
Abstract
Early enteral feeding is vital for the physical health of preterm infants. However, there is uncertainty regarding the effects of early enteral feeding on health outcomes in preterm infants. Hence, we aimed to synthesise evidence from systematic reviews (SRs) to evaluate the effects of early enteral feeding on health outcomes in preterm infants. We conducted a literature search in PubMed, Web of Science, Scopus, and the Cochrane Database of Systematic Reviews. SRs selection followed clear inclusion and exclusion criteria. Two reviewers reached a consensus for the inclusion of SRs. The certainty of evidence and the quality of reviews using the GRADE and AMSTAR tools, respectively. We included nine SRs in this review. The effectiveness of early enteral feeding on health outcomes in preterm infants is mainly divided into six primary outcomes: increase the weight gain, reduce the incidence of feed intolerance, shorten the duration of full enteral feeding, reduce the length of hospital stay, reduce the incidence of necrotizing enterocolitis, and decrease the mortality risk. The overall quality of the included SRs was high, whereas most of the evidence was of low or very low certainty. Our results show the impact of early enteral feeding on health outcomes in preterm infants. Although the currently available data indicate that early enteral feeding may improve the health outcomes of preterm infants, additional clinical observation and investigation are required to evaluate the long-term health outcomes of preterm infants who receive early enteral feeding.
Similar content being viewed by others
Background
Preterm infants, whose gestational age (GA) is less than 37 weeks, face increased risks of morbidity and mortality compared with term infants [1]. Preterm infants are born with incomplete intestinal tract development [2]. Low intestinal immune function and poor gastrointestinal motility in preterm infants may harm their intestinal defense mechanisms and reduce the activity of certain digestive enzymes [3]. Due to the intestinal characteristics of preterm infants, especially those with co-morbidities, appropriate nutrition is a modifiable factor that plays a crucial role in their health outcomes.
Nutrition and growth are critical for preterm infants. Appropriate nutrition is essential for the growth and development of infants, and preterm infants have a greater requirement for nutritional support. Indeed, an adequate feeding approach helps them remain infection-free, boosts their digestive system, and provides adequate nutrients. Generally, breast milk has been recommended as the best type of nutrition for enteral feeding of premature babies [4, 5]. Oropharyngeal administration of colostrum (OAC) might reduce the time to achieve full enteral feeding [6]. Feeding supplements other than breast milk promote health outcomes in premature infants [7]. Although these studies have verified the benefits of enteral feeding, there is still no definitive conclusion on the optimal timing and effects of enteral feeding.
Enteral feeding is feeding through the gastrointestinal tract, usually through a tube or catheter, to deliver nutrition directly into the intestine. This approach provides the individual with adequate nutrient [8]. There are two different options in timing to start enteral feed feeding, namely early and late enteral feeding. Early enteral feeding is defined as the first enteral feeding received on or before the fourth day of life; late enteral feeding is defined as the first enteral feeding received beyond the fourth day of life [1]. The practice of early enteral feeding most closely resembles physiological condition. Although previous studies have concluded that necrotizing enterocolitis (NEC) and feed intolerance (FI) are the most feared complication of enteral feeding [9], late initiation of enteral feeding may not be an objective approach to avoid these complications.
Current studies are more supportive of the benefits of early enteral feedings in preterm infants [10, 11]. A retrospective cohort study reported that early enteral feeding yields better outcomes than late enteral feeding in preterm infants. Specifically, the author concluded that late enteral feeding is more likely to increase intestinal inflammatory makers and the risk of neonatal morbidity [12]. However, there are also some inconsistent conclusions about the effect of early enteral feeding on health outcomes in preterm infants. Some researchers have showed that early enteral feeding does not influence the clinical outcomes of preterm infants, such as mortality and the incidence of NEC [13, 14]. Moreover, other authors have supported the idea that late initiation of enteral feeding provides greater benefits for preterm infant [15, 16].
Given the above-mentioned results, the benefits and harms of early and late initiation of enteral feeding in preterm infants have received little research, and the effects on primary health outcomes remain uncertain. This review aimed to evaluate the certainty of the available systematic reviews (SRs) and the quality of the evidence to comprehensively describe the effectiveness of early enteral feeding in promoting health-related outcomes of preterm infants.
Methods
This overview adopted the guideline outlined by the Cochrane Handbook [17]. Because all data in this review have been published online, no ethical approval or patient consent was required.
