
Abstract
Introduction
While lifelong and strict adherence to gluten-free diet (GFD) is essential for the successful treatment of celiac disease (CeD), only 30–50% of patients are able to maintain a good adherence to GFD. We determined factors influencing the adherence to GFD at various ecological levels including intra-personal, inter-personal, organizational, community and system-based levels in adult patients with CeD.
Methods
A questionnaire to assess the adherence was developed and it was administered in the CeD clinic to patients with CeD on GFD for >1 year. Adherence to GFD was assessed in a subset of patients (n = 320) using Celiac Disease Adherence Test (CDAT).
Results
Overall, 978 patients [median age: 29 years; females: 592] with CeD on GFD were recruited. They reported many barriers to adherence to GFD including intra-personal barriers such as lack of knowledge about GFD (19%), inadequate financial resources (27.2%) and lack of self-motivation/confidence (55.3%); inter-personal barriers such as intake of gluten-containing food upon forceful insistence of friends/family (23.4%); organizational barriers such as high cost (70.8%) and non-availability of GF-food products (48.6%); community-based barriers like consumption of gluten-containing food at religious occasions/festivals (11.1%) and social occasions (27.2%); and system-based barriers such as non-referral to dietitian for counseling (21.9%). As per CDAT, 204 (63.7%), 73(22.8%) and 43(13.4%) patients had good, average, and poor adherence to GFD, respectively. On multivariable analysis, occasional consumption of gluten, non-availability of GF-food while dining out and coercing by family and friends for consumption of GC-food were found to have highest odds for poor adherence to GFD.
Conclusions
Non-referral to a dietitian for counseling, irregular follow-up visits, unavailability of flour mill, non-supportive family/friends, high cost and limited availability of GF-food are the most common barriers to adherence to GFD. There is a need to create infrastructure and develop strategies to overcome these diverse barriers at various levels of ecosystem and thereby facilitate better adherence to GFD.
Similar content being viewed by others


Introduction
Celiac disease (CeD) is an immune-mediated enteropathy induced by dietary gluten in genetically susceptible individuals. The prevalence of CeD is increasing worldwide, making it one of the most common and lifelong food-related autoimmune disorders [1, 2]. Previously considered uncommon in Asia, CeD is now widely being recognized in the Middle East and in the Indian subcontinent, with prevalence equivalent to that of Western countries [3]. At present, strict adherence to gluten-free diet (GFD) is the only definitive and effective treatment for patients with CeD [2]. The adherence to GFD is not just a dietary-based intervention for controlling symptoms and for reversal and maintenance of pathophysiological abnormalities, but also requires behavioral change for adopting a gluten-free (GF) lifestyle. Owing to the ubiquitous nature of gluten, patients with CeD report multiple challenges in maintaining the adherence to GFD in different arenas of their lives including schools, colleges, workplace, traveling, dining out of the home, or social functions [4]. In order to explore the challenges faced by patients with CeD in maintaining a good adherence to GFD, we need to understand the core facilities required such as knowledge and attitude, family support, financial status and affordability of additional cost of GF-food products, availability and quality of GF-food products and membership in Celiac Support Groups.
While multiple studies from across the globe have shown the rate of adherence to GFD in adult patients with CeD between 45 and 90% [5,6,7,8,9,10], very few have reported the barriers faced by patients in maintaining good adherence to GFD [4, 11,12,13,14,15,16]. Furthermore, only a few studies have reported the challenges faced by individuals with CeD in adhering to GFD at multiple levels of ecosystem [17, 18]. One of them is a systematic review by Abu-Janb N, et al. which has described the barriers based on Social Ecological Model (SEM) [18]. The SEM covers five levels of network of integral relationship between an individual’s health behavior and his/her environment such as intrapersonal level (e.g. knowledge, income, skills, attitudes, self-efficacy and self-confidence); the interpersonal level (e.g. family, spouse, in-laws, parenting and personal relationships, peer pressure/support, motivation from others); the community level (e.g. social network, cultural factors, and workplace settings); the organizational level (e.g. food environment, service, community and recreational facilities) and the system level (e.g. hospital care, adequacy of dietary counseling, evaluation on follow up and re-counseling, educational resources, quality of GF food products, food supply-chain, labeling of food items, financial support, and taxation) [19, 20].
