025). However, S4 had significantly lower age and educational level than S4, which can partially be explained by two groups of high school students (n = 22) that were included in S4, while there were no high school groups included in S3.
Ruling out the confounders
To correct for the difference in demographics in the two cross-sectional samples (S3 and S4), we performed a sensitivity analysis excluding the high school students in S4 (n = 22). Hereafter, the mean acceptance score for application for a severe muscular disease at S4 was 3.95 and significance disappeared (t (347) = −1.66, p = 0.098). Significant differences in demographic characteristics between S3 and S4 disappeared, while differences for other HGGE applications remained non-significant.
Opinions about HGGE
Population estimates
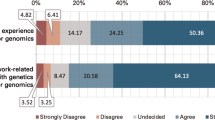
Opinions were coded as positive, negative, mixed (positive and negative), descriptive (positive nor negative) or indeterminable (no opinion was stated). Respondents with negative opinions were most frequent (37.8% in S2) while respondents with positive opinions were least frequent (8.9% in S2; see Fig. 2). Propensity weighing provides estimates for the Dutch population. Compared to S2, the estimated prevalence of mixed opinions was lower, while the estimated prevalence of descriptive and indeterminable opinions was higher (see Fig. 2).

Percentages are depicted for the most recent public opinion poll (S2) and the population estimate (calculated by means of propensity weighting).
Effect evaluation of the DNA-dialogue project
The distributions of opinions were compared between S1 and S2, between S3 and S4, and within S5 using Chi square and Fisher’s Exact tests for independent measures and McNemar tests for paired measures (see Table 4). We found significant differences between S1 and S2 and S3 and S4. Compared to S1, percentages of negative and mixed opinions were higher in S2 (respectively χ2(1) = 4.53, p = 0.033 and (χ2(1) = 4.79, p = 0.029), while percentages of positive and descriptive opinions were lower (respectively χ2(1) = 4.90, p = 0.027 and (χ2(1) = 7.35, p = 0.007). In S4, we found a lower proportion of negative opinions compared to S3 (χ2(1) = 5.14, p = 0.023, OR = 0.56, 95% CI [0.34, 0.93]). For the other opinion categories, differences were small and non-significant.
Ruling out the confounders
To correct for the demographical differences between S3 and S4, we performed a sensitivity analysis. The results remained significant in the sensitivity analysis excluding the high school students (a lower proportion of negative opinions in S4 compared to S3; χ2(1) = 4.69, p = 0.030). Differences between S3 and S4 for other opinions remained small and non-significant.
Self-reported outcomes of dialogue participation
Out of the 137 respondents who answered the questionnaire after taking part in a dialogue meeting, 97 respondents reported on the influence of dialogue participation on their perspective on HGGE. The other 40 participants visited a spin-off dialogue (n = 9) or filled out a pre-dialogue questionnaire while having already participated in a dialogue meeting (n = 31), and were not presented with this question. Out of the 97 people who responded, 41 (42.3%) people indicated that participation in a dialogue meeting had not changed their perspective on HGGE in any way. In the 56 (57.7%) remaining responses, the following themes were identified: opinions, awareness and knowledge, and insight into perspectives of others.
Opinions
Participants indicated that entering in dialogue had strengthened or confirmed their existing perspectives, changed their existing perspectives, or that it had helped them form an initial opinion. Opinions changed in multiple directions, towards being more positive, towards being more negative, and towards being more in doubt.
“Before I entered in dialogue, I didn’t know much about HGGE. I hadn’t really looked into it. The dialogue provided me with a clearer picture of what it means, and it allowed me to form my own opinion: use HGGE for diseases, but not to for example increase the strength of your child.”
“Before I was 100% against, but –dialogue participant- said something about monogenic disorders and this has opened the door a little.”
“My visit confirmed the opinion I already had.”
Awareness and knowledge
Participants indicated they had gained more knowledge, information, insight, and awareness. Some participants also indicated that entering in dialogue had resulted in realization of the complexity of the topic.
“I became more aware of the social and national implications of developments in science and the impact on individual autonomy.”
“My opinion hasn’t changed, but the dialogue did give me more insight into the societal and ethical issues.”
“My perspective hasn’t changed, but I did get more knowledge.”
Insight into perspectives of others
Finally, participants also indicated positive experiences with hearing perspectives of others. This broadened their own perspectives and increased their understanding of other people’s opinions.
“The dialogue gave me more insight and more understanding with regard to the opinions of others.”
“It was nice to hear other perspectives.”
