
Abstract
Background
We characterized age at diagnosis and estimated sex differences for lung cancer and its histological subtypes among individuals who never smoke.
Methods
We analyzed the distribution of age at lung cancer diagnosis in 33,793 individuals across 8 cohort studies and two national registries from East Asia, the United States (US) and the United Kingdom (UK). Student’s t-tests were used to assess the study population differences (Δ years) in age at diagnosis comparing females and males who never smoke across subgroups defined by race/ethnicity, geographic location, and histological subtypes.
Results
We found that among Chinese individuals diagnosed with lung cancer who never smoke, females were diagnosed with lung cancer younger than males in the Taiwan Cancer Registry (n = 29,832) (Δ years = −2.2 (95% confidence interval (CI):−2.5, −1.9), in Shanghai (n = 1049) (Δ years = −1.6 (95% CI:-2.9, −0.3), and in Sutter Health and Kaiser Permanente Hawaiʽi in the US (n = 82) (Δ years = −11.3 (95% CI: −17.7, −4.9). While there was a suggestion of similar patterns in African American and non-Hispanic White individuals. the estimated differences were not consistent across studies and were not statistically significant.
Conclusions
We found evidence of sex differences for age at lung cancer diagnosis among individuals who never smoke.
Similar content being viewed by others

Introduction
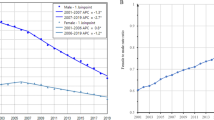
Lung cancer is a significant global health burden with an estimated 2.2 million new cases and 1.8 million deaths worldwide in 2020 [1]. While active smoking is the most prominent risk factor for lung cancer, nearly 25% of lung cancer cases diagnosed worldwide are among people who never smoke, with the proportion varying geographically [2]. It is estimated that 10% of lung cancer cases in the United States (US) and as high as 50% in Asia are diagnosed among patients who never smoke, with higher proportions among female populations [3]. Among lung cancer patients who never smoke, lung adenocarcinoma (LUAD), which originates in the mucous-producing epithelial lining of the lung, is the most commonly diagnosed histological subtype [2, 4], with a higher proportion among females compared to males [4, 5].
Lung cancer is a highly fatal disease, with an overall 5-year survival rate of 22.9% in the US from 2012 to 2018, which ranges from 61.2% for early (localized) stage to as low as 7% for distant stage (metastasized) [6]. Age at diagnosis is an important prognostic factor that influences clinical treatment decisions and survival of lung cancer patients [7,8,9,10,11], as those with younger age at diagnosis often present with earlier tumor stages and benefit from early targeted treatment [12, 13]. According to the Surveillance, Epidemiology, and End Results Program (SEER), the median age at lung cancer diagnosis in the US is 71 years. However, evidence from cancer registries, patient medical records, and case-series analyses suggest differences in age at lung cancer diagnosis between subpopulations defined by smoking status, race and ethnicity, and geographic location [14,15,16,17,18,19,20,21,22,23,24]. Notably, some studies have reported differences with females more often diagnosed [25, 26] at younger ages [27,28,29], with LUAD [28, 30, 31], and with earlier tumor stage at diagnosis, compared to males [25, 26]. However, the existence of sex differences in age at lung cancer diagnosis among individuals who never smoke, which may contribute to lung cancer-related disparities between females and males [25, 26, 28,29,30,31], are unclear.
Given the importance of age at diagnosis for disease prognosis, clinical treatment decisions, and survival of lung cancer patients [6,7,8,9,10], we conducted an international study to characterize age at diagnosis for lung cancer patients who never smoke, as well as examined sex differences by histological subtypes (i.e., LUAD and squamous cell carcinoma [SCC]) and race and ethnicity.
Methods
Study Design
The lung cancer case ascertainment procedures and criteria, as well as histological subtype confirmation for each participating study have been described in detail elsewhere [24, 32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. We received data on age at lung cancer diagnosis among patients who never smoke by self-reported sex, race and ethnicity, as well as histology and SEER tumor stage (when available) from 8 cohort studies and two population-based cancer registries. Individual-level data were provided for 1,571 lung cancer patients who never smoke from the Shanghai Women’s Health Study (SWHS; n = 760) [52], the Shanghai Men’s Health Study (SMHS; n = 289) [40], the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial (n = 39) [41], and the UK Biobank (n = 483) [42, 43]. Summary statistics (i.e., mean, standard deviation (SD), min, max, median, 25th and 75th percentile) were provided for 32,222 lung cancer cases who never smoke from the Taiwan Cancer Registry (TCR) [32, 33] population study (n = 29,832), the Multiethnic Cohort Study (MEC; n = 578) [34], the Cancer Prevention Study-II Nutrition Cohort and Cancer Prevention Study-3 (CPSII, n = 365; CPS-3, n = 64) [35, 36], Sutter Health of Northern California and Kaiser Permanente Hawaiʽi (STKP; n = 515) [24, 37], the Southern Community Cohort Study (SCCS; n = 138) [38, 39], and the National Cancer Center Japan (NCC; n = 730) [53]. In total, we received data for 33,793 lung cancer cases.
