
Abstract
Background
Preclinical studies have shown both pro- and antineoplastic effects of antihistamines. Here, we evaluated the effect of H1 antihistamines on contralateral breast cancer (CBC) risk, and whether cationic amphiphilic (CAD) antihistamines could increase the sensitivity to chemotherapy.
Methods
From the Danish Breast Cancer Group clinical database, we identified all women aged ≥20 years with a first-time diagnosis of breast cancer during 1996–2012. Information on drug use, CBC and potential confounding factors was retrieved from nationwide registries. Using Cox proportional hazard regression models, we calculated hazard ratios (HRs) and 95% confidence intervals (CIs) for CBC associated with H1-antihistamine use.
Results
We identified 52,723 patients with breast cancer with a total of 310,583 person-years of follow-up. Among them, 1444 patients developed a new primary tumour in the contralateral breast. Post-diagnosis use of H1 antihistamines (≥2 prescriptions) was not strongly associated with CBC risk (HR 1.08, 95% CI: 0.90–1.31) compared with non-use (<2 prescriptions). Use of CAD antihistamines among patients receiving chemotherapy was not associated with a decrease in CBC risk.
Conclusions
Taken together, our findings do not suggest any association of H1-antihistamine use with CBC development.
Similar content being viewed by others

Background
Accumulating evidence suggests that histamine may modulate proliferation of normal and malignant cells.1 Histamine plays a role in various physiological and pathological processes in the development and functioning of the mammary gland.2,3 Moreover, high levels of histamine have been detected in tumour tissue from breast cancer patients, and their levels of histamine in serum have been found to be higher than in healthy controls.4
Histamine 1 (H1)-receptor antihistamines, primarily used as first-line treatment for the relief of allergic symptoms, work as inverse agonists of the H1 receptor, which results in inhibition of mast cell activity and histamine release.5 The effect of H1 antihistamines on tumour development is equivocal. In the early 1990s, it was suggested that H1 antihistamines may increase the risk of breast cancer due to their structural similarity to N,N-diethyl-2-[4-(phenylmethyl) phenoxy] ethanamine (DPPE), a compound stimulating chemically induced mammary carcinoma in rodents.6,7 In contrast, during recent years, H1 antihistamines have gained interest due to reports of potential antineoplastic activity.8,9,10
To date, two epidemiological studies investigated the use of H1 antihistamines and breast cancer incidence.11,12 One study reported a slightly reduced risk,11 while the other found a null association.12 Nonetheless, the effects of H1 antihistamines on breast cancer risk may be more pronounced when studying contralateral breast cancer (CBC) risk among breast cancer survivors for whom susceptibility to breast cancer has already been proven. On the basis of studies on tamoxifen, it has been proposed that the occurrence of contralateral tumours among women with breast cancer may serve as a useful model for prevention.13 Furthermore, a subgroup of H1 antihistamines, the cationic amphiphilic drugs (CAD) antihistamines, has shown to increase the efficacy of chemotherapy.14 Adjuvant chemotherapy has previously been associated with reduced CBC risk,15,16 and this association may be more pronounced when it is administered simultaneously with CAD antihistamine use.
To increase the knowledge on whether H1 antihistamines affect breast cancer development, we examined the incidence of CBC among users of H1 antihistamines in a large cohort of Danish breast cancer survivors.
Methods
This population-based cohort study was based on data from several Danish nationwide registries, including the Danish Breast Cancer Group (DBCG) clinical database,17 the National Prescription Registry,18 the National Patient Register,19 the Danish Cancer Registry,20 the Danish Pathology Register21 and registers on Statistics Denmark22 and the Civil Registration System.23 Detailed descriptions of the registries are available in the Supplementary Material of one of our previous publications.24 Unambiguous linkage between the registries was possible by using the personal identification number assigned to all Danish residents.