With a burden of 1% of population having CeD [21], and a large number of patients following GFD, it is thus essential for health professionals, regulatory bodies and the food industry to understand the challenges faced by patients with CeD. Since there is a paucity of detailed data on the barriers to maintenance of adherence to GFD from Asia, we conducted a questionnaire-based survey to assess the barriers faced by adult patients with CeD in maintaining good adherence to GFD at various levels of ecological system.
Patients and methods
The present observational study was conducted at our institute between January 2021 and August 2022. The study was approved by the Ethics Committee of the institute
Development of the study questionnaire
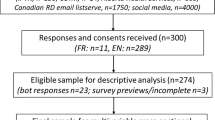
An exhaustive review of current literature was carried out to identify the existing evidences on the factors affecting adherence to GFD in adult patients with CeD across the globe. Further, six sessions of group discussion with an expert panel consisting of three gastroenterologists (AA, AC, GM), four dieticians (WM, AB, NS, AM), one-hundred and twenty adult patients with CeD (females – 68 (56.7%)) and their family members were conducted to discuss the factors influencing the adherence to GFD at multiple levels of ecosystem (intrapersonal, interpersonal, community, organizational and system). After a detailed review of literature and group discussions with expert panel, the following domains (Fig. 1) were identified under five levels of SEM and a bank of questionnaire items was developed. The final questionnaire consisted of 72 questions, with 10 questions in demographics section and 62 questions relating to the domains selected (Supplementary table 1). Kuppuswamy scale 2020 was used for assessing the socio-economic status (SES) of the participants [22].

Factors influencing adherence to gluten-free diet under different levels of Social-Ecological Model.
Administration of questionnaire
Prior to survey distribution, the questionnaire was administered to a group of 15 patients for pilot testing and was subsequently modified for removing the discrepancies and for providing more clarity to the respondents. The patients registered in the Celiac Clinic were reviewed and eligible participants were contacted through phone call or electronic-mail. The questionnaire was administered in a face-to-face interview to those who agreed or were scheduled for a follow-up visit in the Celiac Clinic. For others not agreeing to visit the clinic, detailed interview of patients and their close relatives were conducted telephonically and the responses were recorded in the questionnaire sheet.
The inclusion criteria were – a definite diagnosis of CeD as per standard guidelines and those who were following GFD for more than 1 year. Recruited participants were adults (age range: 19–55 years), having no other diet related disorder and any associated co-morbid illness (e.g., liver cirrhosis, inflammatory bowel disease, cardiovascular disease, any type of cancer, etc.). Eligible patients volunteering to participate in the study signed the consent form and were provided with written information sheet about the study conducted.
Adherence to gluten-free diet
The adherence to GFD was also assessed in a subset of patients (n = 320) using a standardized tool named “Celiac disease adherence test (CDAT)”. CDAT is a 7-item questionnaire, having five responses, with score ranging from 1 to 5. Scores of less than 13 are associated with good GFD adherence, 13–17 with average and greater than 17 are associated with poor GFD adherence [23].
Statistical analysis
The data are presented as median, inter-quartile range (IQR), proportions and percentages as appropriate. The frequencies and descriptive statistics were examined for each variable. Univariate and multivariate logistic regression analysis was conducted to identify factors affecting adherence to GFD and to assess barriers which influenced the adherence independently from each other, respectively. Relevant tests of factor analysis (KMO test, Bartlett’s Test of Sphericity, principal component analysis (PCA), varimax rotation with Kaiser normalization) were conducted to confirm the domains included in the questionnaire. A p-value less than 0.05 is taken as statistically significant. Statistical analysis has been performed using Software Program Stata System (SPSS) v20.0 (SPSS Inc., IBM Corporation, Chicago, Illinois).