Each participating study obtained its own institutional review board approval. Sutter Health of Northern California and Kaiser Permanente Hawaiʽi received waiver of consent, and consent for participants in MEC was received with receipt of baseline questionnaire. All remaining participants provided written or electronic informed consent.
Statistical analyses
In each of the participating studies, we characterized the distribution of age at diagnosis of lung cancer and its histological subtypes (i.e., LUAD and SCC) among individuals who never smoke by self-reported biological sex (i.e., male, female), race and ethnicity (i.e., Chinese and Japanese individuals living in Asia, Chinese and Japanese individuals living in the US, non-Hispanic White and African American individuals living in the US, and White individuals living in the UK), and SEER tumor stage (i.e., local, regional, distant) for studies with available data. Within each participating study, we estimated differences in average age at diagnosis of overall lung cancer, LUAD, and SCC between females and males who never smoke and tested the differences using Student’s t-tests. The differences in average age at diagnosis (Δ years) between females and males were then meta-analyzed across populations of similar racial and ethnic subgroup using random effects inverse variance method. All analyses were performed using the R statistical software (version 4.2.2).
Results
Information on each participating study, including study design, years of enrollment, geographical region, type of data provided, sample size and criteria for age at enrollment is shown in Table 1. Study specific and combined estimates for the difference in age at diagnosis for lung cancer comparing East Asian females and males who never smoke living in Taiwan, China, and US, overall and by histological subtype are presented in Table 2. We observed that among individuals who never smoke in TCR, a population-based registry and the largest study in our analyses, and in the SWHS and SMHS, large population-based prospective cohort studies of Chinese individuals, females were diagnosed younger than males by 2.2 years (Δ years = −2.2 (95% confidence interval (CI): −2.5, −1.88; Pdifference = 2.19 × 10−40) and 1.6 years (Δ years = −1.6 (95% CI: −2.9, −0.3; Pdifference = 0.02), respectively. We observed similar patterns in the Chinese populations living in East Asia for LUAD and SCC. Further, we found that Chinese females who never smoke living in the US from STKP were also diagnosed with overall lung cancer younger than males (Δ years = −11.3 (95% CI: −17.7, −4.9; Pdifference 5.38 x 10−4). Conversely, we observed that among Japanese individuals who never smoke living in Japan from the NCC, the age at LUAD diagnosis was older for females compared to males (Δ years = 3.3 (95% CI: 1.0, 5.6; Pdifference = 5.00 × 10-3). This pattern was further supported in Japanese individuals who never smoke living in the US from MEC, where females had a suggestive older age at LUAD diagnosis compared to males (Δ years = 2.9 (95% CI: −0.2, 6.0; Pdifference = 0.07) (Supplementary Table 1).
Study specific and combined estimates for the difference in age at diagnosis for lung cancer comparing non-Hispanic White females and males living in the US and White females and males living in the UK overall and by histological subtype are presented in Table 3. Similar to the Chinese population, we observed that non-Hispanic White females living in the US from CPSII were diagnosed with overall lung cancer younger than males (Δ years = −2.0 (95% CI: −3.7, −0.3; Pdifference = 0.02). While less pronounced, the meta-analysis across the 7 studies with non-Hispanic White and White individuals who never smoke living in the US and UK suggested that females had younger age at diagnosis compared to males for overall lung cancer (Δ yearscombined = −0.8 (95% CI: −1.9, 0.4; Pmeta-analysis = 0.18) and LUAD (Δ yearscombined = −1.1 (95% CI: −2.4, 0.1; Pmeta-analysis = 0.08); however, the findings were not consistent across studies and were not statistically significant. We further found that among African American individuals who never smoke in the two studies with available data (SCCS and MEC), females had younger age at lung cancer diagnosis compared to males (Δ yearscombined = −1.0 (95% CI: −4.0, 1.9; Pmeta-analysis = 0.49); however, the sample size was limited and the findings were not statistically significant (Supplementary Table 2).
In additional analyses examining differences in age at lung cancer diagnosis across tumor stages (local, regional, distant) for subjects in TCR, we found among individuals who never smoke, females were diagnosed with lung cancer younger than males for local (Δ years = −1.8 (95% CI: −2.4, −1.2; Pdifference = 1.68 × 10−8), regional (Δ years = −3.1 (95% CI: −4.1, −2.2; Pdifference = 2.18 × 10−10), and distant tumor stage (Δ years = −1.9 (95% CI: −2.31, −1.49; Pdifference = 1.14 × 10-20). Similar patterns were found for LUAD and SCC in analyses stratified by tumor stage (Supplementary Table 3).