Study population
The DBCG database is a nationwide, clinical database containing detailed information on nearly all women diagnosed with breast cancer in Denmark since 1977.17 We identified a cohort of women with a diagnosis of unilateral, non-metastatic breast cancer between 1996 and 2012. Breast cancer patients were eligible if they were 20 years or older at diagnosis, underwent surgery and had registered information on the laterality of the first breast cancer (n = 58,704). We excluded patients diagnosed with another malignancy (except non-melanoma skin cancer) at any time before the date of the first breast cancer diagnosis (n = 3344).
Exposure definition
We identified data on the use of H1 antihistamines (ATC = R06A) from the National Prescription Registry, a register that captures data on all prescriptions dispensed at Danish pharmacies since 1995.18 Medications administered by hospitals (during admission or supplied by the hospital), treatment centres or certain institutions are not included in the registry.18 H1 antihistamines were further grouped according to CAD structure into CAD antihistamines, non-CAD antihistamines and mixed use, respectively. Users contributed person-years to the mixed user category when they switched from CAD to non-CAD antihistamines or vice versa. The specific ATC codes are available in Supplementary Table I.
We analysed H1-antihistamine use by applying two different models. In model 1, the time-varying model, use was defined as two or more prescriptions redeemed on separate dates after the first breast cancer diagnosis, and assessed as a time-varying covariate with a 1-year lag time. This means that after diagnosis, H1-antihistamine users were regarded as non-users until 1 year after their second prescription. In this time-varying model, we further investigated H1-antihistamine use according to cumulative amount and intensity of use. Cumulative amount was assessed as the total number of defined daily doses (DDDs) filled during follow-up and categorised into tertiles of <48, 48–300 and >300 DDDs. Intensity of use was defined as the cumulative amount of DDDs divided by the number of days between the first and latest prescription, and categorised into tertiles of <0.36, 0.36–0.95 and >0.95 DDDs/day. We also evaluated the influence of timing of H1-antihistamine use by an exposure matrix of four categories: (1) no pre- or post-diagnosis use (reference group), (2) pre-diagnosis use only, (3) pre- and post-diagnosis use (continuing users) and (4) post-diagnosis use only (new users). Pre-diagnosis use was defined as two or more prescriptions redeemed on separate dates within 2 years prior to the first breast cancer diagnosis.
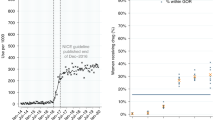
In model 2, the baseline model, we evaluated H1-antihistamine use in a fixed exposure period to investigate the potential interaction with chemotherapy. Here, H1-antihistamine use was defined as ≥1 prescription and divided into two exposure windows: (1) 3 months before and 6 months following breast cancer diagnosis (early baseline use) and (2) 7–12 months following breast cancer diagnosis (late baseline use). Early baseline use was further divided according to CAD-structure and chemotherapy use. Even though antihistamines may be used daily in certain periods, they may also be used sporadically, and then prescriptions may last for several months. Therefore, we find it possible that tablets on a prescription up to 3 months before the breast cancer diagnosis may have been taken after the diagnosis during chemotherapy. In these analyses, we excluded all women with a first breast cancer during 2007–2012, since antihistamines are often used routinely at the hospital as premedication for taxane-based chemotherapy to prevent hypersensitivity reactions or to treat such reactions, and 90% of women receiving chemotherapy from 2007 were treated with taxanes.25
Outcome and follow-up
Information on CBC was obtained from a previously established nationwide CBC database based on data from the Danish Cancer Registry20 and other registers. According to specific coding rules in the Cancer Registry, contralateral tumours with the same histology as the first breast cancer are not registered as new individual cancer records, but instead labelled as ‘bilateral breast cancer’. Therefore, we retrieved additional information on these CBCs through the original paper notification forms to the Cancer Registry for the period 1978–2003, and electronic records in the Danish Pathology Registry from 2004 and onwards,21 and only cases confirmed by these sources were accepted as CBCs in the database. Additional CBCs registered in the DBCG database only were added to obtain the highest degree of completeness (11% of all CBCs in the CBC Database).