Search methods
Four electronic databases (PubMed, Web of Science, Scopus, and the Cochrane Database of Systematic Reviews) were searched for SRs and meta-analyses up to December 2021. We used the following search terms: (‘preterm infant’ OR ‘preterm infants’ OR ‘preterm baby’ OR ‘preterm babies’ OR ‘premature infant’ OR ‘premature infants’ OR ‘preterm neonate’ OR ‘prematurity’ OR ‘low birth weight infant’ OR ‘very low birth weight infant’) AND (‘early enteral feeding’ OR ‘early enteral nutrition’ OR ‘early trophic feeding’). We did not apply language restrictions. Two reviewers independently searched all sources; the references of the articles to ensure that no references were missed.
Study selection, inclusion, and exclusion
Two reviewers independently selected the reviews by using ENDNOTE X9 and Microsoft Excel. They each evaluated the full texts and abstracts to assess the study’s inclusion eligibility and quality. They discussed discrepancies and consulted a third reviewer if needed.
The inclusion criteria were: (i) participants were preterm neonates; (ii) intervention was to initiate enteral feeding from birth to 96 h postnatally; (iii) the comparison was early enteral feeding with late enteral feeding or early enteral feeding with other interventions; and (iv) SRs focused on the impact of early and late enteral feeding on health outcomes of the preterm infants. When two or more similar SRs existed on a similar topic, they were evaluated in terms of publication time, sample size, primary outcomes, and content quality. Furthermore, the most consistent criteria were selected based on the findings, resulting in the best inclusion.
The exclusion criteria were: (i) participants were not preterm neonates; (ii) interventions did not meet the inclusion criteria; (iii) SRs had ambiguous results; (iv) no complete tests; and (v) SRs focused only on individual steps of early enteral feeding, rather than the feeding implementation and health outcomes.
Data extraction
Two reviewers independently extracted data from each SR using Microsoft Excel; subsequently, a third person checked this extraction. They collected the following data: author, publication year, the theme of the review, study design, study intervention, the number of studies included, the number of patients included, type of participants, the effectiveness of the intervention, and overall quality. The aim was to investigate the effect of early enteral feeding on promoting health outcomes of preterm infants, with post-feeding growth, early feeding complications (from birth to hospitalization), and health outcomes as the main outcomes. After group discussions, we classified the health outcomes: (i) weight gain, (ii) incidence of FI, (iii) the number of days to reach full enteral feeding, (iv) hospital stay, (v) morbidity of any disease, and (vi) all-cause mortality.
Data synthesis
The data synthesis involved the following steps. First, we adopted the Population, Intervention, Comparison, Outcomes, and Study (PICOS) criteria to integrate the characteristics and outcomes of the interventions and data sources. Second, we integrated the collected data into trilinear tables in Microsoft Excel. Third, we determined the effects of early enteral feeding on preterm infants. We have presented the extracted results in two tables, namely “characteristic of the included studies” and “characteristics of the interventions.”
Quality assessment
Two reviewers applied the Assessing the Methodological Quality of Systematic Reviews (AMSTAR) tool to independently assess the quality of included SRs [18].
This tool has 11 items, and the total score correlates positively with the quality of SRs: 11 is the highest quality, 8–11 is high quality, 4–7 is moderate quality, and 0–3 is low quality. Each SR was of high quality.
Two reviewers used the Grades of Recommendations, Assessment, Development, and Evaluation (GRADE) tool [19] to independently evaluate the certainty of evidence of conclusions and specific outcomes of each study. The GRADE tool assesses the level of bias across five domains: study limitation, indirectness, publication bias, imprecision, and inconsistency. According to the assessment, the evidence is categorized as high certainty, moderate certainty, low certainty, and very low certainty [20]. Although some of the included SRs included GRADE scores, we still applied this analysis. Disagreements between the two reviewers were resolved by research team discussion.
Results
Overview of reviews
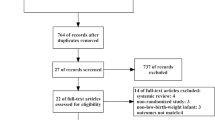
The initial search strategy yielded 1190 articles; after eliminating duplicates 1102 articles remained. After excluding unrelated titles and abstracts, the full text of 137 articles had their full text retrieved for analysis. One hundred and twenty-eight full-text articles were excluded for the following reasons: (i) intervention did not meet the inclusion criteria; (ii) ambiguous results; (iii) no meta-analysis; and (iv) incomplete tests. The selection process of the nine included SRs is depicted in Fig. 1.

