
Abstract
X-linked Alport syndrome (XLAS) is an inherited renal disease caused by mutations in COL4A5 gene. The c.2858G>T(p.(G953V)) in COL4A5 gene (rs78972735) has been considered pathogenic previously. However, there are conflicting interpretations of its pathogenicity recently. Here we presented 19 Chinese families, out of which 36 individuals (18 probands and 18 family members) carried the c.2858G>T(p.(G953V)) in COL4A5 gene. The clinical manifestations and genetic findings of them were analyzed. We found there were no clinical features of Alport syndrome not only in six probands with c.2858G>T(p.(G953V)) in COL4A5 plus pathogenic variants in other genes (e.g., WT1, ADCK4, NPHP1, TRPC6, COL4A4, and PAX2) but also in another six probands with only the c.2858G>T(p.(G953V)) variant. The other six probands with a combination of c.2858G>T(p.(G953V)) and another pathogenic variant in COL4A5 had XLAS. Eleven family members (11/18, nine females and two males) who had only the c.2858G>T(p.(G953V)) variant were asymptomatic. These two males (at age of 42 and 35 years) had normal result of urine analysis and no more clinical traits of Alport syndrome. We conclude c.2858G>T(p.(G953V)) in COL4A5 gene is not a pathogenic variant for XLAS. Individuals should not be diagnosed as XLAS only based on the detection of c.2858G>T(p.(G953V)) in COL4A5 gene.
Similar content being viewed by others

Introduction
Alport syndrome (AS) is an inherited renal disease characterized by hematuria, proteinuria, and progressive renal failure, variably associated with hearing loss and ocular abnormalities [1,2,3]. It is caused by mutations in the COL4A3, COL4A4, or COL4A5 genes encoding α3, α4, and α5 chains of collagen type IV, a component of the glomerular basement membrane (GBM) in the kidney [4, 5]. Eighty-five percent of families have X-linked Alport syndrome (XLAS) with mutations in COL4A5 gene [6, 7]. It is well known that male patients with XLAS, who are hemizygous for mutations in COL4A5 gene, are severely affected [8, 9]. All of the males have microscopic hematuria and 90% of them progress to end-stage renal disease (ESRD) before age 40 years [9,10,11,12].
Up to now, 1000 mutations in COL4A5 gene have been included in the Human Gene Mutation Database (HGMD) and about 36% of them are glycine substitutions. Glycine substitutions in the collagenous domain of the α5 (IV) chain are usually considered pathogenic, since glycine is the smallest amino acid and it is critical for the formation of the triple helical structure [13, 14]. However, many variants have quite limited evidence for pathogenicity assessment. With the wide application of next generation sequencing (NGS), more and more variations in COL4A5 gene are found and the relationship of genotype and phenotype are analyzed [15, 16]. Therefore, the assessments of pathogenicity are important and would be corrected over time.
The c.2858G>T(p.(G953V)) in COL4A5 gene (rs78972735) is considered pathogenic in the HGMD database, while it is considered conflicting of pathogenicity in the ClinVar database [17,18,19,20]. In addition, it is more common in Asian population, in whom the allele frequency ranges from 0.01 to 0.03. In this study, we report 19 families from China with the variant of c.2858G>T(p.(G953V)) in COL4A5 gene and their clinical manifestations, providing more evidence to assess its pathogenicity.
Subjects and methods
Patients and families
We selected patients from the online registry database of hereditary kidney diseases in children in China (https://www.nrdrs.org.cn/app/rare/), according to the following two criteria (1) cases with gene mutations tested by targeted NGS; (2) cases with the variant of c.2858G>T(p.(G953V)) in COL4A5 gene. Cases without clinical data were excluded. And all their family members in the registry database were included. The clinical data including gender, age, renal and extrarenal manifestations, and renal histopathology results were collected. The Ethical Committee of Peking University First Hospital approved the project, and informed consent was obtained from the probands and their family members.