From the Civil Registration System, we obtained information on death and emigration.23 The Danish Cancer Registry provided information on other cancer diagnoses.20 We used the National Patient Registry to identify women who received a mastectomy of the contralateral breast.19 In order to not overlook CBCs recorded after an accompanying mastectomy, we added 60 days to the date of the mastectomy, assuming that mastectomy without an accompanying CBC diagnosis within this time interval represented prophylactic mastectomy.
Follow-up in all analyses began 12 months after the first breast cancer diagnosis and ended at the occurrence of CBC, with censoring at the date of ipsilateral breast cancer, other primary malignancies (except non-melanoma skin cancer), mastectomy of the contralateral breast + 60 days (~prophylactic mastectomy), emigration and death or on December 31, 2013. Patients who developed CBC or any of the censoring outcomes within 12 months following the first breast cancer diagnosis were excluded (n = 2637).
Information on potential confounders
We based the a priori selection of confounders on knowledge from the literature and availability in the nationwide registers. Information on age at diagnosis, year of diagnosis (1996–2000; 2001–2004; 2005–2008; 2009–2012), lobular histology (yes/no), oestrogen receptor (ER) status (positive; negative; unknown), lymph node status (positive; negative; unknown) and treatment modality of the first primary breast cancer was obtained from the DBCG Database.17 For treatment, we used an intention-to-treat variable, representing the prescribed treatment according to DBCG’s guidelines, and categorised it using a matrix combining endocrine, chemo- and radiation therapy (nine categories: endocrine therapy only; chemotherapy only; radiation therapy only; endocrine + chemotherapy; endocrine + radiation therapy; chemo- + radiation therapy; endocrine + chemo- + radiation therapy; no therapy; unknown). We used the National Patient Registry19 to retrieve information on diabetes, and alcohol-, tobacco- and allergy-related conditions during a period of 10 years before and until 1 year after the first breast cancer diagnosis (yes/no) (Supplementary Table I). Information on other concomitant drug use was obtained from the National Prescription Registry18 (Supplementary Table I). We included information on pre-diagnosis use of hormone-replacement therapy (≥2 prescriptions) and post-diagnosis use (≥2 prescriptions) of low-dose aspirin, high-dose aspirin, non-aspirin non-steroidal anti-inflammatory drugs (NSAID), statins, bisphosphonates, digoxin and metformin. Use of the post-diagnosis confounder drugs was modelled in the same way as H1 antihistamines in the time-varying model, and as first-year post-diagnosis use in the baseline model. Socio-economic status was measured by the highest achieved education (short: <9 years; medium: 10–12 years; high >12 years; unknown) at breast cancer diagnosis, and was obtained from the Danish Education Register at Statistics Denmark.22
Statistical analysis
We calculated the proportions of breast cancer patients within categories of the covariates at baseline according to H1-antihistamine use (≥2 prescriptions) within the first 12 months following breast cancer diagnosis. By using Cox proportional hazard regression models, we estimated age- and multivariable-adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for H1-antihistamine use and CBC. The multivariable-adjusted model included the above-mentioned confounders in addition to age at the first breast cancer diagnosis (restricted cubic spline). Time since 1 year after the first breast cancer diagnosis was used as the underlying timescale.
In the time-varying model, we investigated effect measure modification by ER status and histological subtype of the first breast cancer. Moreover, we did the analysis according to ER status of the CBC, thereby only counting ER-positive CBCs as outcomes while censoring on all other CBCs and vice versa.
In post hoc sensitivity analyses of ever vs. non-use of H1 antihistamines and stratifications of use, we (1) removed the lag time and (2) extended the lag time to 2 years. The start of follow-up was unchanged, i.e. start date was 12 months after the first breast cancer diagnosis.
In the baseline model, we stratified according to CAD structure and chemotherapy (intention to treat: yes/no).
