
Abstract
Background
Imatinib is an active agent for some patients with melanoma harbouring c-KIT alterations. However, the genetic and clinical features that correlate with imatinib sensitivity are not well-defined.
Methods
We retrospectively evaluated 38 KIT-altered melanoma patients from five medical centres who received imatinib, and pooled data from prospective studies of imatinib in 92 KIT-altered melanoma patients. Baseline patient and disease characteristics, and clinical outcomes were assessed.
Results
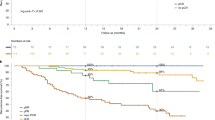
In the pooled analysis (N = 130), alterations in exons 11/13 had the highest response rates (38% and 33%); L576P (N = 23) and K642E (N = 12) mutations had ORR of 52% and 42%, respectively. ORR was 38% (mucosal), 25% (acral), and 8% (unknown-primary). PFS appeared longer in exon 11/13 vs. exon 17 alterations (median 4.3 and 4.5 vs. 1.1 months; p = 0.19), with similar superiority in OS (median 19.7 and 15.4 vs. 12.1 months; p = 0.20). By histology, median PFS was 4.5 months (mucosal), 2.7 (acral), and 5.0 (unknown-primary) [p = 0.36]. Median OS was 18.0 months (mucosal), 21.8 (acral), 11.5 (unknown-primary) [p = 0.26]. In multivariate analyses, mucosal melanoma was associated with higher PFS and exon 17 mutations were associated with reduced PFS.
Conclusion
This multicenter study highlights KIT-alterations sensitive to imatinib and augments evidence for imatinib in subsets of KIT-altered melanoma.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 24 print issues and online access
$259.00 per year
only $10.79 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


Data availability
No data are available. All data relevant to the study are included in the article or uploaded as supplemental information.
References
Curtin JA, Busam K, Pinkel D, Bastian BC. Somatic activation of KIT in distinct subtypes of melanoma. J Clin Oncol. 2006;24:4340–6.
Guo J, Si L, Kong Y, Flaherty KT, Xu X, Zhu Y, et al. Phase II, open-label, single-arm trial of imatinib mesylate in patients with metastatic melanoma harboring c-Kit mutation or amplification. J Clin Oncol. 2011;29:2327–34.
Carvajal RD, Antonescu CR, Wolchok JD, Chapman PB, Roman RA, Teitcher J, et al. KIT as a therapeutic target in metastatic melanoma. J Am Med Assoc. 2011;305:3182–90.
Hodi FS, Corless CL, Giobbie-Hurder A, Fletcher JA, Zhu M, Marino-Enriquez A, et al. Imatinib for melanomas harboring mutationally activated or amplified kit arising on mucosal, acral, and chronically sun-damaged skin. J Clin Oncol. 2013;31:3182–90
Kelly CM, Gutierrez Sainz L, Chi P. The management of metastatic GIST: current standard and investigational therapeutics. J Hematol Oncol. 2021;14:2.
Yaman B, Akalin T, Kandiloʇlu G. Clinicopathological characteristics and mutation profiling in primary cutaneous melanoma. Am J Dermatopathol. 2015;37:389–97.
Carlino MS, Haydu LE, Kakavand H, Menzies AM, Hamilton AL, Yu B, et al. Correlation of BRAF and NRAS mutation status with outcome, site of distant metastasis and response to chemotherapy in metastatic melanoma. Br J Cancer. 2014;111:1530–8.
Pracht M, Mogha A, Lespagnol A, Fautrel A, Mouchet N, le Gall F, et al. Prognostic and predictive values of oncogenic BRAF, NRAS, c-KIT and MITF in cutaneous and mucous melanoma. J Eur Acad Dermatol Venereol. 2015;29:1530–38.
Ponti G, Manfredini M, Greco S, Pellacani G, Depenni R, Tomasi A, et al. BRAF, NRAS and c-KIT advanced melanoma: clinico-pathological features, targeted-therapy strategies and survival. Anticancer Res. 2017;37:6821–8.
Beadling C, Jacobson-Dunlop E, Hodi FS, Le C, Warrick A, Patterson J, et al. KIT gene mutations and copy number in melanoma subtypes. Clin Cancer Res. 2008;14:5259.
Newell F, Wilmott JS, Johansson PA, Nones K, Addala V, Mukhopadhyay P, et al. Whole-genome sequencing of acral melanoma reveals genomic complexity and diversity. Nat Commun. 2020;11:1446–56.
Torres-Cabala CA, Wang WL, Trent J, Yang D, Chen S, Galbincea J, et al. Correlation between KIT expression and KIT mutation in melanoma: A study of 173 cases with emphasis on the acral-lentiginous/mucosal type. Mod Pathol. 2009;22:3163.
Newell F, Kong Y, Wilmott JS, Johansson PA, Ferguson PM, Cui C, et al. Whole-genome landscape of mucosal melanoma reveals diverse drivers and therapeutic targets. Nat Commun. 2019;10:3163.