Results
Nine hundred and seventy-eight patients with CeD following GFD for more than 1 year with median age of 32 years (IQR: 20–41 years, female: 60.5%) were included in this study. More than half of the patients (n = 510, 52.1%) were following GFD for 1–5 years and around one-third (n = 296, 30.3%) of patients belonged to lower-middle income group as per the Kuppuswamy scale. One hundred and sixty-nine (17.3%) patients had a family history of CeD with a predominance of female relatives (mothers: 20.7%, sisters: 22.5%, and daughters:17.7%) (Table 1).
Barriers to adherence to GFD
Intra-personal level
At the intra-personal or individual level, income, knowledge about GFD, availability of flour mill, sensory factors, food preparation and behavior and temptation control were the main factors related to adherence to GFD in adult patients with CeD (Table 2).
Other factors influencing adherence to GFD at intrapersonal level included overall health status and psychological factors.
Overall health status
While on one hand, 195 (20%) and 109 (11.1%) patients suffered moderate and severe weight loss, respectively, on the other hand 353 (36.1%) and 188 (19.2%) patients reported moderate and excessive weight gain. Further, 133 (13.6%) patients reported no change in weight after following GFD. Approximately, 207 (21.2%) patients reported moderate to severe decrease in appetite while 544 (55.6%) patients reported moderate to severe increase in appetite. Also, 227 (23.2%) patients reported no change in appetite after following the GFD.
Psychological factors
Overall, 394 (40.3%) patients believed that they were making mistakes in their dietary choices and were not following the GFD properly while 541 (55.3%) patients were not self-willing and self-motivated to follow the GFD strictly. Further, 231 (23.6%) patients felt that they had lost their self-esteem due to the disease itself and the extra efforts required to maintain the special dietary needs whereas 480 (49.1%) patients felt no change in their self-confidence while on GFD. Furthermore, 304 (31.1%) patients felt embarrassed in refusing food at religious places/marriages/festivals/birthdays, etc.
Inter-personal level
At the inter-personal level, support and motivation from friends/family, awareness among friends/family and confidence in health practitioner(s) were the main factors found to be influencing adherence to GFD in adult patients with CeD (Table 3).
Community level
At the community level, socio-cultural factors and lack of awareness in the society about CeD and its treatment were major factors which were impediment to maintenance of appropriate adherence to GFD.
Socio-cultural factors
Amongst all, 65 (6.6%) patients with CeD admitted eating GC “religious offerings (prashad, often made up of wheat)” at religious places because they could not refuse. Religious offering is considered very sacred in India, and further, 109 (11.1%) and 266 (27.2%) patients admitted consuming GC-food items at religious occasions/festivals and social occasions such as marriages, birthdays etc., respectively. Seventy-eight (7.9%) patients reported that they had to consume GC-food items because of forceful insistence by relatives and friends.
Lack of awareness about the disease in the society
Overall, 267 (27.3%) patients reported that their relatives were unaware about CeD while 419 (42.8%) patients mentioned that their relatives did not understand the consequences of eating gluten despite knowing about their disease.
Organizational level
At the organizational level, cost and availability of GFD, eating out and traveling and membership to the Celiac Support Groups were the main factors related to adherence to GFD in adult patients with CeD (Table 4).
System level
At the system level, counseling for GFD, facilitation of follow-up visits, contact with health practitioner(s) and access to healthcare resources were main factors influencing adherence to GFD in patients with CeD (Table 4).
Rate of adherence to GFD
The adherence to GFD was assessed via Celiac Disease Adherence Test (CDAT) in a subset of patients (n = 320). Based on the scores of CDAT, 204 (63.7%), 73 (22.8%) and 43 (13.4%) patients were found to have good, average, and poor adherence to GFD, respectively.
Factors affecting adherence to GFD
Univariate logistic regression
On univariate logistic regression analysis, the rates of non-adherence to GFD were high (CDAT score >17) in those patients with CeD who considered occasional intake of gluten as normal and those who were forced by family members, spouse, friends, and colleagues to eat GC-food at multiple occasions and social events (Odds ratio (OR) > 5) (Table 5). The odds of poor or average adherence to GFD were also higher among those who considered GF-foods to be expensive, faced non-availability of GF-food while dining out, and traveling, etc. and who were not counseled by a dietitian (Table 5).