Targeted NGS and data analysis
Genomic DNA was isolated from the blood samples using a FlexiGene DNA Kit (Qiagen) according to the manufacturer’s protocol. Genomic DNA from probands was detected for pathogenic variants with targeted NGS (No.DX0595, including 464 genes related to inherited kidney disease) by BGI in China. Data were filtered with the variant databases, such as dbSNP (https://www.ncbi.nlm.nih.gov/projects/SNP/), the 1000 Genomes Project (ftp://ftp-trace.ncbi.nih.gov/1000genomes/ftp/release), and Exome Aggregation Consortium (ExAC) (http://exac.broadinstitute.org/). The allele frequency of the candidate variants were considered to be <5% in these databases. The functional significance of unpublished variants was predicted using SIFT, PolyPhen 2, and Mutation Taster. The evolutionary conservation of the variant sites was evaluated using the PhyloP Primates tool. Splice site effect prediction was performed using Human Splicing Finder (Version 3.1) [21]. The pathogenicity of variants identified was classified according to the ACMG standards and guidelines [22]. If the following criteria were met including truncating mutations (nonsense, consensus splice site ± 1 or 2 nucleotide, large deletion, and frameshift) or novel missense variants in domain of high evolutionary conservation and more than two prediction scores classified the allele as disease causing (SIFT, Mutation Taster, Polyphen 2), the variant was ascertained to be a pathogenic variant. All the variants data has been submitted to ClinVar (Submission ID: SUB6246401; Organization ID: 505424).
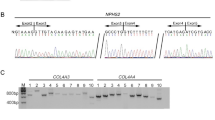
Sanger sequencing or real-time quantitative PCR (qPCR) was used to confirm candidate pathogenic variants identified with NGS in probands. Genomic DNA from family members was analyzed by Sanger sequencing or qPCR to determine whether they had the same pathogenic variants as the probands.
Results
Nineteen different Chinese families (51 individuals) were enrolled in this study, out of which 36 individuals carried the c.2858G>T(p.(G953V)) in COL4A5 gene. The clinical features and genetic results of the individuals enrolled in this study were shown in Table 1.
The 19 families were divided into three groups according to their genetic findings
Group 1: families with the c.2858G>T(p.(G953V)) variant plus pathogenic variants in other genes
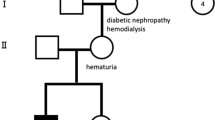
There were seven families in group 1 (family number 1–7). The proband from family 1, a 10-year-old girl with ESRD, had a younger sister who died at age of 7 years due to ESRD. Both of the two sisters had focal segmental glomerulosclerosis (FSGS). Genetic test of the proband revealed compound heterozygous variants in ADCK4 gene and the c.2858G>T(p.(G953V)) variant. And her parents were asymptomatic heterozygous carriers of the variants in ADCK4. The probands from two families (family number 3 and 6), both of them were female, presented with renal failure at an early age, identified with pathogenic variants in TRPC6 gene and NPHP1 gene respectively, in addition to the c.2858G>T(p.(G953V)) variant. Another two probands (family number 4 and 5) presented with hypospadia and microphthalmus, respectively. Genetic test found de novo pathogenic variants in WT gene and PAX2 gene in these two probands, respectively, besides the c.2858G>T(p.(G953V)) variant inherited from their mothers. The proband from family 7 presented with hematuria at age of 3 years, with a positive family history of hematuria in her mother. Genetic test found a heterozygous nonsense variant in COL4A4 gene and the c.2858G>T(p.(G953V)) variant in both the proband and her mother. The last proband (family number 2) in group 1 was diagnosed with congenital nephrotic syndrome (CNS) at age of 1 month after birth. The mother and father undertook genetic test because the DNA sample was not available for proband 2. Genetic test found the parents were heterozygous carriers of the pathogenic variants in NPHS1. Moreover, the mother had the c.2858G>T(p.(G953V)) variant but she was asymptomatic.