We evaluated the influence of competing events by calculating age- and multivariable-adjusted HRs and the corresponding 95% CIs for four censoring criteria (ipsilateral breast cancer, other primary malignancies, mastectomy of the contralateral breast and death) combined as one outcome variable.
In secondary analysis, we investigated potential bias by over-the-counter (OTC) use of H1 antihistamines in a multidimensional bias analysis as described by Lash et al.26 Assuming non-differential misclassification, a tabular quantitative bias analysis model was implemented by calculating bias-adjusted rate ratios using combinations of values assigned to the sensitivity, the probability of correctly classifying an exposed individual (0.7, 0.75, 0.8, 0.85, 0.9, 0.95 and 1.0) and specificity, the probability of correctly classifying an unexposed individual (0.95, 0.96, 0.97, 0.98, 0.99 and 1.0) (Supplementary Information and Supplementary Tables IIa, IIb and IIc). The specificity in our study was the probability among the true non-users of having no record of antihistamine use in the Prescription Register and was assumed to be high (≥98%).
The assumption of proportional hazards was evaluated by testing for trends in the Schoenfeld residuals in the fully adjusted model (ever use vs. non-use). All analyses were performed using R Statistical software version 3.4.2.27
Results
This study included 52,723 patients diagnosed with breast cancer between 1996 and 2012 (Table 1). Overall, we identified 1444 patients diagnosed with a CBC over a total median follow-up of 4.8 years. Approximately 3.2% of the breast cancer patients (n = 1685) redeemed two or more H1-antihistamine prescriptions between breast cancer diagnosis and start of follow-up, and this proportion increased to 9.5% H1-antihistamine users (n = 5005) during follow-up. There were no major differences between H1-antihistamine users and non-users in the first year after breast cancer in terms of age, calendar period, main tumour characteristics and treatment of the first breast cancer (Table 1). H1-antihistamine users were more often diagnosed with comorbidities, such as smoking-related diseases and allergy-related conditions, and more likely to have used hormone-replacement therapy before diagnosis and non-aspirin NSAIDS in the first 12 months after diagnosis.
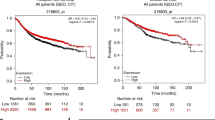
Ever use of H1 antihistamines was not strongly associated with risk of CBC (HR: 1.08, 95% CI: 0.90–1.31) (Table 2). The HRs did not change substantially by cumulative dose or CAD structure. Low- and medium-intensity H1-antihistamine use were associated with HRs close to unity, while high-intensity use was associated with a HR of CBC of 1.45 (95% CI: 1.00–2.12). Associations were similar among patients who had used H1 antihistamines exclusively after (new users) or both before and after (continuing users) the first breast cancer diagnosis, compared with non-users (Table 2). In post hoc sensitivity analyses, we found no major changes in these risk estimates when removing the lag time or extending it to 2 years (Supplementary Table III).
Stratification by ER status and histology did not substantially influence the associations (Table 3). The HRs for ER-positive and ER-negative CBC were 1.01 (95% CI: 0.81–1.27) and 1.18 (95% CI: 0.74–1.86), respectively.
The association between H1-antihistamine use and CBC at baseline is given in Table 4, divided into an early baseline period of 3 months before until 6 months after diagnosis, and a late baseline period of 7–12 months after diagnosis. We observed HRs for CBC of 1.02 (95% CI: 0.80–1.29) and 1.42 (95% CI: 1.00–1.98) for a post-diagnosis H1-antihistamine prescription being filled in the period of 3 months before and 6 months following and 7–12 months following breast cancer diagnosis, respectively. In contrast to our hypothesis, although based on small numbers, when stratifying according to chemotherapy at the first breast cancer diagnosis, the HR for CBC was slightly higher among CAD antihistamine users who received chemotherapy compared with those who did not.
In the analyses on competing events, HRs for the combined outcome were similar to those for CBC (results not shown).