Multivariate logistic regression
Since it is probable that some barriers cluster in the same individuals and have overlapping relations with the adherence to the GFD, a multivariate logistic regression was also performed to assess which barriers influence the adherence independently from each other. The R-squared for overall model obtained from multivariate analysis was 0.74 which shows a high level of correlation between the adherence and the barriers to GFD. Through this model, we identified some other barriers to GFD (OR > 3) in addition to those obtained from univariate analysis. The odds of poor adherence to GFD were also high among patients who had lack of provision of detailed list of dietary do’s and don’ts, non-membership in celiac support groups and among those whose family members were non-counseled for GFD (Table 5). The other factors obtained were similar to those obtained from univariate analysis.
Factor analysis
We also conducted factor analysis to see if all the barriers explored could be reduced to few factors. The data was found to be appropriate for conducting factor analysis (KMO value = 0.861; Bartlett’s test of sphericity, p < 0.01) suggesting proportion of variance and interrelationship among variables that might be due to various underlying factors. We conducted factor analysis under each ecological level as well as for the overall questionnaire (Table 6). Although, the overall questionnaire consisted of twenty separate domains which were initially postulated, but after PCA, nine different factors were extracted (eigenvalues > 1) with a cumulative variance of 68.6% (Table 6) and a different combination of items. Variables were loaded into extracted factors using varimax rotation with Kaiser Normalization, obtaining a component loading of greater than 0.50 for each variable. The expert panel reviewed the factors identified and by consensus renamed them based on their clinical features: 1) Socio-cultural factors, 2) Financial factors and purchasing power, 3) Psychological and behavioral factors, 4) Counseling of GFD and post treatment care, 5) Access to healthcare system, 6) Availability of GFD while eating out and traveling, 7) Awareness about the disease and treatment, 8) Support from friends/ family members and 9) Miscellaneous other factors.
However, the results are presented based on the initial domains postulated under each ecological level.
Discussion
Non-adherence to GFD is considered as one of the major significant obstacles in the successful treatment of CeD. Since CeD is relatively a new disease, the awareness about the disease amongst health-care professionals and patients varies from country to country. Unlike treatment of many other diseases, the only treatment of CeD is strict dietary restriction, however the delivery of dietary treatment is very heterogenous. Successful institution of GFD requires proper infrastructure having well informed patients, celiac expert dietician, availability of affordable and wide varieties of GF-food, knowledge about and use of naturally GF grains, appropriate supply chain of GF-food closer to patients living, labeling of GF-food items, and quality assurance etc. However, availability of such infrastructure is not uniform, and varies from region to region. Non-availability of adequate infrastructure acts as an impediment in the adherence to GFD. While prescribing a GFD is easy, it is extremely challenging for patients with CeD to maintain a strict and prolonged adherence to GFD.
The present study is the first known quantitative survey to assess the challenges faced by adult patients with CeD in adhering to GFD, at different domains of human ecosystem including intrapersonal, interpersonal, organizational, community, and system level. At the intrapersonal level, at least one-fourth patients reported that their income did not support their diet and around 10% of patients had to take financial help to buy GF-food items. Studies from Iran [24] and United Kingdom [25, 26] also reports higher cost of living for patients on GFD. Further, around one-fourth of patients considered occasional intake of gluten as acceptable, hence a better understanding of adverse outcomes of gluten consumption amongst CeD patients is likely to impact the adequacy of adherence to GFD [27].
At the intrapersonal level, a home-based separate flour mill was not available to 45% of patients. Patients with low income rely on grinding naturally occurring GF grains using home-based mills. Non-availability of home-based flour mills compels them to get these grains grinded at the commercial mills where they ground all kinds of grains, and hence exposing GF-flour to gluten contamination. Among the psychological and behavioral factors, more than half of patients were non-motivated to follow GFD, one-fourth of patients lost their self-esteem due to the disease and about one-fourth of them were depressed because of their inability to consume GC-food served at social functions (GF-food items are most often not served at such occasions). Furthermore, depression and anxiety in patients with CeD have been associated with reduced adherence to GFD [15, 28,29,30]. The findings of the present study along with data from previous studies suggest that psychological support should be an integral part of counseling of patients with CeD in order to enhance adherence to GFD.