Discussion
We conducted a large-scale study to characterize age at diagnosis for lung cancer and its histological subtypes, comparing females versus males by race and ethnicity. We analyzed summary and individual-level data from 33,793 lung cancer cases who never smoke in 10 studies from Taiwan, China, Japan, US, and UK. Overall, we found that among Chinese individuals living in East Asia and in the US, females were diagnosed with lung cancer younger than males. While there was a suggestion of similar patterns in African American and non-Hispanic White individuals living in the US and White individuals living in the UK, the estimated differences were not consistent across studies and were not statistically significant. These findings were consistent across histological subtypes, as well as tumor stages. An exception to this pattern was found among Japanese individuals who never smoke living in Japan and in the US, where females were diagnosed with lung cancer at a later age compared to males.
The demographic makeup of lung cancer has substantially shifted over the last few decades, with the proportion of never-smoking lung cancer increasing due to the decline in smoking prevalence, and sex differences in the epidemiology, pathogenesis and outcomes of the disease have become apparent [29, 54]. Factors that may contribute to sex differences in the characteristics of lung cancer, such as age at diagnosis, may include screening, as well as endogenous and exogenous exposures. A study in the US on gender differences in cancer screening behaviors have showed that women are more likely than men to have more frequent contact with health care providers and seek cancer screening [55], which may on average lead to an earlier diagnosis. However, given that our study focused on individuals who never smoke, a population for which there are no established lung cancer screening guidelines, we suspect that screening behavior had limited impact on the observed differences. Further, we found that females had consistent younger age at lung cancer diagnoses across different tumor stages, suggesting that additional factors may impact the observed sex differences.
Endogenous factors that potentially contribute to sex differences in age at diagnosis among lung cancer in patients who never smoke include the distribution of lung cancer histological subtypes, tumor mutations and genetic susceptibility [44, 45, 56,57,58,59]. For example, females are at an increased risk compared to males of developing lung cancer with a driver mutation, such as the epidermal growth factor receptor (EGFR) [60,61,62]. However, studies have found that lung cancer patients with an EGFR mutation are more likely to have an older age at diagnosis [63], and therefore may not be the reason for our findings. Additionally, estrogen may also lead to sex differences in lung cancer. While research on this topic is ongoing, estrogen receptors have been shown to be overexpressed in many lung cancers [61, 64] and studies have linked the use of hormone replacement therapy [65] and reproductive factors to the risk of lung cancer in females [66,67,68].
Exogenous factors, such as environmental and occupational exposure profiles may also impact sex differences in lung cancer diagnosis. For example, lung cancer risk factors among East Asian individuals who never smoke include indoor solid fuel combustion, fumes from cooking oil, outdoor air pollution, diesel exhaust, workplace exposures, and secondhand smoke [2, 4, 69,70,71,72,73,74]. Notably, East Asian women are more likely to be exposed to indoor air pollution from fuel and cooking oil early in life [75], as well as to spousal secondhand smoke. Conversely, male individuals in East Asia are more likely to be exposed to occupational sources of air pollution, such as secondhand smoke in the work environment. Despite potential differences between East Asian individuals living in Asia and the US, we found similar patterns of age at diagnoses, which could suggest similar exposures or genetic predisposition.
Our study had notable strengths. We compiled a large pool of ethnically and geographically diverse data of lung cancer cases who never smoke, which allowed for comparison of age at lung cancer diagnosis by sex, within subpopulations defined by race and ethnicity, histological subtype, and tumor stage. Importantly, we obtained data from the TCR, one of the largest sources of lung cancer data for patients who never smoke in the world, which included information on tumor stage. Further, we obtained data from the CPSII, MEC and Sutter Health / Kaiser Permanente- Hawaiʽi, which greatly improved the representation in our study of Chinese and Japanese individuals living in the US.
Our study had some limitations and interpretation of our results should be done with caution. This study was intended primarily as a descriptive analysis as we could not account or adjust for potential sources of confounding or heterogeneity that potentially drive differences in age at diagnosis across the participating studies and their subgroups. Given the heterogeneity among the participating studies, we opted not to calculate a combined weighted average age at diagnosis across studies, as this would not be meaningful. Further, our analyses were primarily conducted in cohort studies, which do not represent the general population. Despite these caveats, a consistently younger age at diagnosis among females versus males was observed across multiple studies, including a large population-based registry, as well as across histological subtypes and tumor stage. Additionally, although some data on African American individuals were obtained from SCCS, MEC, and CPSII, we did not have sufficient case numbers to comprehensively analyze this population and its subgroups. Future studies that include larger African American, as well as Hispanic populations will be needed to accurately characterize differences in age at diagnosis.
In summary, we characterized the average age at diagnosis for lung cancer and its subtypes among patients who never smoke in a comprehensive analysis of 33,793 lung cancer patients from the US, China, Taiwan, Japan and the UK. We found that, among individuals who never smoke, females had a younger age at diagnosis compared to males, which was especially apparent among Chinese individuals living in Taiwan and Mainland China, as well as among Chinese individuals living in the US. Future studies are needed to elucidate the potential reasons for these observed differences.