The quantitative bias analysis showed that OTC use of H1 antihistamines resulted in a bias towards the null (Supplementary Table IIc). However, as the exposure prevalence of H1-antihistamine use is rare (~10%), the magnitude of the bias is mainly influenced by the specificity.
Discussion
In this population-based cohort study of breast cancer patients, we found no support of an association between use of H1 antihistamines and CBC development, neither overall nor within specific classes of antihistamines. This finding was consistent after stratification by ER status and histology of the first breast cancer. Further, we did not observe a reduction in CBC risk for CAD antihistamine use when prescribed closely in time to the course of chemotherapy.
Conflicting results have emerged on breast cancer growth from preclinical studies regarding H1 antihistamines. Originally, H1 antihistamines have long been seen as potential risk factors for cancer as their amino-ethyl group has structural similarity to DPPE.6,7 More recently, preclinical research has pointed towards potential anticancer properties. Two experimental studies by Garcia-Quiroz et al. demonstrated the capacity of astemizole, an old second-generation H1 antihistamine, to inhibit breast cancer tumour growth in vitro28 and in vivo29 by targeting Eag1, a potassium ion channel involved in tumour progression. Just recently, Fernandez-Nogueira et al. found the H1 receptor to be overexpressed in basal and HER2-targeted therapy-resistant breast cancer cells, and demonstrated that inhibition of the H1 by terfenadine led to increased cell death and a reduction in cell proliferation, although only in these two specific types of breast cancer.9 H1 antihistamines have also been shown to exert growth-inhibitory effects and promote apoptosis in vitro in other cancer cell lines.10,30,31,32
One previous study investigating breast cancer risk does to some extent support the anticancer effects found in preclinical studies. This case–control study from the United States by Kelly et al.,11 included almost 6000 cases with invasive breast cancer, and reported an OR of 0.8 (95% CI: 0.6–1.0) for regular antihistamine use and risk of breast cancer. A Canadian study by Nadalin et al. based on 3133 breast cancer cases observed no effect of antihistamine use on breast cancer risk (OR: 0.93, 95% CI: 0.81–1.06).12 The overall null associations observed in our study are in line with findings in the latter study. Both previous studies found no evidence of a duration–response pattern.11,12 Our results pointed towards a cancer-promoting effect with increasing intensity of use, though we saw no evidence of a dose–response association, so this finding may be due to chance.
The hypothesis that CAD antihistamines may improve the response to chemotherapy has been proposed already in 1993 by Hait et al., who reported on the ability of terfenadine to increase sensitisation of a multidrug-resistant human breast cancer cell line to the chemotherapeutic drug, doxorubicin.33 This finding is compatible with a recently published study from our institution, where HRs for all-cause mortality associated with use of the CAD antihistamines, loratidine and desloratidine, were found to be lower among patients diagnosed with advanced cancer who received chemotherapy compared with those who did not.14 Furthermore, they reported on the ability of low concentrations of CAD antihistamines to increase the sensitivity to chemotherapy in triple-negative breast cancer cells in vitro.14 We only had few cases of CBC who had used CAD- or non-CAD antihistamines during the period of chemotherapy administration, and therefore can neither support nor reject the hypothesis that the response to chemotherapy will be strengthened by use of CAD antihistamines.
Besides being the first to investigate the effect of H1 antihistamines in a population at high risk of breast cancer, another major strength of our study includes its nationwide approach covering the entire population of women with breast cancer in Denmark. Second, we solely used continuously updated, high-quality registries, which gave us virtually complete follow-up and accurate, prospectively collected data on H1-antihistamine use and potential confounding factors. Third, we ensured high case validity of the CBCs by combining data from the Danish Cancer Registry, the Pathology Register, the original paper notification forms and the DBCG database.