At the interpersonal level, approximately 20% of patients with CeD reported lack of awareness about their disease amongst family/friends and non-supportive in-laws. In the present study, forceful consumption of GC-food upon insistence of family/friends has also been reported as a major factor for poor adherence to GFD. High level of support from family and friends lowers the risk of isolation and feeling of being alienated, thereby, improving the adherence to GFD [4, 16, 31]. Thus, it is important to counsel both the patient and their family members to make them understand about the importance of GFD for patients with CeD.
At the organizational level, more than half of patients in the present study reported GF-food products to be expensive and unavailable in markets/stores, leading to consumption of GC-food products by approximately 10% of patients. Studies from Italy [32], Australia [33], Austria [34], Brazil [35], Canada [36], Chile [37], Greece [38] and USA [39] stand in consonance with the observation of the present study that GF-foods are expensive than their GC-counterparts. Limited ability to afford GF-food has been associated with poor adherence to GFD as reported from studies from many Western countries [15, 16, 40]. Interestingly, around three-fourth (77%) patients of the present study expressed their concern towards non-supportive restaurant staff in catering GF-foods while around one-third and one-fourth of patients mentioned their inability to find GF-food while dining out and traveling, respectively. Having better access to GF-food products while eating out or shopping leads to increased adherence to GFD [11, 41]. Thus, there is a need to spread awareness about cooking of GF-food among restaurant chefs and the general public in order to ensure safe supply of GF-food in public eateries. Further, one-third patients of the present study reported non-membership in Celiac Support Groups. Membership in Celiac Support Groups results in increased likelihood of adhering to GFD [4, 26]. These Celiac Support Groups allow patients to get connected with experienced patients, which allow them to share their personal experiences, sharing of coping strategies, GF recipes, safe shopping of GF products, and safe dining out places, etc.
At the system level, more than one-fifth of patients in the present study were not referred to a dietitian for counseling, and around one-third of patients started GFD without any counseling by a dietitian. Another study from USA also reported non-referral to a dietitian for counseling and difficulty in finding a celiac specialist dietitian in 21% and 40% of patients, respectively [42]. Further, more than 50% of patients in the present study reported irregular follow-up visits with both physician and dietitian and no contact details of their concerned healthcare provider. Other studies from USA [42], Australia [43] and Olmsted county [44] have also reported irregularity in follow-up visits after first counseling. Getting counseled by a celiac expert dietitian, having access to a health-care practitioner in case of emergencies and regular follow-up with a dietitian has been positively correlated with better adherence to GFD [26, 41]. Also, more than one-third of patients in the present study were not given any detailed GFD chart. Provision of detailed description of CeD, treatment, GFD and its benefits to newly diagnosed patients allows them to follow GFD accurately [18].
In the present study, specific factors responsible for poor adherence to GFD were also identified through regression analysis which included occasional consumption of gluten, forceful intake of gluten through family members, spouse, friends, and colleagues to eat GC-food at multiple occasions and social events, considering GF-foods to be expensive, non-availability of GF-food while dining out and traveling, non-counseling of GFD by a dietitian, lack of provision of detailed list of dietary do’s and don’ts and non-membership in celiac support groups.
The factors or domains identified from factor analysis including socio-cultural factors, financial factors and purchasing power, psychological and behavioral factors, counseling of GFD and post treatment care, access to healthcare system, availability of GFD while eating out and traveling, awareness about the disease and treatment, support from friends/ family members and miscellaneous other factors are wholesome and includes all aspects of human ecosystem.