Data availability
Summary data can be made available upon request.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2022;71:209–49. https://onlinelibrary.wiley.com/doi/full/10.3322/caac.21660
Sun S, Schiller JH, Gazdar AF. Lung cancer in never smokers — a different disease. Nat Rev Cancer. 2018;7:778–90. http://www.nature.com/articles/nrc2190
Cho J, Choi SM, Lee J, Lee CH, Lee SM, Kim DW, et al. Proportion and clinical features of never-smokers with non-small cell lung cancer. Chin J Cancer. 2022;36:20.
Subramanian J, Govindan R. Lung cancer in never smokers: a review. J Clin Oncol. 2018;25:561–70. http://ascopubs.org/doi/10.1200/JCO.2006.06.8015
Toh CK, Wong EH, Lim WT, Leong SS, Fong KW, Wee J, et al. The impact of smoking status on the behavior and survival outcome of patients with advanced non-small cell lung cancer: a retrospective analysis. Chest. 2022;126:1750–6. https://pubmed.ncbi.nlm.nih.gov/15596669/
Lung and Bronchus Cancer (2022) — Cancer Stat Facts Dec. https://seer.cancer.gov/statfacts/html/lungb.html
Ramsey SD, Howlader N, Etzioni RD, Donato B. Chemotherapy use, outcomes, and costs for older persons with advanced non-small-cell lung cancer: Evidence from surveillance, epidemiology and end results-medicare. J Clin Oncol. 2004;22:4971–8.
Sacher AG, Dahlberg SE, Heng J, Mach S, Jänne PA, Oxnard GR. Association Between Younger Age and Targetable Genomic Alterations and Prognosis in Non-Small-Cell Lung Cancer. JAMA Oncol. 2022;2:313–20. https://pubmed.ncbi.nlm.nih.gov/26720421/
Chen T, Zhou F, Jiang W, Mao R, Zheng H, Qin L, et al. Age at diagnosis is a heterogeneous factor for non-small cell lung cancer patients. J Thorac Dis. 2022;11:2251–66. https://pubmed.ncbi.nlm.nih.gov/31372262/
Liu M, Cai X, Yu W, Lv C, Fu X. Clinical significance of age at diagnosis among young non-small cell lung cancer patients under 40 years old: a population-based study. Oncotarget. 2022;6:44963.
Tas F, Ciftci R, Kilic L, Karabulut S. Age is a prognostic factor affecting survival in lung cancer patients. Oncol Lett. 2022;6:1507–13. https://pubmed.ncbi.nlm.nih.gov/24179550/
Flores R, Patel P, Alpert N, Pyenson B, Taioli E. Association of Stage Shift and Population Mortality Among Patients With Non–Small Cell Lung Cancer. JAMA Netw Open. 2022;4:e2137508–e2137508. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2787247
Knight SB, Crosbie PA, Balata H, Chudziak J, Hussell T, Dive C. Progress and prospects of early detection in lung cancer. Open Biol. 2022;7:170070 https://pubmed.ncbi.nlm.nih.gov/28878044/
Campling BG, Ye Z, Lai Y, Li L, Bar-Ad V, Werner-Wasik M, et al. Disparity in age at lung cancer diagnosis between current and former smokers. J Cancer Res Clin Oncol. 2022;145:1243–51. https://pubmed.ncbi.nlm.nih.gov/30830294/
Campling BG, Collins BN, Algazy KM, Schnoll RA, Lam M. Spontaneous smoking cessation before lung cancer diagnosis. J Thorac Oncol. 2022;6:517–24. https://pubmed.ncbi.nlm.nih.gov/21258255/
Toh CK, Gao F, Lim WT, Leong SS, Fong KW, Yap SP, et al. Never-smokers with lung cancer: epidemiologic evidence of a distinct disease entity. J Clin Oncol. 2022;24:2245–51. https://pubmed.ncbi.nlm.nih.gov/16710022/
Bhatt VR, Batra R, Silberstein PT, Loberiza FR, Ganti AK. Effect of smoking on survival from non-small cell lung cancer: a retrospective Veterans’ Affairs Central Cancer Registry (VACCR) cohort analysis. Med Oncol. 2022;32:1–6. https://pubmed.ncbi.nlm.nih.gov/25429831/
Ferketich AK, Niland JC, Mamet R, Zornosa C, D’Amico TA, Ettinger DS, et al. Smoking status and survival in the national comprehensive cancer network non-small cell lung cancer cohort. Cancer. 2022;119:847–53. https://pubmed.ncbi.nlm.nih.gov/23023590/
Yang P, Allen MS, Aubry MC, Wampfler JA, Marks RS, Edell ES, et al. Clinical features of 5,628 primary lung cancer patients: experience at Mayo Clinic from 1997 to 2003. Chest. 2022;128:452–62. https://pubmed.ncbi.nlm.nih.gov/16002972/
Korpanty GJ, Kamel-Reid S, Pintilie M, Hwang DM, Zer A, Liu G, et al. Lung cancer in never smokers from the Princess Margaret Cancer Centre. Oncotarget. 2022;9:22559.