“I found it very interesting to hear how various philosophies think about HGGE. I gained more insight into the arguments in favor and against held by other people.”
Discussion
Although public engagement for HGGE has often been called for [20,21,22,23], little had been initiated up until September 2019, when the Dutch DNA-dialogue project started organizing dialogue meetings [24]. In line with the new architecture for democratic debate on gene editing that Burall [25] proposed in Nature, the DNA-dialogue was organized by a large interdisciplinary consortium.
On a national level, we aimed to look at overall trends in the complex system of opinion development about HGGE. Compared to a previous study in 2016, acceptance of applications in our study (S2) was comparable for severe muscle disease (65.9% in the previous study, 68.6% in this study), but somewhat higher for a severe infectious disease (30.2% in the previous study, 39.7% in this study), and somewhat lower for intelligence (16.1% in the previous study, 8.5% in this study) [26]. These percentages should be interpreted carefully, as the underlying values and considerations remain unclear. Deliberation with the general public as well as with clinician groups and patients who live with severe genetic diseases, is necessary to provide insight into the severe genetic diseases for which the clinical need for and acceptance of HGGE are the highest, and why.
On a dialogue level, this study aimed to inquire changes in opinions about HGGE as a result of the Dutch DNA-dialogue project. In the light of the deficit-dialogue history and the need for evidence-based science communication practices, we aimed to find out whether dialogue led to more acceptance and/or whether it helped people develop their opinion. Regarding acceptance of HGGE applications, none of the samples showed changes after controlling for confounders. Regarding opinions about HGGE, we found no difference for deliberative polling and differences in public opinion polling were significant but relatively small and in opposite direction of the change in the cross-sectional samples. Here, fewer respondents who filled out the questionnaire after participating in dialogue showed negative opinions compared to respondents who filled out our questionnaire before participating in dialogue, also after controlling for possible confounders. Previous studies showed a positive influence of knowledge on attitudes towards general science and human genome editing [27, 28], thus the lower percentage of negative opinions might be explained by higher knowledge. However, other studies looked at genetically modified food and bioenergy and found greater knowledge to lead to more conflicting or strengthened rather than positive attitudes [29, 30].
Based on the self-reported impact of dialogue participation and the participant testimonials that were shared with the researchers after dialogue meetings, the lower percentage of negative opinions might also be the effect of exposure to opinions and arguments that are less often heard in the global debate which often focusses on designer babies, eugenics, and playing God. Participants reported that dialogue participation increased their knowledge and awareness and provided them with a better image and understanding of the arguments and opinions held by others. However, other participants also indicated that the dialogue had not influenced their perspective or that it had confirmed them in the opinion or beliefs they already had, the latter of which may have led to more attitude strength as described in previous literature [29, 31].
Strengths and limitations
An important strength of this study is that by means of propensity sampling and propensity weighing, we were able to estimate acceptance of various HGGE applications and opinions about HGGE in the Dutch population. Such results that are representative for the population can be challenging to obtain when it comes to complex topics such as HGGE. Another strength is that participants in this study were engaged at various levels. This has enabled a balance between political equality and deliberation [32]; the public opinion polls increased the reach of the DNA-dialogue project and allowed more people to inform future policy making regarding HGGE, while the DNA-dialogue meetings stimulated deliberation.
Limitations of this study include the small number of respondents in deliberative polling (n = 40). This research setting required respondents to participate in a dialogue meeting and fill out the questionnaire both before and after this dialogue meeting. Respondents may have been reluctant to fill out the questionnaire, especially for a second time, given the lengthy questionnaire that was used. Participants were therefore not given a time limit to fill out the questionnaire after a dialogue meeting. Furthermore, sampling for cross sectional polling and deliberative polling was convenience-based and resulted in selection biases. Cross-sectional polling was in addition limited by the (apparent) differences in demographics between S3 and S4. The educational scale we used had a range from 1 to 8, which was converted to low (1–3), intermediate (4–6), and high (7 and 8). A number of high school students who participated in S4 scored 3 on this scale, placing them in the low educational level category, even though they were following high school education on the highest and second highest level. To minimize actual confounding factors, future studies that evaluate the outcomes of dialogue participation should use a within-subjects design or match the characteristics of participants in the samples that are being compared. To further prevent selection biases, future studies should aim for representivity among research participants. To this end, it should be made as easy and attractive as possible for participants to fill out the questionnaire both before and after dialogue, for example with very short questionnaires that can be filled out on-site and by using incentives for completed questionnaires.