The strengths of the present study include development of the questionnaire based on extensive review of the relevant literature and multiple group meetings including patients, inclusion of relatively large number of patients with experience of challenges faced over a prolonged period of time, involvement of patients with various socioeconomic statuses and administration of the questionnaire by a celiac expert dietitian in face-to-face interview setting. To the best of our knowledge, the present study is the first quantitative survey to look at the challenges faced by patients with CeD in adhering to GFD, at different levels of ecosystem. The outcome of the present study is limited by lack of validation of the questionnaire developed by us. Also, the barriers explored by the questionnaire have not been analyzed in relation to hard clinical outcomes including anti-tTG antibodies or symptoms. Further, every country/region have their own social structure and challenges, and thus, region and country specific barriers have not been addressed in the present study.
In conclusion, the present study indicates multiple barriers to the adherence of GF lifestyle at all levels of human ecosystem. Non-referral to a dietitian for counseling, lack of knowledge about GFD, irregular follow-up visits, lack of self-motivation, non-supportive family/friends, high cost and decreased availability of GF-food, non-provision of educational material to learn about GFD and non-membership in celiac support groups are the most common barriers to adherence to GFD. Forceful consumption of GC-food upon insistence of family/friends has been reported as a major factor for poor adherence to GFD. There is a need to create infrastructure for removal of these barriers at various levels of ecosystem for a better adherence to GFD by patients with CeD. At the governmental and societal level, gluten appropriate policies should be adopted for the overall improvement in the adherence to GFD.
Data availability
The data generated and analyzed during this study can be found within the published article, or from the corresponding author on reasonable request.
References
Parzanese I, Qehajaj D, Patrinicola F, Aralica M, Chiriva-Internati M, Stifter S, et al. Celiac disease: From pathophysiology to treatment. World J Gastrointest Pathophysiol. 2017;8:27–38.
Ludvigsson JF, Leffler DA, Bai JC, Biagi F, Fasano A, Green PHR, et al. The Oslo definitions for coeliac disease and related terms. Gut. 2013;62:43–52.
Poddighe D, Abdukhakimova D. Celiac disease in asia beyond the middle east and indian subcontinent: epidemiological burden and diagnostic barriers. World J Gastroenterol. 2021;27:2251–6.
Silvester JA, Weiten D, Graff LA, Walker JR, Duerksen DR. Living gluten‐free: adherence, knowledge, lifestyle adaptations and feelings towards a gluten‐free diet. J Hum Nutr Dietetics. 2016;29:374–82.
Tovoli F, Negrini G, Sansone V, Faggiano C, Catenaro T, Bolondi L, et al. Celiac disease diagnosed through screening programs in at-risk adults is not associated with worse adherence to the gluten-free diet and might protect from osteopenia/osteoporosis. Nutrients. 2018;10:1940.
Costa AF, Sugai E, Temprano MdelaP, Niveloni SI, Vázquez H, Moreno ML, et al. Gluten immunogenic peptide excretion detects dietary transgressions in treated celiac disease patients. World J Gastroenterol. 2019;25:1409–20.
Paganizza S, Zanotti R, DʼOdorico A, Scapolo P, Canova C. Is adherence to a gluten-free diet by adult patients with celiac disease influenced by their knowledge of the gluten content of foods? Gastroenterol Nurs J Soc Gastroenterol Nurses Assoc. 2019;42:55–64.
Dana ZY, Lena B, Vered R, Haim S, Efrat B. Factors associated with non adherence to a gluten free diet in adult with celiac disease: A survey assessed by BIAGI score. Clin Res Hepatol Gastroenterol. 2020;44:762–7.
Fueyo-Díaz R, Magallón-Botaya R, Gascón-Santos S, Asensio-Martínez Á, Palacios-Navarro G, Sebastián-Domingo JJ. The effect of self-efficacy expectations in the adherence to a gluten free diet in celiac disease. Psychol Health. 2020;35:734–49.
Ruiz-Carnicer Á, Garzón-Benavides M, Fombuena B, Segura V, García-Fernández F, Sobrino-Rodríguez S, et al. Negative predictive value of the repeated absence of gluten immunogenic peptides in the urine of treated celiac patients in predicting mucosal healing: new proposals for follow-up in celiac disease. Am J Clin Nutr. 2020;112:1240–51.
Zarkadas M, Cranney A, Case S, Molloy M, Switzer C, Graham ID, et al. The impact of a gluten-free diet on adults with coeliac disease: results of a national survey. J Hum Nutr Diet J Br Diet Assoc. 2006;19:41–9.