Etzel CJ, Lu M, Merriman K, Liu M, Vaporciyan A, Spitz MR. An epidemiologic study of early onset lung cancer. Lung Cancer. 2022;52:129–34. https://pubmed.ncbi.nlm.nih.gov/16564601/
Kawaguchi T, Matsumura A, Fukai S, Tamura A, Saito R, Zell JA, et al. Japanese ethnicity compared with Caucasian ethnicity and never-smoking status are independent favorable prognostic factors for overall survival in non-small cell lung cancer: a collaborative epidemiologic study of the National Hospital Organization Study Group for Lung Cancer (NHSGLC) in Japan and a Southern California Regional Cancer Registry databases. J Thorac Oncol. 2022;5:1001–10. https://pubmed.ncbi.nlm.nih.gov/20526205/
Ou SHI, Ziogas A, Zell JA. A comparison study of clinicopathologic characteristics of Southern California Asian American Non-small Cell Lung Cancer (NSCLC) patients by smoking status. J Thorac Oncol. 2022;5:158–68. https://pubmed.ncbi.nlm.nih.gov/20040896/
Derouen MC, Canchola AJ, Thompson CA, Jin A, Nie S, Wong C, et al. Incidence of Lung Cancer Among Never-Smoking Asian American, Native Hawaiian, and Pacific Islander Females. J Natl Cancer Inst. 2022;114:78–86. https://pubmed.ncbi.nlm.nih.gov/34345919/
Sakurai H, Asamura H, Goya T, Eguchi K, Nakanishi Y, Sawabata N, et al. Survival differences by gender for resected non-small cell lung cancer: a retrospective analysis of 12,509 cases in a Japanese Lung Cancer Registry study. J Thorac Oncol. 2022;5:1594–601. https://pubmed.ncbi.nlm.nih.gov/20736855/
Sagerup CMT, Småstuen M, Johannesen TB, Helland Å, Brustugun OT. Sex-specific trends in lung cancer incidence and survival: a population study of 40,118 cases. Thorax. 2022;66:301–7. https://pubmed.ncbi.nlm.nih.gov/21199818/
Fidler-Benaoudia MM, Torre LA, Bray F, Ferlay J, Jemal A. Lung cancer incidence in young women vs. young men: A systematic analysis in 40 countries. Int J Cancer. 2022;147:811–9. https://pubmed.ncbi.nlm.nih.gov/32020598/
Jemal A, Miller KD, Ma J, Siegel RL, Fedewa SA, Islami F, et al. Higher Lung Cancer Incidence in Young Women Than Young Men in the United States. N. Engl J Med. 2022;378:1999–2009. https://www.nejm.org/doi/full/10.1056/nejmoa1715907
Ragavan M, Patel MI, Weatherald J, Humbert M, Riha R. The evolving landscape of sex-based differences in lung cancer: a distinct disease in women. Eur Respir Rev. 2022;31:210100 https://err.ersjournals.com/content/31/163/210100
Infante MV, Cardillo G. Lung cancer screening in never-smokers: facts and remaining issues. Eur Respir J. 2022;56:2002949 https://erj.ersjournals.com/content/56/5/2002949
Siegel DA, Fedewa SA, Henley SJ, Pollack LA, Jemal A. Proportion of Never Smokers Among Men and Women With Lung Cancer in 7 US States. JAMA Oncol. 2022;7:302–4. https://jamanetwork.com/journals/jamaoncology/fullarticle/2773380
Chiang CJ, You SL, Chen CJ, Yang YW, Lo WC, Lai MS. Quality assessment and improvement of nationwide cancer registration system in Taiwan: a review. Jpn J Clin Oncol. 2022;45:291–6. https://pubmed.ncbi.nlm.nih.gov/25601947/
Kao WH, Hong JH, See LC, Yu HP, Hsu J, te, Chou IJ, et al. Validity of cancer diagnosis in the National Health Insurance database compared with the linked National Cancer Registry in Taiwan. Pharmacoepidemiol Drug Saf. 2022;27:1060–6. https://pubmed.ncbi.nlm.nih.gov/28815803/
Stram DO, Park SL, Haiman CA, Murphy SE, Patel Y, Hecht SS, et al. Racial/Ethnic Differences in Lung Cancer Incidence in the Multiethnic Cohort Study: An Update. J Natl Cancer Inst. 2022;111:811–9. https://pubmed.ncbi.nlm.nih.gov/30698722/
Calle EE, Rodriguez C, Jacobs EJ, Almon ML, Chao A, McCullough ML, et al. The American Cancer Society Cancer Prevention Study II Nutrition Cohort: rationale, study design, and baseline characteristics. Cancer. 2022;94:500–11. https://pubmed.ncbi.nlm.nih.gov/11900235/
Patel AV, Jacobs EJ, Dudas DM, Briggs PJ, Lichtman CJ, Bain EB, et al. The American Cancer Society’s Cancer Prevention Study 3 (CPS-3): Recruitment, study design, and baseline characteristics. Cancer. 2022;123:2014–24. https://pubmed.ncbi.nlm.nih.gov/28171707/
DeRouen MC, Thompson CA, Canchola AJ, Jin A, Nie S, Wong C, et al. Integrating Electronic Health Record, Cancer Registry, and Geospatial Data to Study Lung Cancer in Asian American, Native Hawaiian, and Pacific Islander Ethnic Groups. Cancer Epidemiol Biomark Prev. 2022;30:1506–16. https://pubmed.ncbi.nlm.nih.gov/34001502/
Signorello LB, Blot WJ. The Southern Community Cohort Study: investigating health disparities. J Health Care Poor Underserved. 2022;21:26–37. https://pubmed.ncbi.nlm.nih.gov/20173283/
Shu X, Yu D, Shu XO, Munro HM, Zheng W, Blot WJ. Investigating the associations of glycemic load and glycemic index with lung cancer risk in the Southern Community Cohort Study. Cancer Causes Control. 2022;31:1069.