Group 2: families with the c.2858G>T(p.(G953V)) variant plus another pathogenic variant in COL4A5 gene
There were six families in group 2 (family number 8–13). All of the six probands in this group presented with hematuria and proteinuria. One of the proband from family 13 presented with hearing loss at age of 14 years. Five of the probands underwent renal biopsy, and four had typical GBM changes of AS. Five of the mothers had hematuria with or without proteinuria, except the mother from family 9. Genetic test found a pathogenic variant in COL4A5 gene and the c.2858G>T(p.(G953V)) variant in each of the six probands. Both of the two variants in COL4A5 gene in five probands (except proband 9) were inherited from their mothers. It was proved the pathogenic variant c.937-2A>C in proband 9 was de novo, and the c.2858G>T(p.(G953V)) variant was inherited from her mother.
Group 3: families with only the c.2858G>T(p.(G953V)) variant
There were six families in group 3 (family number 14–19). Three of the probands in this group presented with steroid resistant nephrotic syndrome. The onset age of nephrotic syndrome in these three probands was 1.5, 4, and 6 years, respectively. The result of kidney biopsy in these three probands was FSGS and mesangial proliferative glomerulonephritis (MsPGN) without anomalies of GBM. Two of the probands presented with ESRD at age of 9 and 5 years, respectively. The proband from family 14 presented with steroid sensitive nephrotic syndrome at age of 2 years. All these six probands had no hematuria and no family history of kidney diseases. Genetic test found the c.2858G>T(p.(G953V)) variant in COL4A5 gene in all these six probands. The c.2858G>T(p.(G953V)) variant was inherited from their mothers in five of the probands except proband 19, who inherited this variant from her healthy father.
Clinical features of the family members with the c.2858G>T(p.(G953V)) variant
There were 18 family members identified with the c.2858G>T(p.(G953V)) variant in this study. They were 2 males and 16 females. In the male group, they were two fathers (family number 6 and 19) with normal result of urine analysis at age of 42 and 35 years, respectively. And both of the two fathers had no extrarenal manifestations. In the female group, in addition to the heterozygous c.2858G>T(p.(G953V)) variant, a heterozygous pathogenic variant of COL4A5 gene was found in five of them (5/16) and a heterozygous pathogenic variant of COL4A4 gene was found in one of them (1/16). These six females presented with hematuria with or without proteinuria at age of 24–44 years and with normal renal function. Another female identified with a heterozygous p.(Tyr1009*) variant in NPHS1 gene and the heterozygous c.2858G>T(p.(G953V)) variant in COL4A5 was asymptomatic. The other nine females who had the heterozygous c.2858G>T(p.(G953V)) variant were all asymptomatic at age of 20–47 years. And the clinical features of the individuals with only c.2858G>T(p.(G953V)) variant in COL4A5 gene were shown separately in Table 2.
Gene analysis
Fifteen pathogenic variants were detected in the 19 families in this study besides the c.2858G>T(p.(G953V)) variant (Table 3). Seven of them (7/15) were novel pathogenic variants: one in NPHS1 gene c.144dup (p.(Val49Serfs*43)), one in TRPC6 gene c.335C>T (p.(Pro112Leu)), one in PAX2 gene c.418C>T (p.(Arg140Trp)), and four in COL4A5 gene c.937-2A>C, c.1813_1814dup (p.(Gly606Leufs*13)), c.4024G>T (p.(Gly1342*)), and c.4510delG (p.(Ala1504Profs*50)). The variant c.81G>A (p.(Ala27=)) in COL4A5 was not found in 1000G and ExAC. The mutation Taster predicted it as disease causing. The c.81G>A occurs in the last base pair of exon 1 of COL4A5. Human Splicing Finder predicted it as broken WT donor site and most probably affecting splicing. The c.2858G>T(p.(G953V)) variant (rs78972735) in COL4A5 gene had a high allele frequency of 0.01 in the 1000G Asian populations. It was included in the ClinVar, HGMD, and LOVD database. The mutation Taster predicted the c.2858G>T(p.(G953V)) variant as polymorphism, while Polyphen 2 and SIFT scored it as damaging.
Discussion
In this study, we reported 19 Chinese families with the c.2858G>T(p.(G953V)) variant in COL4A5 gene. By analyzing the clinical manifestations of 36 individuals (18 probands and 18 family members) who carried the c.2858G>T(p.(G953V)) variant, we found the c.2858G>T(p.(G953V)) variant in COL4A5 gene was not a pathogenic variant resulting XLAS.