The flow diagram of study selection.
Characteristics of the included SRs
The included SRs had been published between 2000 and 2021. Six SRs had been published between 2019 and 2021 [21,22,23,24,25,26], while the others had been published in 2014 [27], 2013 [11], and 2000 [1]. Overall, the nine SRs included 116 studies. The primary outcome was to assess the effect of early enteral feeding on the health outcomes. GA and birth weight were <37 weeks or <1500 g, meeting the criteria for premature infants. The nine SRs included any strategy for early enteral feeding. Late initiation of enteral feeding was the control. Regarding the sample sizes of the included studies, only three SRs [22,23,24] included more than ten original studies. The primary outcomes were weight gain, disease morbidity, and all-cause mortality. The secondary outcomes were the incidence of FI, the number of days to reach full feeding, and hospital stay durations. In terms of the included SRs, most of the results presented the incidence of disease, especially NEC [1, 11, 21,22,23,24,25,26,27]. The characteristics of the included SRs are provided in Table 1.
Effectiveness of the intervention on health outcomes and the quality of evidence
The effectiveness of the interventions on specific health outcomes of the included SRs is presented in Table 2. Overall, the nine SRs reported feeding-related conditions and health outcomes.
In terms of the effectiveness of early enteral feeding on health outcomes, four SRs [11, 21, 22, 25] concluded that the time of feeding initiation is associated with improved weight gain. One SR [23] concluded that early enteral feeding promotes adaptation of the immature gut and thus reduces the incidence of feeding intolerance. Three SRs [21, 26, 27] concluded that an early slow enteral feeding regimen shortens the number of days to reach full feeding without prolonging the duration of hospitalization.
One SR [22] provided the opposite conclusion, suggesting that early enteral feeding increases endogenous infection rather than reduces morbidity and mortality in premature infants. Four SRs [1, 11, 24, 25] reported no effect of the early enteral feeding on the preterm infants owing to there was no statistical significance.
We divided the health outcomes improved by early enteral feeding into six aspects: weight gain, the incidence of FI, the number of days to reach full enteral feeding, hospital stays, the morbidity of any disease, and all-cause mortality. Moreover, we assessed the certainty of the evidence for each aspect according to the GRADE tool (Table 3).
Methodological quality assessment of the included SRs
The methodological quality of the SRs determined according to the AMSTAR tool and presented in Table 4. All SRs were of high methodological quality, indicating that the SRs had a high rigor for article inclusion. One SRs scored 11 [26], five SRs scored 10 [11, 23,24,25, 27], two SRs scored 9 [1, 22] and one SRs scored 8 [21]. All included SRs met AMSTAR criterion A (prior design provided), criterion B (duplicate study selection and data extraction), criterion F (characteristics of the included studies provided), criterion G (scientific quality of the included studies assessed and documented), and criterion H (scientific quality of the included studies used appropriately in formulating conclusions). The least met AMSTAR criterion was 10 (the likelihood of publication bias assessed). A small sample size of the included SRs was the main cause of publication bias [11, 22,23,24,25, 27].
Data synthesis
Weight gain
The most commonly reported growth parameter is the time to regain birth weight, and the primary measure is weight gain during hospitalization. We assessed the effectiveness of early enteral feeding on weight gain based on six high-quality SRs [1, 11, 21, 22, 25, 27]. There are data from four trials on hospital weight gain. Early enteral feeding of preterm infants promoted weight gain and head circumference, and increased index scores (weight percentiles and z-scores) [11, 21, 22, 25]. Alshaikh et al. [21] concluded that early enteral feeding contributed to the recovery of birth weight. Walsh et al. [25] showed that birth weight was regained after several days of early enteral feeding. Oddie and Morgan et al. [11, 22] concluded that early enteral feeding promotes weight gain in a short period of time. There were both a very low degree of certainty of evidence based on the GRADE scores.
Two SRs [1, 27] concluded that early enteral feeding did not significantly increase weight gain.
The incidence of FI
FI is defined as the need to cease enteral feeds for more than 4 h. In preterm infants, FI is frequently associated with incorrect early enteral feeding. We assessed the effectiveness of early enteral feeding on the incidence of FI based on five high-quality SRs [11, 22, 23, 25, 27].