Shu XO, Li H, Yang G, Gao J, Cai H, Takata Y, et al. Cohort Profile: The Shanghai Men’s Health Study. Int J Epidemiol. 2022;44:810–8. https://pubmed.ncbi.nlm.nih.gov/25733578/
Seow WJ, Cawthon RM, Purdue MP, Hu W, Gao YT, Huang WY, et al. Telomere length in white blood cell DNA and lung cancer: a pooled analysis of three prospective cohorts. Cancer Res. 2022;74:4090.
Wong JYY, Jones RR, Breeze C, Blechter B, Rothman N, Hu W, et al. Commute patterns, residential traffic-related air pollution, and lung cancer risk in the prospective UK Biobank cohort study. Environ Int. 2022;155:106698 https://pubmed.ncbi.nlm.nih.gov/34139591/
Wong JYY, Bassig BA, Loftfield E, Hu W, Freedman ND, Ji BT, et al. White Blood Cell Count and Risk of Incident Lung Cancer in the UK Biobank. JNCI Cancer Spectr. 2022;4:pkz102 https://pubmed.ncbi.nlm.nih.gov/33313477/
Seow WJ, Matsuo K, Hsiung CA, Shiraishi K, Song M, NamKim H, et al. Association between GWAS-identified lung adenocarcinoma susceptibility loci and EGFR mutations in never-smoking Asian women, and comparison with findings from Western populations. Hum Mol Genet. 2017;26:454–65.
Lan Q, Hsiung CA, Matsuo K, Hong YC, Seow A, Wang Z, et al. Genome-wide association analysis identifies new lung cancer susceptibility loci in never-smoking women in Asia. Nat Genet. 2012;44:1330–5.
Wang Z, Seow WJ, Shiraishi K, Hsiung CA, Matsuo K, Liu J, et al. Meta-analysis of genome-wide association studies identifies multiple lung cancer susceptibility loci in never-smoking Asian women. Hum Mol Genet. 2018;25:620–9. http://www.ncbi.nlm.nih.gov/pubmed/26732429
Andriole GL, Levin DL, Crawford ED, Gelmann EP, Pinsky PF, Chia D, et al. Prostate cancer screening in the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial: Findings from the initial screening round of a randomized trial. J Natl Cancer Inst. 2022;97:433–8. https://experts.arizona.edu/en/publications/prostate-cancer-screening-in-the-prostate-lung-colorectal-and-ova
Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am J Epidemiol. 2022;186:1026–34. https://pubmed.ncbi.nlm.nih.gov/28641372/
Sudlow C, Gallacher J, Allen N, Beral V, Burton P, Danesh J, et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2022;12:e1001779 https://pubmed.ncbi.nlm.nih.gov/25826379/
de Koning HJ, van der Aalst CM, de Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl J Med. 2022;382:503–13. https://pubmed.ncbi.nlm.nih.gov/31995683/
Kolonel LN, Henderson BE, Hankin JH, Nomura AMY, Wilkens LR, Pike MC, et al. A Multiethnic Cohort in Hawaii and Los Angeles: Baseline Characteristics. Am J Epidemiol. 2022;151:346.
Zheng W, Chow WH, Yang G, Jin F, Rothman N, Blair A, et al. The Shanghai Women’s Health Study: Rationale, Study Design, and Baseline Characteristics. Am J Epidemiol. 2021;162:1123–31. http://academic.oup.com/aje/article/162/11/1123/185210/The-Shanghai-Womens-Health-Study-Rationale-Study
National Cancer Center Japan (2022) | National Cancer Center Japan. https://www.ncc.go.jp/en/index.html
Pelosof L, Ahn C, Gao A, Horn L, Madrigales A, Cox J, et al. Proportion of Never-Smoker Non–Small Cell Lung Cancer Patients at Three Diverse Institutions. JNCI J Natl Cancer Inst. 2022;109:djw295.