Our study, however, has some limitations. We did not have information available on OTC use of H1 antihistamines, which may have introduced exposure misclassification bias. During the study period, around 75% of the purchased H1 antihistamines were redeemed on prescription; for the main H1 antihistamines, this was 55% for cetirizine, 65% for loratadine, 97% for fexofenadine and >99% for desloratadine.34 As breast cancer patients typically are under close medical surveillance, these proportions may be even higher. Furthermore, the quantitative bias analysis suggested that the impact of the bias due to OTC use is likely to be negligible. Use of medicine at hospitals is also not recorded by the Prescription Register. To take into account that H1 antihistamines often used at the hospital to prevent or treat hypersensitivity reactions from taxane-based chemotherapy are not captured in the register, we excluded all women with the first breast cancer during 2007–2012 in our baseline model, when 90% of chemotherapy was taxane-based.25 Although our cohort included over 52,000 breast cancer patients, the number of CBC cases using H1 antihistamines was relatively limited. As a result, we were unable to examine use of the individual H1 antihistamines separately, and the risk estimates should be interpreted with caution. Lastly, residual confounding may arise from inclusion of missing values for some of the covariates in our multivariable model. Also, despite controlling for a broad range of covariates, we lacked information on some risk factors for CBC such as family history and pathogenic BRCA1/2 mutations, but we find it unlikely that these factors are associated with the use of H1 antihistamines.
In summary, the use of H1 antihistamines after breast cancer diagnosis did not seem to affect the risk of a new contralateral tumour.
References
Rivera, E. S., Cricco, G. P., Engel, N. I., Fitzsimons, C. P., Martin, G. A. & Bergoc, R. M. Histamine as an autocrine growth factor: an unusual role for a widespread mediator. Semin Cancer Biol. 10, 15–23 (2000).
Davio, C. A., Cricco, G. P., Martin, G., Fitzsimons, C. P., Bergoc, R. M. & Rivera, E. S. Effect of histamine on growth and differentiation of the rat mammary gland. Agents Actions, 41, Spec No: C115–117 (1994).
Falus, A., Pos, Z. & Darvas, Z. Histamine in normal and malignant cell proliferation. Adv. Exp. Med Biol. 709, 109–123 (2010).
Sieja, K., Stanosz, S., von Mach-Szczypinski, J., Olewniczak, S. & Stanosz, M. Concentration of histamine in serum and tissues of the primary ductal breast cancers in women. Breast (Edinb., Scotl.) 14, 236–241 (2005).
Church, M. K. & Church, D. S. Pharmacology of Antihistamines. Indian J. Dermatol 58, 219–224 (2013).
Brandes, L. J., Warrington, R. C., Arron, R. J., Bogdanovic, R. P., Fang, W., Queen, G. M. et al. Enhanced cancer growth in mice administered daily human-equivalent doses of some H1-antihistamines: predictive in vitro correlates. J. Natl Cancer Inst. 86, 770–775 (1994).
Brandes, L. J., Beecroft, W. A. & Hogg, G. R. Stimulation of in vivo tumor growth and phorbol ester-induced inflammation by N,N-diethyl-2-[4-(phenylmethyl)phenoxy] ethanamine HCl, a potent ligand for intracellular histamine receptors. Biochem. Biophys Res. Com. 179, 1297–1304 (1991).
Garcia-Quiroz, J. & Camacho, J. Astemizole: an old anti-histamine as a new promising anti-cancer drug. Anticancer Agents Med. Chem. 11, 307–314 (2011).
Fernández-Nogueira, P., Noguera-Castells, A., Fuster, G., Recalde-Percaz, L., Moragas, N., López-Plana, A. et al. Histamine receptor 1 inhibition enhances antitumor therapeutic responses through extracellular signal-regulated kinase (ERK) activation in breast cancer. Cancer Lett. 424, 70–83 (2018).
Hadzijusufovic, E., Peter, B., Gleixner, K. V., Schuch, K., Pickl, W. F., Thaiwong, T. et al. The H1-receptor antagonists terfenadine and loratadine inhibit spontaneous growth of neoplastic mast cells. Exp. Hematol. 38, 896–907 (2010).