Pham DM, Guhan S, Tsao H. Kit and melanoma: biological insights and clinical implications. Yonsei Med J Yonsei Univ Coll Med. 2020;61:562–71.
Woodman SE, Davies MA. Targeting KIT in melanoma: a paradigm of molecular medicine and targeted therapeutics. Biochemical Pharmacol. 2010;80:4342–9.
Heinrich MC, Corless CL, Demetri GD, Blanke CD, von Mehren M, Joensuu H, et al. Kinase mutations and imatinib response in patients with metastatic gastrointestinal stromal tumor. J Clin Oncol. 2003;21:348–57.
Steeb T, Wessely A, Petzold A, Kohl C, Erdmann M, Berking C, et al. c-Kit inhibitors for unresectable or metastatic mucosal, acral or chronically sun-damaged melanoma: a systematic review and one-arm meta-analysis. Eur J Cancer. 2021;157:1380–7.
Guo J, Carvajal RD, Dummer R, Hauschild A, Daud A, Bastian BC, et al. Efficacy and safety of nilotinib in patients with kit-mutated metastatic or inoperable melanoma: final results from the global, single-arm, phase ii team trial. Ann Oncol. 2017;28:1380–87.
Janku F, Bauer S, Shoumariyeh K, Jones RL, Spreafico A, Jennings J, et al. 1082P Phase I study of ripretinib, a broad-spectrum KIT and PDGFRA inhibitor, in patients with KIT-mutated or KIT-amplified melanoma. Ann Oncol. 2021;32:454–65.
Seifert AM, Zeng S, Zhang JQ, Kim TS, Cohen NA, Beckman MJ, et al. PD-1/PD-L1 blockade enhances T-cell activity and antitumor efficacy of imatinib in gastrointestinal stromal tumors. Clin Cancer Res. 2017;23:1094–100.
Balachandran VP, Cavnar MJ, Zeng S, Bamboat ZM, Ocuin LM, Obaid H, et al. Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido. Nat Med. 2011;17:234–8.
Yao Z, Yaeger R, Rodrik-Outmezguine VS, Tao A, Torres NM, Chang MT, et al. Tumours with class 3 BRAF mutants are sensitive to the inhibition of activated RAS. Nature. 2017;548:234–8.
Garrido MC, Bastian BC. KIT as a therapeutic target in melanoma. J Investigative Dermatol. 2010;130:20–7.
Acknowledgements
DBJ receives funding from the Susan and Luke Simons Melanoma Directorship, the James C. Bradford Melanoma Fund, and the Van Stephenson Melanoma Fund.
Author information
Authors and Affiliations
Contributions
The project was designed by DBJ and SJ. Data analysis was performed by DBJ, SJ, FY, AL. Manuscript was written by DBJ and SJ. This submission has been reviewed and approved by all authors.
Corresponding author
Ethics declarations
Competing interests
DBJ is on advisory boards or consults for BMS, Catalyst, Iovance, Jansen, Mallinckrodt, Merck, Mosaic ImmunoEngineering, Novartis, Oncosec, Pfizer, and Targovax, and receives research funding from BMS and Incyte. ANS has been on advisory boards or a consultant for Bristol-Myers Squibb, Immunocore, and Novartis and has received research funding from Bristol-Myers Squibb, Immunocore, Novartis, Xcovery, Targovax, Polaris, Pfizer, Checkmate Pharmaceuticals, and Forhorn Therapeutics. RJS has been on advisory boards or a consultant over the last 36 months for BMS, Eisai, Iovance, Merck, Novartis, OncoSec, Pfizer, and has received research funding from Amgen and Merck. RDC has been on advisory boards or a consultant for BMS, Castle Biosciences, Compugen, Foundation Medicine, Immunocore, I-Mab, Incyte, Merck, Roche/Genentech, PureTech Health, Sanofi Genzyme, Sorrento Therapeutics, Rgenix, Chimeron, and Aura Biosciences. He has received research funding from Amgen, Astellis, AstraZeneca, Bayer, Bellicum, BMS, Corvus, Eli Lilly, Immunocore, Incyte, Macrogenics, Merck, Mirati, Novartis, Pfizer, Plexxikon, and Roche/Genentech. EA, SJ, and AZW have no conflicts of interest to report.
Ethics approval and consent to participate
Institutional review board approval was received for study protocols from each institution.
Consent for publication
Not applicable.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jung, S., Armstrong, E., Wei, A.Z. et al. Clinical and genomic correlates of imatinib response in melanomas with KIT alterations. Br J Cancer 127, 1726–1732 (2022). https://doi.org/10.1038/s41416-022-01942-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-01942-z
This article is cited by
-
Genomic and clinical characterization of a familial GIST kindred intolerant to imatinib
npj Genomic Medicine (2024)