Davis JL, Buchanan KL, Katz RV, Green BL. Gender differences in cancer screening beliefs, behaviors, and willingness to participate: Implications for health promotion. Am J Mens Health. 2022;6:211.
Hung RJ, Spitz MR, Houlston RS, Schwartz AG, Field JK, Ying J, et al. Lung Cancer Risk in Never-Smokers of European Descent is Associated With Genetic Variation in the 5p15.33 TERT-CLPTM1Ll Region. J Thorac Oncol. 2022;14:1360–9. https://pubmed.ncbi.nlm.nih.gov/31009812/
Li Y, Xiao X, Li J, Byun J, Cheng C, Bossé Y, et al. Genome-wide interaction analysis identified low-frequency variants with sex disparity in lung cancer risk. Hum Mol Genet. 2022;31:2831.
Gabriel ACDSAG, Atkins JR, Penha RCC, Smith-Byrne K, Gaborieau V, Voegele C, et al. Genetic Analysis of Lung Cancer and the Germline Impact on Somatic Mutation Burden. J Natl Cancer Inst. 2022;114:1159–66. https://pubmed.ncbi.nlm.nih.gov/35511172/
Byun J, Han Y, Li Y, Xia J, Long E, Choi J, et al. Cross-ancestry genome-wide meta-analysis of 61,047 cases and 947,237 controls identifies new susceptibility loci contributing to lung cancer. Nat Genet. 2022;54:1167–77. https://pubmed.ncbi.nlm.nih.gov/35915169/
Yim SH, Chung YJ. Molecular Epidemiology of Female Lung Cancer. Cancers. 2022;3:1861–76. https://www.mdpi.com/2072-6694/3/2/1861/htm
Berardi R, Verdecchia L, Paolo MD, Giampieri R, Scartozzi M, Pierantoni C, et al. Women and lung cancer: clinical and molecular profiling as a determinate for treatment decisions: a literature review. Crit Rev Oncol Hematol. 2022;69:223–36. https://pubmed.ncbi.nlm.nih.gov/18722785/
MacRosty CR, Rivera MP. Lung Cancer in Women: A Modern Epidemic. Clin Chest Med. 2022;41:53–65. https://pubmed.ncbi.nlm.nih.gov/32008629/
Wu SG, Chang YL, Yu CJ, Yang PC, Shih JY. Lung adenocarcinoma patients of young age have lower EGFR mutation rate and poorer efficacy of EGFR tyrosine kinase inhibitors. ERJ Open Res. 2023;3:00092–2016. https://openres.ersjournals.com/content/3/3/00092-2016
Pirie K, Peto R, Green J, Reeves GK, Beral V. Lung cancer in never smokers in the UK Million Women Study. Int J Cancer. 2022;139:347.
Greiser CM, Greiser EM, Dören M.Menopausal hormone therapy and risk of lung cancer.Sys Rev Meta-Anal. 2022;65:198–204. https://pubmed.ncbi.nlm.nih.gov/20031346/.
Zhang Y, Yin Z, Shen L, Wan Y, Zhou B. Menstrual factors, reproductive factors and lung cancer risk: a meta-analysis. Zhongguo Fei Ai Za Zhi. 2018;15:701–19. http://www.ncbi.nlm.nih.gov/pubmed/23249716
Weiss JM, Lacey JV, Shu XO, Ji BT, Hou L, Yang G, et al. Menstrual and reproductive factors in association with lung cancer in female lifetime nonsmokers. Am J Epidemiol. 2018;168:1319–25. http://www.ncbi.nlm.nih.gov/pubmed/18849300
Seow A, Koh WP, Wang R, Lee HP, Yu MC. Reproductive variables, soy intake, and lung cancer risk among nonsmoking women in the Singapore Chinese Health Study. Cancer Epidemiol Biomark Prev. 2018;18:821–7. http://www.ncbi.nlm.nih.gov/pubmed/19240237
Barone-Adesi F, Chapman RS, Silverman DT, He X, Hu W, Vermeulen R, et al. Risk of lung cancer associated with domestic use of coal in Xuanwei, China: Retrospective cohort study. BMJ (Online). 2021;345:e5414 https://pubmed.ncbi.nlm.nih.gov/22936785/
Myers R, Brauer M, Dummer T, Atkar-Khattra S, Yee J, Melosky B, et al. High-Ambient Air Pollution Exposure Among Never Smokers Versus Ever Smokers With Lung Cancer. J Thorac Oncol. 2022;16:1850–8. https://pubmed.ncbi.nlm.nih.gov/34256112/
Sisti J, Boffetta P. What proportion of lung cancer in never-smokers can be attributed to known risk factors? Int J Cancer. 2018;131:265–75. http://www.ncbi.nlm.nih.gov/pubmed/22322343
Dean Hosgood H, Boffetta P, Greenland S, Lee YCA, Mclaughlin J, Seow A, et al. In-home coal and wood use and lung cancer risk: A pooled analysis of the international lung cancer consortium. Environ Health Perspect. 2018;118:1743–7. http://www.ncbi.nlm.nih.gov/pubmed/20846923
Chen TY, Fang YH, Chen HL, Chang CH, Huang H, Chen YS, et al. Impact of cooking oil fume exposure and fume extractor use on lung cancer risk in non-smoking Han Chinese women. Sci Rep. 2022;10:1–10. https://www.nature.com/articles/s41598-020-63656-7