Lamontagne P, West GE, Galibois I. Quebecers with celiac disease: analysis of dietary problems. Can J Dietetic Pract Res. 2001;62:175.
Rajpoot P, Makharia GK. Problems and challenges to adaptation of gluten free diet by Indian patients with celiac disease. Nutrients. 2013;5:4869–79.
Ukkola A, Mäki M, Kurppa K, Collin P, Huhtala H, Kekkonen L, et al. Patients’ experiences and perceptions of living with coeliac disease - implications for optimizing care. J Gastrointest Liver Dis JGLD. 2012;21:17–22.
Dowd AJ, Tamminen KA, Jung ME, Case S, McEwan D, Beauchamp MR. Motives for adherence to a gluten‐free diet: a qualitative investigation involving adults with coeliac disease. J Hum Nutr Dietetics. 2014;27:542–9.
Muhammad H, Reeves S, Jeanes YM. Identifying and improving adherence to the gluten-free diet in people with coeliac disease. Proc Nutr Soc. 2019;78:418–25.
Garnweidner-Holme L, Sende K, Hellmann M, Henriksen C, Lundin KE, Myhrstad MC, et al. Experiences of managing a gluten-free diet on multiple levels of society: a qualitative study. BMC Nutr. 2020;6:1–7.
Abu‐Janb N, Jaana M. Facilitators and barriers to adherence to gluten‐free diet among adults with celiac disease: a systematic review. J Hum Nutr Dietetics. 2020;33:786–810.
Salihu HM, Wilson RE, King LM, Marty PJ, Whiteman VE. Socio-ecological Model as a Framework for Overcoming Barriers and Challenges in Randomized Control Trials in Minority and Underserved Communities. Int J MCH AIDS. 2015;3:85–95.
Elder JP, Lytle L, Sallis JF, Young DR, Steckler A, Simons-Morton D, et al. A description of the social–ecological framework used in the trial of activity for adolescent girls (TAAG). Health Educ Res. 2007;22:155–65.
Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16:823–36.
Saleem SM. Modified Kuppuswamy socioeconomic scale updated for the year 2020. Indian J Forensic Community Med. 2020;7:1–3.
Leffler DA, Dennis M, Edwards George JB, Jamma S, Magge S, Cook EF, et al. A Simple Validated Gluten-Free Diet Adherence Survey for Adults With Celiac Disease. Clin Gastroenterol Hepatol. 2009;7:530–536.e2.
Pourhoseingholi MA, Rostami-Nejad M, Barzegar F, Rostami K, Volta U, Sadeghi A, et al. Economic burden made celiac disease an expensive and challenging condition for Iranian patients. Gastroenterol Hepatol Bed Bench. 2017;10:258–62.
Barratt SM, Leeds JS, Sanders DS. Quality of life in coeliac disease is determined by perceived degree of difficulty adhering to a gluten-free diet, not the level of dietary adherence ultimately achieved. J Gastrointestin Liver Dis. 2011;20:241–5.
Hall NJ, Rubin GP, Charnock A. Intentional and inadvertent non-adherence in adult coeliac disease. A cross-sectional survey. Appetite. 2013;68:56–62.
Ford S, Howard R, Oyebode J. Psychosocial aspects of coeliac disease: A cross‐sectional survey of a UK population. Br J health Psychol. 2012;17:743–57.
Dowd AJ, Jung ME. Self-compassion directly and indirectly predicts dietary adherence and quality of life among adults with celiac disease. Appetite. 2017;113:293–300.
Kothe EJ, Sainsbury K, Smith L, Mullan BA. Explaining the intention-behaviour gap in gluten-free diet adherence: The moderating roles of habit and perceived behavioural control. J Health Psychol. 2015;20:580–91.
Villafuerte-Galvez J, Vanga RR, Dennis M, Hansen J, Leffler DA, Kelly CP, et al. Factors governing long-term adherence to a gluten-free diet in adult patients with coeliac disease. Aliment Pharm Ther. 2015;42:753–60.