Conclusion
Although the results provided a tentative indication that participation in dialogue may lead to less negative opinions about HGGE, we found no indications of participants in dialogue meetings being systematically directed towards or convinced of a certain opinion. Self-reported impacts of dialogue participation included no impact, strengthening of opinion, enabling of forming a first opinion, more insight into the potential implications of HGGE, and a better understanding of other people’s perspectives. Thus, at the very least, dialogue makes participants aware of their own perspective, and in many cases allows the participants to acquire a larger context of their own perspectives in relation to those of others. Keeping the goal of societal alignment in mind, dialogue may contribute to identifying the needs and values of the public since they become more aware of these themselves, leading to better informed decisions. At the same time, being able to place one’s own perspective in the context of others’ may contribute to more support for future decisions.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
07 September 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41431-022-01176-w
References
Lander ES, Baylis F, Zhang F, Charpentier E, Berg P, Bourgain C. et al. Adopt a moratorium on heritable genome editing. Nature. 2019;567:165–8.
Collins FS. NIH supports international moratorium on clinical application of germline editing: National Institutes of Health; 2019 [updated 13-03-2019. Available from: https://www.nih.gov/about-nih/who-we-are/nih-director/statements/nih-supports-international-moratorium-clinical-application-germline-editing.
ESHRE. Moratorium on Gene Editing in human embryos: European Society of Human Reproductioin and Embryology; 2019. Available from: https://www.eshre.eu/Press-Room/ESHRE-News/2019.
ESHG. Response to ‘Adopt a moratorium on heritable gene editing’: The European Society of Human Genetics; 2019 [updated 27-03-2019. Available from: https://www.eshg.org/index.php?id=910&tx_news_pi1%5Bnews%5D=16&tx_news_pi1%5Bcontroller%5D=News&tx_news_pi1%5Baction%5D=detail&cHash=50d16c4b8e5abef5e2693e7864b7e2e5.
van Baalen S, Gouman J, Verhoef P Discussing the modification of heritable DNA in embryo’s. Rathenau Institute; 2020.
van Baalen S, Gouman J, Houtman D, Vijlbrief B, Riedijk S, Verhoef P. The DNA-dialogue: a broad societal dialogue about human germline genome editing in the Netherlands. The CRISPR J. 2021;4:616–25.
Lutkenhaus RO, Jansz J, Bouman MPA. Stimulating conversations about human germline technology. In: Lutkenhaus RO (ed). Entertainment-Education in the New Media Landscape: Stimulating Creative Engagement in Online Communities for Social and Behavioral Change. Erasmus Research Centre for Media, Communication and Culture, Rotterdam, 2020. pp 88–119.
Ribeiro B, Bengtsson L, Benneworth P, Bührer S, Castro-Martínez E, Hansen M, et al. Introducing the dilemma of societal alignment for inclusive and responsible research and innovation. J Responsible Innov. 2018;5:316–31.
Andorno R, Baylis F, Darnovsky M, Dickenson D, Haker H, Hasson K, et al. Geneva statement on heritable human genome editing: the need for course correction. Trends in Biotechnol. 2020.
Dryzek JS, Nicol D, Niemeyer S, Pemberton S, Curato N, Bächtiger A. et al. Global citizen deliberation on genome editing. Science. 2020;369:1435–7.
Gerber A, Jensen E. For science communication to be effective it should be evidence based. In: Impact of Soc Sci Blog. The London school of economics and political science. 2020. https://blogs.lse.ac.uk/impactofsocialsciences/2020/05/27/for-science-communication-to-be-effective-it-should-be-evidence-based/. Accessed 10 May 2022.
Delhove J, Osenk I, Prichard I, Donnelley M. Public acceptability of gene therapy and gene editing for human use: a systematic review. Hum Gene Ther. 2020;31:20–46.
Howell EL, Yang S, Beets B, Brossard D, Scheufele DA, Xenos MA. What Do We (Not) Know About Global Views of Human Gene Editing? Insights and Blind Spots in the CRISPR Era. CRISPR. J. 2020;3:148–55.
Zorn TE, Roper J, Weaver CK, Rigby C. Influence in science dialogue: Individual attitude changes as a result of dialogue between laypersons and scientists. Public Underst Sci. 2012;21:848–64.
Escobar O. Public dialogue and deliberation: a communication perspective for public engagement practitioners. Edinburgh: UK Beacons for Public Engagement. 2011.