The 19 families enrolled in this study were divided into three groups for analysis. We found probands in group 1 and group 3 presented mainly with early onset of renal failure (median age of 9 years) or nephrotic syndrome. The proband from family 14 in group 3 presented steroid sensitive nephrotic syndrome without hematuria and got complete remission after treatment. In addition, the available renal biopsies of the probands in these two groups were FSGS or MsPGN without abnormal changes of GBM. And the majority of the families in these two groups had no family history of hematuria and had no hearing loss or typical ocular lesions for AS [23, 24]. Apparently the probands in group 1 and group 3 should not be diagnosed as XLAS even all of them had the c.2858G>T(p.(G953V)) variant in COL4A5 gene. Moreover, eleven (nine females and two males) of the family members who had only the c.2858G>T(p.(G953V)) variant were asymptomatic. The two males (at age of 42 and 35 years) had normal result of urine analysis and no more clinical traits of AS. This strongly suggested that the c.2858G>T(p.(G953V)) variant in COL4A5 gene was not a pathogenic variant for XLAS. In a recently report [19] of a family with polycystic kidney disease, the c.2858G>T(p.(G953V)) variant in COL4A5 gene was identified in four individuals who had no clinical features of AS, which supported our findings.
Totally 11 female and 6 male individuals with only c.2858G>T(p.(G953V)) variant in COL4A5 gene were included in this study. Two of the 11 females, of the youngest ages, developed ESRD at 9-year old and steroid resistance nephrotic syndrome at 6-year old, respectively. And the other nine females aged from 20 to 47 years old had normal urinary analysis. This is different from the natural history of female patients with XLAS. It has been reported that hematuria, usually microscopic, presented in 96% of females with XLAS and proteinuria developed in 72.6–75% [8, 25]. Especially a median renal survival age of 65.0 years in females with XLAS was reported [8]. Thus, ESRD at 9-year old in female is too early to diagnose as XLAS. In the other hand, hematuria is a common clinical feature in all males with XLAS and 90% of male patients are at risk of developing ESRD before the age of 40 [9]. However, all the six males with only c.2858G>T(p.(G953V)) variant in COL4A5 gene had no hematuria. Furthermore, two of the males had normal result of urine analysis at age of 35 and 42. Therefore, no clues to support diagnosis of XLAS in all of the 17 individuals who detected with only c.2858G>T(p.(G953V)) variant in COL4A5 gene, especially for males. In addition, the variant c.2858G>T(p.(G953V)) in COL4A5 gene has a high allele frequency of more than 0.01 in 1000 Genomes, gnomAD—Genomes, gnomAD—Exomes and ExAC, which implies its benign possibility.
By reviewing of patients diagnosed as XLAS and detected with c.2858G>T(p.(G953V)) in COL4A5 gene previously reported [6, 18, 20], we found that totally four patients have been reported. In three of them, COL4A5 gene was tested by RT-PCR and direct sequencing. And in each of the three patients, c.2858G>T(p.(G953V)) in COL4A5 gene and another pathogenic mutation in COL4A5 gene were detected on the same allele in the same family [6, 18]. Only in one patient, the three Alport genes were detected by NGS. And the variant c.2858G>T(p.(G953V)) in COL4A5 gene and a splicing variant c.3817+1G>T in COL4A4 gene were detected [20]. Together with the individuals in group 2 in this study, the clinical manifestations of AS in these patients may not be caused by c.2858G>T(p.(G953V)) in COL4A5 gene. Further information and researches are required to explore whether the variant c.2858G>T(p.(G953V)) in COL4A5 gene would have a modifier effect in the phenotype.
Glycine substitutions in a collagenous domain of the a (IV) chain are usually disease causing variants. However, a few of Glycine substitutions have been considered neutral polymorphisms, including c.127G>C (p.Gly43Arg) in COL4A3, c.2996G>A (p.Gly999Glu) in COL4A4, c.1634G>C (p.Gly545Ala) in COL4A4. Accompanied by the wide application of NGS in diagnosis of AS, we would get a better understanding of the pathogenicity of variants in Alport genes. And in order to make an accurate diagnosis, the gene results must combined with clinical manifestations.