One SR concluded that early enteral feeding impacted on FI. Ramaswamy et al. [23] found that early enteral feeding may decrease the incidence of FI. There was a very low degree of certainty of evidence based on GRADE analysis. Meanwhile, three SRs [11, 25, 27] concluded that early enteral feeding had no effect on the incidence of FI. However, Oddie et al. [22] concluded that early enteral feeding might slightly increase the incidence of FI. There was a low degree of certainty of evidence based on the GRADE score.
The number of days to reach full enteral feeding
The number of days to achieve full enteral feeding represent the days from birth needed to establish full enteral feeding (at least 150 ml/kg/day) [28]. Reaching full feeding is required before premature infants can be discharged. Moreover, feeding recovery can improve the quality of life and prognosis of preterm neonates. We assessed the effectiveness of early enteral feeding on the number of days to achieve full enteral feeding based on five high-quality SRs [21,22,23, 26, 27].
Four SRs concluded that early enteral feeding on preterm neonates impacted the number of days to reach full feeding [21, 23, 26, 27]. Four SRs concluded that early enteral feeding of preterm infants reduced the number of days to achieve full enteral feeding. Three SRs had a low degree of certainty of evidence based on the GRADE score [21, 23, 26]. One SR had a very low degree of certainty of evidence based on the GRADE score [27].
Oddie et al. [22] demonstrated that early enteral feeding might increase the number of days to reach full enteral feeding. There was a low degree of certainty of evidence based on the GRADE score.
Hospital stay
Hospital stay is measured as the number of days to discharge [29]. The hospital stay is associated with disease progression and prognosis, as well as the quality of life of a preterm infant. We assessed the effectiveness of early enteral feeding on hospital stay based on five high-quality SRs [21, 22, 25,26,27].
Four SRs concluded that early enteral feeding on preterm babies has significantly reduced hospital stay [21, 22, 25,26,27]. The degree of certainty of evidence was low, moderate, very low, and very low, respectively, according to the GRADE score. Meanwhile, one SR reported the opposite result that early enteral feeding might increase hospital stay, but it was not statistically significant [22].
Morbidity of any disease
The most common complications among preterm infants are mainly due to inappropriate feeding. These complications include sepsis, NEC, and invasive infections. We assessed the effect of early enteral feeding on the morbidity of any disease based on nine high-quality SRs [1, 11, 21,22,23,24,25,26,27].
Seven SRs [1, 21,22,23,24,25,26] concluded that early enteral feeding of premature infants impacted disease morbidity. Kennedy et al. [1] concluded that early enteral feeding decreased late-onset sepsis and the need for a percutaneous venous catheter. There was a very low degree of certainty of evidence based on the GRADE score. Alshaikh et al. [21] showed that early enteral feeding with preterm infants could decrease the incidence of sepsis. There was a low degree of certainty of evidence based on the GRADE score. Walsh et al. [25] reported that early enteral feeding reduced the incidence of NEC. There was a very low degree of certainty of evidence based on the GRADE score. According to Oddie et al. [22], early enteral feeding on preterm infants may increase the incidence of NEC and invasive infection. There was a moderate and low degree of certainty of evidence, respectively, based on the GRADE score. Ramaswamy et al. [23] reported that early enteral feeding reduces the morbidity of NEC and sepsis. There was a very low degree of certainty of evidence based on the GRADE score. Ibrahim et al. [26] showed that early enteral feeding could reduce NEC. There was a low degree of certainty of evidence-based on the GRADE score. Kwok et al. [24] concluded that early enteral feeding could result in a significantly lower incidence of NEC and sepsis. There was a very low degree of certainty of evidence based on the GRADE score.
Two SRs [11, 27] had no data for quantitative integration and therefore did not report statistical significance.
All-cause mortality
We assessed the effect of early enteral feeding on all-cause mortality based on six high-quality SRs [11, 22,23,24,25].
Three SRs [22,23,24] concluded that early enteral feeding to preterm infants was related to mortality. Ramaswamy and Kwok et al. [23, 24] revealed that neonatal death was prevented by early enteral feeding and nutrition. Both had a very low certainty of evidence according to the GRADE score. Oddie et al. [22] concluded that early enteral feeding slightly increased all-cause mortality. There was a moderate certainty of evidence according to the GRADE score.
Three SRs [11, 25, 27] concluded that early enteral feeding had no significant effect on all-cause mortality, but the mortality related to NEC and sepsis was reported to be reduced.