Kelly, J. P., Rosenberg, L., Palmer, J. R., Rao, R. S., Strom, B. L., Stolley, P. D. et al. Risk of beast cancer according to use of antidepressants, phenothiazines, and antihistamines. Am. J. Epidemiol. 150, 861–868 (1999).
Nadalin, V., Cotterchio, M. & Kreiger, N. Antihistamine use and breast cancer risk. Int J. Cancer 106, 566–568 (2003).
Cuzick, J., DeCensi, A., Arun, B., Brown, P. H., Castiglione, M., Dunn, B. et al. Preventive therapy for breast cancer: a consensus statement. Lancet Oncol. 12, 496–503 (2011).
Ellegaard, A.-M., Dehlendorff, C., Vind, A. C., Anand, A., Cederkvist, L., Petersen, N. H. T. et al. Repurposing cationic amphiphilic antihistamines for cancer treatment. EBioMedicine 9, 130–139 (2016).
Langballe, R., Mellemkjaer, L., Malone, K. E., Lynch, C. F., John, E. M., Knight, J. A. et al. Systemic therapy for breast cancer and risk of subsequent contralateral breast cancer in the WECARE Study. Breast Cancer Res 18, 65 (2016).
Kramer, I., Schaapveld, M., Oldenburg, H. S. A., Sonke, G. S., McCool, D., van Leeuwen, F. E. et al. The influence of adjuvant systemic regimens on contralateral breast cancer risk and receptor subtype. J. Natl Cancer Inst. https://doi.org/10.1093/jnci/djz010 (2019).
Christiansen, P., Ejlertsen, B., Jensen, M. B. & Mouridsen, H. Danish Breast Cancer Cooperative Group. Clin. Epidemiol. 8, 445–449 (2016).
Pottegard, A., Schmidt, S. A. J., Wallach-Kildemoes, H., Sorensen, H. T., Hallas, J. & Schmidt, M. Data resource profile: The Danish National Prescription Registry. Int J. Epidemiol. 46, 798–79 (2017).
Schmidt, M., Schmidt, S. A., Sandegaard, J. L., Ehrenstein, V., Pedersen, L. & Sorensen, H. T. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin. Epidemiol. 7, 449–490 (2015).
Gjerstorff, M. L. The Danish Cancer Registry. Scand. J. Public Health 39(7 Suppl), 42–45 (2011).
Bjerregaard, B. & Larsen, O. B. The Danish Pathology Register. Scand. J. Public Health 39(7 Suppl), 72–74 (2011).
Jensen, V. M. & Rasmussen, A. W. Danish Education Registers. Scand. J. Public Health 39(7 Suppl), 91–94 (2011).
Schmidt, M., Pedersen, L. & Sorensen, H. T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 29, 541–549 (2014).
Bens, A., Friis, S., Dehlendorff, C., Jensen, M. B., Ejlertsen, B., Kroman, N. et al. Low-dose aspirin use and risk of contralateral breast cancer: a Danish nationwide cohort study. Prev. Med 116, 186–193 (2018).
Jensen, M. B., Laenkholm, A. V., Offersen, B. V., Christiansen, P., Kroman, N., Mouridsen, H. T. et al. The clinical database and implementation of treatment guidelines by the Danish Breast Cancer Cooperative Group in 2007-2016. Acta Oncol. 57, 13–18 (2018).
Lash, T. L. F., Fox, M. P. & Fink, A. K. Applying Quantitative Bias Analysis to Epidemiological Data. (Springer New York, 2009).
R. Core Team. R: A language and environment for statistical computing Vienna, Austria: R Foundation for Statistical Computing 2017. Available from: https://www.R-project.org/ (accessed 1 Sep 2017).