Therefore, we should carefully use the criteria “a pathogenic mutation in the COL4A5 gene” to confirm the diagnoses of XLAS [13, 24, 26]. Persistent glomerular hematuria should not be ignored and it is the basement for diagnoses of XLAS [9, 25, 27]. In the case with only one missense variant in COL4A5 gene (including glycine substitutions), any of the following items including [27] positive family history of AS or renal failure, hearing loss, typical ocular lesions, typical GBM changes of AS, and abnormal staining of collagen IV α5 chain would help to avoid a misdiagnoses of XLAS.
In summary, the cases we reported here providing evidence to reassess the pathogenicity of c.2858G>T(p.(G953V)) in COL4A5 gene. We conclude c.2858G>T(p.(G953V)) in COL4A5 gene is not a pathogenic variant for XLAS. Individuals should not be diagnosed as XLAS only based on the detection of c.2858G>T(p.(G953V)) in COL4A5 gene.
References
Flinter F. Alport’s syndrome. J Med Genet. 1997;34:326–30.
Kashtan CE. Alport syndrome. An inherited disorder of renal, ocular, and cochlear basement membranes. Medicine. 1999;78:338–60.
Zhang Y, Ding J. Renal, auricular, and ocular outcomes of Alport syndrome and their current management. Pediatr Nephrol. 2018;33:1309–16.
Barker DF, Hostikka SL, Zhou J, Chow LT, Oliphant AR, Gerken SC, et al. Identification of mutations in the COL4A5 collagen gene in Alport syndrome. Science. 1990;248:1224–7.
Mochizuki T, Lemmink HH, Mariyama M, Antignac C, Gubler MC, Pirson Y, et al. Identification of mutations in the alpha 3(IV) and alpha 4(IV) collagen genes in autosomal recessive Alport syndrome. Nat Genet. 1994;8:77–81.
Inoue Y, Nishio H, Shirakawa T, Nakanishi K, Nakamura H, Sumino K, et al. Detection of mutations in the COL4A5 gene in over 90% of male patients with X-linked Alport’s syndrome by RT-PCR and direct sequencing. Am J Kidney Dis. 1999;34:854–62.
Kashtan CE, Ding J, Gregory M, Gross O, Heidet L, Knebelmann B, et al. Alport Syndrome Research Collaborative. Clinical practice recommendations for the treatment of Alport syndrome: a statement of the AlportSyndrome Research Collaborative. Pediatr Nephrol. 2013;28:5–11.
Yamamura T, Nozu K, Fu XJ, Nozu Y, Ye MJ, Shono A, et al. Natural history and genotype–phenotype correlation in female x-linked alport syndrome. Kidney Int Rep. 2017;2:850–5.
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, et al. X-linked Alport syndrome: natural history in 195 families and genotype–phenotype correlations in males. J Am Soc Nephrol. 2000;11:649–57.
Wang F, Ding J, Guo S, Yang J. Phenotypic and genotypic features of Alport syndrome in Chinese children. Pediatr Nephrol. 2002;17:1013–20.
Savige J, Storey H, Il Cheong H, Gyung Kang H, Park E, Hilbert P, et al. X-Linked and autosomal recessive alport syndrome: pathogenic variant features and further genotype–phenotype correlations. PLoS ONE. 2016;11:e0161802.
Bekheirnia MR, Reed B, Gregory MC, McFann K, Shamshirsaz AA, Masoumi A, et al. Genotype–phenotype correlation in X-linked Alport syndrome. J Am Soc Nephrol. 2010;21:876–83.
Savige J, Ariani F, Mari F, Bruttini M, Renieri A, Gross O, et al. Expert consensus guidelines for the genetic diagnosis of Alport syndrome. Pediatr Nephrol. 2018. https://doi.org/10.1007/s00467-018-3985-4.