Discussion
Summary of the main results
Although perinatal medicine and neonatal care are well developed, prematurity remains a global problem that significantly affects the morbidity and mortality of preterm infants. Early enteral feeding has recently been proposed as a potentially modifiable intervention to mitigate adverse outcomes for preterm babies. Several studies have revealed that early enteral feeding during hospitalization increases weight and reduces mortality in preterm infants. However, there is no definitive conclusion on the effectiveness of health outcomes of early enteral feedings. To address this problem, we re-evaluated nine SRs of early enteral feeding in preterm infants to determine its effects on health outcomes.
Four of the nine included SRs had a meta-analysis. The main intervention measures were postnatal feeding initiation time and the micro-feeding amount. The authors compared early enteral feeding with late enteral feeding and evaluated the effectiveness of early enteral feeding on health outcomes of preterm infants based on weight gain, the incidence of FI, the number of days to reach full feeding, hospital stays, the morbidity of any disease, and all-cause mortality. Although the quality of evidence was of low certainty, the methodological quality was high.
Among the included studies in the nine SRs, the authors provided two general conclusions regarding the effectiveness of early enteral feeding on health outcomes of preterm infants. The first conclusion is that early enteral feeding improved the health of preterm infants [1, 11, 21, 23,24,25,26]. Seven studies showed an overall positive trend, namely that early enteral feeding improves health outcomes. The results are consistent with previous studies that early enteral feeding in preterm infants could improve weight gain, reduce the incidence of NEC, and decrease the mortality risk. The second conclusion is the lack of consensus among the studies regarding the benefit of early initiation of enteral feeding. In two SRs, the authors suggested that early enteral feeding may not reduce the risk of feeding problems or the incidence of disease or death, and may even increase the risk of invasive infections in preterm infants [22, 27].
The health-promoting effect of early enteral feeding on preterm infants is reflected in weight gain, which is an essential indicator of the early volumes ingested and physical health. Based on 44 studies from six SRs [1, 11, 21, 22, 25, 27], we found evidence that early enteral feeding promoted weight gain in preterm infants. Among these six SRs, the author of three concluded that early enteral feeding promoted weight gain during hospitalization of preterm infants, which is consistent with our results [21, 22, 25]. Although the remaining three SRs [1, 11, 27] reported that early enteral feeding did not significantly increase weight gain in preterm infants, there was still an overall positive trend. It is worth noting that the heterogeneity of preterm infants and the variability of absorption may be crucial factors that underlie statistical insignificance. Therefore, we believe early enteral feeding could effectively promote weight gain in preterm infants.
The findings from the included SRs also support that enteral feeding reduce the incidence of NEC in preterm infants. The timing of the introduction of enteral feeding may be an influential modifiable risk factor for the development of NEC. Based on four SRs involving 53 studies, early enteral feeding slightly reduced the risk of NEC in preterm infants [23,24,25,26]. These SRs reported a similar incidence of NEC, but it is much lower the average described in the literature, thus suggesting the importance of early enteral feeding on the pathogenesis of NEC. This finding is consistency with the validity of the primary health outcomes. Although some SRs [1, 11, 21]showed no statistical significance due to the heterogeneity of the sample size and the control group intervention, their data indicate a correlation trend for reducing the incidence of NEC in premature infants.
Early enteral feeding contributes to reduce mortality in preterm infants. Reducing the mortality rate of preterm infants plays an important role in family support of preterm infants. Analysis of data from two SRs including 42 studies showed that early enteral feeding reduced the severity of disease and decreased the risk of complications, thereby lessening the risk of mortality [23, 24]. Considering individual differences in preterm infants and disease severity, the included studies found only limited growth, resulting in statistically insignificant support or early enteral feeding reducing mortality [11, 25, 27]. Although the results of our review have shown the effectiveness of early enteral feeding in promoting health outcomes of preterm infants, two SRs indicated that early enteral feeding is not significantly associated with protection of preterm infants [22, 27]. There are several reasons for the inconsistency between those findings and the results of this review. First, compared with other studies, enteral feeding was initiated within 96 h of birth in preterm infants, the earliest within 24 h. Early initiation of enteral feeding may result in delayed gastric emptying and immature gastrointestinal motility, which further affects the absorption of the required enteral nutrients and may increase adverse health outcomes. Second, these two SRs had large sample sizes, with a total of 4026 preterm infants from14 trials. The high individual variability and confounding factors contributed to bias in presenting health outcomes. Finally, related to the physiological mechanisms of the gastrointestinal tract of preterm infants. Early enteral feeding stimulated gastrointestinal hormone secretion, delaying gastrointestinal adaptation and disrupting bacterial colonization. Therefore, there was an increased risk of invasive infections and NEC, resulting mortality. To a certain extent, the above-mentioned reasons, underscored the lack of significant differences when examining the effects of early enteral feeding.