Sainsbury K, Mullan B. Measuring beliefs about gluten free diet adherence in adult coeliac disease using the theory of planned behaviour. Appetite. 2011;56:476–83.
Gorgitano MT, Sodano V. Gluten-free products: From dietary necessity to premium price extraction tool. Nutrients. 2019;11:1997.
Lambert K, Ficken C. Cost and affordability of a nutritionally balanced gluten‐free diet: Is following a gluten‐free diet affordable? Nutr Dietetics. 2016;73:36–42.
Missbach B, Schwingshackl L, Billmann A, Mystek A, Hickelsberger M, Bauer G, et al. Gluten-free food database: the nutritional quality and cost of packaged gluten-free foods. Peer J. 2015;3:e1337.
Do Nascimento A, Fiates G, Anjos A, Teixeira E. Availability, cost and nutritional composition of gluten-free products. Br Food J. 2014;116:1842–52.
Pinto-Sanchez MI, Verdu EF, Gordillo MC, Bai JC, Birch S, Moayyedi P, et al. Tax-deductible provisions for gluten-free diet in Canada compared with systems for gluten-free diet coverage available in various countries. Can J Gastroenterol Hepatol. 2015;29:104–10.
Estévez V, Ayala J, Vespa C, Araya M. The gluten-free basic food basket: a problem of availability, cost and nutritional composition. Eur J Clin Nutr. 2016;70:1215–7.
Panagiotou S, Kontogianni MD. The economic burden of gluten‐free products and gluten‐free diet: a cost estimation analysis in Greece. J Hum Nutr Dietetics. 2017;30:746–52.
Lee AR, Ng DL, Zivin J, Green PH. Economic burden of a gluten‐free diet. J Hum Nutr Dietetics. 2007;20:423–30.
Lee AR, Ng DL, Diamond B, Ciaccio EJ, Green PH. Living with coeliac disease: survey results from the USA. J Hum Nutr Dietetics. 2012;25:233–8.
Butterworth JR, Banfield LM, Iqbal TH, Cooper BT. Factors relating to compliance with a gluten-free diet in patients with coeliac disease: comparison of white Caucasian and South Asian patients. Clin Nutr Edinb Scotl. 2004;23:1127–34.
Mahadev S, Simpson S, Lebwohl B, Lewis SK, Tennyson CA, Green PHR. Is dietitian use associated with celiac disease outcomes? Nutrients. 2013;5:1585–94.
Goodyer L, Brown LJ, Crowley E. Celiac disease knowledge and practice of dietitians in rural New South Wales, Australia. Food Nutr Sci. 2016;7:874–83.
Herman ML, Rubio–Tapia A, Lahr BD, Larson JJ, Van Dyke CT, Murray JA. Patients with celiac disease are not followed up adequately. Clin Gastroenterol Hepatol. 2012;10:893–9.
Acknowledgements
We acknowledge the contribution of each of the participants of the study. We would like to acknowledge Indian Council of Agricultural Research, Department of Biotechnology for providing grants for research on Celiac Disease. We do acknowledge the University Grants Commission for providing Fellowship to Wajiha Mehtab.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
WM: Review of literature, questionnaire development, data collection, data analysis, drafting of manuscript; AA: Review of literature, questionnaire development, data proofing, critical review of the paper; AC: Review of literature, questionnaire development, critical review of the paper; SA: Data analysis; AS: Data proofing, data analysis, critical review of the paper; AA: Data collection, data proofing; AB: Questionnaire development, data proofing, critical review of the paper; NS: Questionnaire development, critical review of the paper; VA: Critical review of the paper; AM: Questionnaire development, study supervision, critical review of the paper; GKM: Overall guarantor of the paper, designed the study concept, study supervision, data analysis, and finalization of the paper. All authors revised and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mehtab, W., Agarwal, A., Chauhan, A. et al. Barriers at various levels of human ecosystem for maintaining adherence to gluten free diet in adult patients with celiac disease. Eur J Clin Nutr 78, 320–327 (2024). https://doi.org/10.1038/s41430-024-01399-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-024-01399-8