García-Quiroz, J., García-Becerra, R., Barrera, D., Santos, N., Avila, E., Ordaz-Rosado, D. et al. Astemizole synergizes calcitriol antiproliferative activity by inhibiting CYP24A1 and upregulating VDR: a novel approach for breast cancer therapy. PLoS ONE 7, e45063–e45063 (2012).
García-Quiroz, J., García-Becerra, R., Santos-Martínez, N., Barrera, D., Ordaz-Rosado, D., Avila, E. et al. In vivo dual targeting of the oncogenic Ether-à-go-go-1 potassium channel by calcitriol and astemizole results in enhanced antineoplastic effects in breast tumors. BMC Cancer 14, 745 (2014).
Dobbeling, U., Waeckerle-Men, Y., Zabel, F., Graf, N., Kundig, T. M. & Johansen, P. The antihistamines clemastine and desloratadine inhibit STAT3 and c-Myc activities and induce apoptosis in cutaneous T-cell lymphoma cell lines. Exp. Dermatol 22, 119–124 (2013).
Liu, J. D., Wang, Y. J., Chen, C. H., Yu, C. F., Chen, L. C., Lin, J. K. et al. Molecular mechanisms of G0/G1 cell-cycle arrest and apoptosis induced by terfenadine in human cancer cells. Mol. Carcinog. 37, 39–50 (2003).
Wang, W. T., Chen, Y. H., Hsu, J. L., Leu, W. J., Yu, C. C., Chan, S. H. et al. Terfenadine induces anti-proliferative and apoptotic activities in human hormone-refractory prostate cancer through histamine receptor-independent Mcl-1 cleavage and Bak up-regulation. Naunyn-Schmiedeberg’s Arch. Pharm. 387, 33–45 (2014).
Hait, W. N., Gesmonde, J. F., Murren, J. R., Yang, J. M., Chen, H. X. & Reiss, M. Terfenadine (Seldane): a new drug for restoring sensitivity to multidrug resistant cancer cells. Biochem Pharm. 45, 401–406 (1993).
Danish Health Data Authority. MEDSTAT 2018. Available from: http://www.medstat.dk/en (accessed 1 Oct 2018).
Author information
Authors and Affiliations
Contributions
A.B., L.M., S.F., D.C.F., N.K., B.E. and M.J. participated in writing the study protocol. M.J. and B.E. provided data for the study. A.B., L.M., S.F., C.D. and D.C.F. wrote the data analyses plan. L.M., C.D. (statistical analyses) and T.L.L. (quantitative bias analysis) provided supervision. A.B. performed the statistical analyses and drafted and coordinated the revision of the paper. All authors contributed to the critical revision of the papert.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Danish Data Protection Agency (J. no. 2012-41-0284). In Denmark, approvals from Ethical Committees are not required for register-based studies that do not involve biological samples.
Data availability
The study was approved by the Danish Data Protection Board. Data were available from the Danish Breast Cancer Group (http://www.dbcg.dk/), Statistics Denmark (https://www.dst.dk/en/TilSalg/Forskningsservice) and the Research Service of Sundhedsdatastyrelsen (https://sundhedsdatastyrelsen.dk/da/forskerservice). R-code of analyses is available from the corresponding author upon request.
Competing interests
Maj-Britt Jensen has received grants from AstraZeneca, Celgene and Novartis, and Bent Ejlertsen from NanoString, Novartis and Roche, both outside the submitted work. Lene Mellemkjær has an immediate family member employed at Novo Nordisk and has an immediate family member who owns stocks in Novo Nordisk. All other authors declared no conflicts of interest.
Funding information
This work was supported by the Danish Research Council for Independent Research [grant number 11-108395].
Additional information
Note This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution 4.0 International (CC BY 4.0).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bens, A., Dehlendorff, C., Friis, S. et al. The role of H1 antihistamines in contralateral breast cancer: a Danish nationwide cohort study. Br J Cancer 122, 1102–1108 (2020). https://doi.org/10.1038/s41416-020-0747-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-020-0747-4