Our review has contributed to the theoretical basis for developing clinical feeding strategies for preterm infants. However, additional clinical observation and studies are needed to determine the health outcomes and effects of early enteral feeding on preterm infants. Last but not least, the decision regarding the duration and type of feeding should also consider the parents’ choice.
Strengths and limitations
The strength of this review is the rigorous and comprehensive search strategy conducted independently by two reviewers. Our review also has some limitations. First, there is heterogeneity in the included studies. Second, subjective inclusion and exclusion analysis may not be objective. Finally, the experimental results have existing risks of bias. Therefore, we used the GRADE and AMSTAR tools to evaluate the experimental results and the certainty of the evidence. Moreover, the small set of relevant evaluations included in the SRs was small, so we reassessed the GRADE scores to ensure their accuracy.
Implications for clinical practice and research
Despite the large number of feeding studies, this is the first overview of SRs focusing on the effectiveness of early enteral feeding in preterm infants. We found that early enteral feeding is associated with improved health outcomes in preterm neonates. Initiation of early enteral feeding could be considered to treat preterm infants for several reasons: (i) improve health outcomes, (ii) promote intestinal adaptation, and (iii) facilitate gastrointestinal tolerance. However, caution must be exercised when considering early enteral feeding for preterm infants, owing to the low quality of the published evidence. Therefore, more clinical research is required to confirm the reliability of its effects.
Conclusion
This overview of SRs provides evidence that early enteral feeding improves preterm infants’ health outcomes. The benefits of early enteral feeding include promoting weight gain, reducing the risk of NEC and mortality, reducing the time to achieve total enteral feeding, decreasing hospital stay, and lowering FI. Although the effect on the time to achieve total enteral feeding and FI is relatively small, the reduction in FI is likely to enhance the physical health of preterm infants. Therefore, early enteral feeding could be considered a potential protective nutritional strategy in clinical practice to promote the health outcomes of preterm infants. However, because the certainty of most of the evidence is not high, future clinical observation and research are still needed to focus on the effect of early enteral feeding on short and long-term health outcomes in preterm infants to provide an optimal clinical feeding strategy.
References
Kennedy KA, Tyson JE, Chamnanvanikij S. Early versus delayed initiation of progressive enteral feedings for parenterally fed low birth weight or preterm infants. Cochrane Database Syst Rev. 2000;2:Cd001970.
Thoene M, Anderson-Berry A. Early Enteral Feeding in Preterm Infants: A Narrative Review of the Nutritional, Metabolic, and Developmental Benefits. Nutrients. 2021;13:2289.
Munch A, Buhrer C, Longardt AC. Digestive enzyme replacement relieves growth failure in preterm infants with poor exocrine pancreatic function: a retrospective case series. Eur J Pediatr. 2021;180:2951–8.
Black A. Breastfeeding the premature infant and nursing implications. Adv Neonatal Care. 2012;12:10–1.
Section on, B. Breastfeeding and the use of human milk. Pediatrics. 2012;129:e827–41.
Tao J, Mao J, Yang J, Su Y. Effects of oropharyngeal administration of colostrum on the incidence of necrotizing enterocolitis, late-onset sepsis, and death in preterm infants: a meta-analysis of RCTs. Eur J Clin Nutr. 2020;74:1122–31.
Liu K, Tao J, Yang J, Li Y, Su Y, Mao J. Effectiveness of feeding supplementation in preterm infants: an overview of systematic reviews. BMC Pediatr. 2022;22:20.
Kozeniecki M, Fritzshall R. Enteral Nutrition for Adults in the Hospital Setting. Nutr Clin Pr. 2015;30:634–51.
Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis. Lancet. 1990;336:1519–23.
Abdelmaaboud M, Mohammed A. Early Versus Late Minimal Enteral Feeding in Weeks Preterm Growth-Restricted neonates with Abnormal Antenatal Doppler Studies. J Matern Fetal Neonatal Med. 2012:21. https://doi.org/10.3109/14767058.2012.695821.