Ko YC, Cheng LSC, Lee CH, Huang JJ, Huang MS, Kao EL, et al. Chinese food cooking and lung cancer in women nonsmokers. Am J Epidemiol. 2022;151:140–7. https://pubmed.ncbi.nlm.nih.gov/10645816/
Wong JYY, Downward GS, Hu W, Portengen L, Seow WJ, Silverman DT, et al. Lung cancer risk by geologic coal deposits: A case–control study of female never-smokers from Xuanwei and Fuyuan, China. Int J Cancer. 2022;144:2918–27. https://onlinelibrary.wiley.com/doi/full/10.1002/ijc.32034
Acknowledgements
This study was supported by intramural funding from the National Cancer Institute, Division of Cancer Epidemiology and Genetics. TCR is supported by Taiwan’s Ministry of Health and Welfare (MOHW106-TDU-B-212–144013 (to I.S. Chang), MOHW107-TDU-B-212–114026 (to I.S. Chang)) and by Taiwan’s National Health Research Institutes (NHRI-PH-110-GP-01 (to C.A. Hsiung)). The SWHS (UM1CA173640 to W Zheng), SMHS (UM1CA182910 to X-O, Shu), SCCS (U01CA202979 to W Zheng) and MEC (U01CA164973 to L Le Marchand, CA Haiman and LR Wilkens) were supported by grants from the US National Cancer Institute. The American Cancer Society funds the creation, maintenance, and updating of the Cancer Prevention Study-II and Cancer Prevention Study-3 cohorts.
The datasets of the TCR analyzed in this study were provided by and analyzed in the Data Science Center, Ministry of Health and Welfare (MOHW), Taiwan.
The authors express sincere appreciation to all Cancer Prevention Study-II and Cancer Prevention Study-3 participants, and to each member of the study and biospecimen management group. The authors would like to acknowledge the contribution to this study from central cancer registries supported through the Centers for Disease Control and Prevention’s National Program of Cancer Registries and cancer registries supported by the National Cancer Institute’s Surveillance Epidemiology and End Results Program.
Author information
Authors and Affiliations
Contributions
Conceptualization: Batel Blechter, Jason Y.Y. Wong, Takashi Kohno, Iona Cheng, I-Shou Chang, Chao Agnes Hsiung, Nathaniel Rothman and Qing Lan; Formal Analysis: Batel Blechter, Jason Y.Y. Wong; Writing-original draft preparation: Batel Blechter, Jason Y.Y. Wong; Writing-review and editing: Li-Hsin Chien, Kouya Shiraishi, Xiao-Ou Shu, Qiuyin Cai, Wei Zheng, Bu-Tian Ji, Wei Hu, Mohammad L Rahman, Hsin-Fang Jiang, Fang-Yu Tsai, Wen-Yi Huang, Yu-Tang Gao, Xijing Han, Mark D. Steinwandel, Gong Yang, Yihe G. Daida, Su-Ying Liang, Scarlett L Gomez, Mindy C. DeRouen, W. Ryan Diver, Ananya G. Reddy, Alpa V. Patel, Loïc Le Marchand, Christopher Haiman, Takashi Kohno, Iona Cheng, I-Shou Chang, Chao Agnes Hsiung, Nathaniel Rothman, Qing Lan; Supervision: Takashi Kohno, Iona Cheng, I-Shou Chang, Chao Agnes Hsiung, Nathaniel Rothman, Qing Lan.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Each participating study obtained its own institutional review board approval. Sutter Health of Northern California and Kaiser Permanente Hawaiʽi received waiver of consent, and consent for participants in MEC was received with receipt of baseline questionnaire. All remaining participants provided written or electronic informed consent. This study was approved by the Institutional Review Board of National Health Research Institutes, Taiwan (EC1030707-E), which conforms to the STROBE GUIDELINE for observation studies. All the patients’ personal information was protected by encrypting their identification numbers, and all the analyses were performed in accordance with the relevant guidelines and regulations and performed in a secured area administered by the Data Science Center, Ministry of Health and Welfare, Taiwan. Only summary tables could be brought out after verification by the officials to assure that there was no leakage of personal information.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Blechter, B., Wong, J.Y.Y., Chien, LH. et al. Age at lung cancer diagnosis in females versus males who never smoke by race and ethnicity. Br J Cancer 130, 1286–1294 (2024). https://doi.org/10.1038/s41416-024-02592-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-024-02592-z