Fishkin JS Deliberative polling. The Oxford handbook of deliberative democracy: Oxford University Press; 2018. 314-28.
Hendriks F. Democratic innovation beyond deliberative reflection: the plebiscitary rebound and the advent of action-oriented democracy. Democratization. 2019;26:444–64.
Spangenberg F, Lampert M. De grenzeloze generatie: en de eeuwige jeugd van hun opvoeders: Nieuw Amsterdam; 2013.
Standaard Onderwijsindeling (SOI): Centraal Bureau voor de Statistiek. Available from: https://www.cbs.nl/nl-nl/onze-diensten/methoden/classificaties/onderwijs-en-beroepen/standaard-onderwijsindeling--soi--.
Baylis F. Human germline genome editing and broad societal consensus. Nat Hum Behav. 2017;1:1–3.
Jasanoff S, Hurlbut JB, Saha K. Democratic governance of human germline genome editing. CRISPR J. 2019;2:266–71.
Sarewitz D. CRISPR: science can’t solve it. Nature 2015;522:413–4.
Jasanoff S, Hurlbut JB, Saha K. CRISPR democracy: gene editing and the need for inclusive deliberation. Issues Sci Technol. 2015;32:37.
Vijlbrief B, Riedijk S, Houtman D, Hofstra R Germline genome editing: public dialogue is urgent but not self-evident. Eur J Hum Genet. 2020;28:1–2.
Burall S. Rethink public engagement for gene editing. Nature. 2018;555:438–9.
Hendriks S, Giesbertz NAA, Bredenoord AL, Repping S. Reasons for being in favour of or against genome modification: a survey of the Dutch general public. Hum Reprod Open. 2018;2018:hoy008.
Allum N, Sturgis P, Tabourazi D, Brunton-Smith I. Science knowledge and attitudes across cultures: a meta-analysis. Public Underst Sci. 2008;17:35–54.
Scheufele DA, Xenos MA, Howell EL, Rose KM, Brossard D, Hardy BW. US attitudes on human genome editing. Science. 2017;357:553–4.
Van Dael M, Lizin S, Swinnen G, Van Passel S. Young people’s acceptance of bioenergy and the influence of attitude strength on information provision. Renew energy. 2017;107:417–30.
Durant RF, Legge JS Jr. Public opinion, risk perceptions, and genetically modified food regulatory policy: reassessing the calculus of dissent among European citizens. Eur Union Politics. 2005;6:181–200.
Drummond C, Fischhoff B. Individuals with greater science literacy and education have more polarized beliefs on controversial science topics. Proc Natl Acad Sci. 2017;114:9587–92.
Fishkin JS, Luskin RC. Experimenting with a democratic ideal: deliberative polling and public opinion. Acta politica. 2005;40:284–98.
Acknowledgements
We would like to thank our partners of the DNA-dialogue project consortium for fruitful discussions about this research and for facilitating the distribution of our questionnaire.
Funding
The Dutch DNA-dialogue was an independent bottom-up initiative of 11 organizations from the Netherlands, including patient representative groups, academic departments in clinical genetics and reproductive medicine, professional associations, a technology assessment institute, the National Institute for Public Health and the Environment, a science communication organization, and the Dutch National Information Center on Heredity. These organizations wrote a project proposal titled “A public dialogue on germline genome editing”. The Dutch Ministry of Health, Welfare, and Sport financed this project but was in no way involved in the design and organization of the dialogues, the collection, and analysis of the data, or the reporting of the results.
Author information
Authors and Affiliations
Contributions
SR, MP, PV, and DH contributed to study concept and design. SR, BV, and DH conducted the study and gathered data of this manuscript. DH and MP performed the statistical analysis. All authors were involved in the interpretation of the study results, as well as the drafting and revision of the manuscript, and all approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The local Medical Ethical Committee (METC) exempted this study from the medical research involving human subjects act (WMO) (number: MEC-2019–0368).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Houtman, D., Vijlbrief, B., Polak, M. et al. Changes in opinions about human germline gene editing as a result of the Dutch DNA-dialogue project. Eur J Hum Genet 31, 409–416 (2023). https://doi.org/10.1038/s41431-022-01114-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41431-022-01114-w
This article is cited by
-
“What if” should precede “whether” and “how” in the social conversation around human germline gene editing
Journal of Community Genetics (2023)
-
Stakeholder Involvement in the Governance of Human Genome Editing in Japan
Asian Bioethics Review (2023)
-
The Duty to Edit the Human Germline
Res Publica (2023)