Morgan J, Bombell S, McGuire W. Early trophic feeding versus enteral fasting for very preterm or very low birth weight infants. Cochrane Database Syst Rev. 2013;3:CD000504.
Konnikova Y, Zaman MM, Makda M, D’Onofrio D, Freedman SD, Martin CR. Late Enteral Feedings Are Associated with Intestinal Inflammation and Adverse Neonatal Outcomes. PLoS One. 2015;10:e0132924.
Panchal H, Athalye-Jape G, Patole S. Oropharyngeal Colostrum for Preterm Infants: A Systematic Review and Meta-Analysis. Adv Nutr. 2019;10:1152–62.
Garg BD, Balasubramanian H, Kabra NS, Bansal A. Effect of oropharyngeal colostrum therapy in the prevention of necrotising enterocolitis among very low birthweight neonates: A meta-analysis of randomised controlled trials. J Hum Nutr Diet. 2018;31:612–24.
Berseth CL, Bisquera JA, Paje VU. Prolonging small feeding volumes early in life decreases the incidence of necrotizing enterocolitis in very low birth weight infants. Pediatrics. 2003;111:529–34.
Brown EG, Sweet AY. Preventing necrotizing enterocolitis in neonates. JAMA. 1978 ;240:2452–4.
Pollock M, Fernandes RM, Becker LM, et al. Chapter V: overviews of reviews. In: Cochrane Handbook for Systematic Reviews of Interventions. Accessed July 14, 2020 /handbook/current/chapter-v.
Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol. 2009;62:1013–20.
Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rat Qual Evid–study Limit (risk bias) J Clin Epidemiol. 2011;64:407–15.
Meerpohl JJ, Langer G, Perleth M, Gartlehner G, Kaminski-Hartenthaler A, Schünemann H. GRADE-Leitlinien: 4. Bewertung der Qualität der Evidenz – Studienlimitationen (Risiko für Bias). Z für Evidenz, Fortbild und Qualät im Gesundheitswesen. 2012;106:457–69.
Alshaikh B, Dharel D, Yusuf K, Singhal N. Early total enteral feeding in stable preterm infants: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2021;34:1479–86.
Oddie SJ, Young L, McGuire W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst Rev. 2021;8:CD001241.
Ramaswamy VV, Bandyopadhyay T, Ahmed J, Bandiya P, Zivanovic S, Roehr CC. Enteral Feeding Strategies in Preterm Neonates </=32 weeks Gestational Age: A Systematic Review and Network Meta-Analysis. Ann Nutr Metab. 2021;77:204–20.
Kwok TC, Dorling J, Gale C. Early enteral feeding in preterm infants. Semin Perinatol. 2019;43:151159.
Walsh V, Brown JVE, Copperthwaite BR, Oddie SJ, McGuire W. Early full enteral feeding for preterm or low birth weight infants. Cochrane Database Syst Rev. 2020;12:CD013542.
Ibrahim NR, Van Rostenberghe H, Ho JJ, Nasir A. Short versus long feeding interval for bolus feedings in very preterm infants. Cochrane Database Syst Rev. 2021;8:CD012322.
Morgan J, Young L, McGuire W. Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. 2014;12:CD001970.
Moe-Byrne T, Brown JV, McGuire W. Glutamine supplementation to prevent morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2016;1:CD001457.
Pammi M, Suresh G. Enteral lactoferrin supplementation for prevention of sepsis and necrotizing enterocolitis in preterm infants. Cochrane Database Syst Rev. 2020;3:CD007137.
Funding
This work was supported by National Natural Science Foundation of China (81601330). The funder contributed to define the research theme, be fully accountable for ensuring the integrity and accuracy of the work, analyze the data and interpret the results.
Author information
Authors and Affiliations
Contributions
QL contributed to collate and analyze the data, draft and revise the manuscript according to the Cochrane Handbook. Adilaabudusalamu contributed to screen and collaborate on data analysis. JY contributed to analyze the data and interpret the results. YS contributed to define the research theme, analyze the data and interpret the results, revise the manuscript, and was responsible for the layout and use of funds. All the authors have read and approved the final manuscript and reported no declarations of interest.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, K., Abudusalamu, A., Yang, J. et al. Effectiveness of early enteral feeding on health outcomes in preterm infants: an overview of systematic reviews. Eur J Clin Nutr 77, 628–636 (2023). https://doi.org/10.1038/s41430-022-01223-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-022-01223-1