Wang YF, Ding J, Wang F, Bu DF. Effect of glycine substitutions onalpha5 (IV) chain structure and structure-phenotype correlations in Alport syndrome. Biochem Biophys Res Commun. 2004;316:1143–9.
Liu JH, Wei XX, Li A, Cui YX, Xia XY, Qin WS, et al. Novel mutations in COL4A3, COL4A4, and COL4A5 in Chinese patients with Alport Syndrome. PLoS ONE. 2017;12:e0177685.
Fallerini C, Baldassarri M, Trevisson E, Morbidoni V, La Manna A, Lazzarin R, et al. Alport syndrome: impact of digenic inheritance in patients management. Clin Genet. 2017;92:34–44.
Knebelmann B, Breillat C, Forestier L, Arrondel C, Jacassier D, Giatras I, et al. Spectrum of mutations in the COL4A5 collagen gene in X-linked Alport syndrome. Am J Hum Genet. 1996;59:1221–32.
Wang F, Wang Y, Ding J, Yang J. Detection of mutations in the COL4A5 gene by analyzing cDNA of skin fibroblasts. Kidney Int. 2005;67:1268–74.
Miao Y, Xiong J, Zhang X, Huang H, Yu L, Chen J, et al. Genetic diagnosis of polycystic kidney disease, Alport syndrome, and thalassemia minor in a large Chinese family. Clin Sci. 2017;131:2427–38.
Mencarelli MA, Heidet L, Storey H, van Geel M, Knebelmann B, Fallerini C, et al. Evidence of digenic inheritance in Alport syndrome. J Med Genet. 2015;52:163–74.
Wang F, Zhang Y, Mao J, et al. Spectrum of mutations in Chinese children with steroid-resistant nephrotic syndrome. Pediatr Nephrol. 2017;32:1181–92.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, ACMG Laboratory Quality Assurance Committee. et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015;17:405–24.
Zhang X, Zhang Y, Zhang Y, Gu H, Chen Z, Ren L, et al. X-linked Alport syndrome: pathogenic variant features and further auditory genotype-phenotype correlations in males. Orphanet J Rare Dis. 2018;13:229.
Savige J, Sheth S, Leys A, Nicholson A, Mack HG, Colville D. Ocular features in Alport syndrome: pathogenesis and clinical significance. Clin J Am Soc Nephrol. 2015;10:703–9.
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, et al. X-linked Alport syndrome: natural history and genotype-phenotype correlations in girls and women belonging to 195 families: a “European Community Alport Syndrome Concerted Action” study. J Am Soc Nephrol. 2003;14:2603–10.
Gross O, Kashtan CE, Rheault MN, Flinter F, Savige J, Miner JH, et al. Advances and unmet needs in genetic, basic and clinical science in Alport syndrome: report from the2015 International Workshop on Alport Syndrome. Nephrol Dial Transpl. 2017;32:916–24.
Savige J, Gregory M, Gross O, Kashtan C, Ding J, Flinter F. Expert guidelines for the management of Alport syndrome and thin basement membrane nephropathy. J Am Soc Nephrol. 2013;24:364–75.
Acknowledgements
We thank all the children and their family members participated in this study. This work was supported by the National Key Research and Development Program of China (No. 2016YFC0901505): the registry study of rare diseases in children, the National Nature Science Foundation (81400685) and the Beijing key laboratory of molecular diagnosis and study on pediatric genetic diseases (BZ0317).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, Y., Ding, J., Wang, S. et al. Reassessing the pathogenicity of c.2858G>T(p.(G953V)) in COL4A5 Gene: report of 19 Chinese families. Eur J Hum Genet 28, 244–252 (2020). https://doi.org/10.1038/s41431-019-0523-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41431-019-0523-1
This article is cited by
-
Genotype–phenotype correlations for COL4A3–COL4A5 variants resulting in Gly substitutions in Alport syndrome
Scientific Reports (2022)
-
Consensus statement on standards and guidelines for the molecular diagnostics of Alport syndrome: refining the ACMG criteria
European Journal of Human Genetics (2021)
