
Orthodontics has witnessed meaningful progress in recent decades with renewed interest in self-ligation; the advent, wider adoption and continued growth of aligner therapy; and the dawn of a range of surgical and non-surgical adjuncts just some of the more salient developments. While progress challenges us to adapt, to update our knowledge and understanding, and to embrace new technologies, the primacy of fundamental knowledge, careful planning and diligent oversight, and the centrality of the orthodontist rather than their tools remains unchallenged. As such, the requirement for guiding principles may be more pertinent than ever and the challenge of condensing these into digestible tips is considerable.
-
1.
Diagnosis is key. As with any other area of dentistry or medicine, safe, effective and predictable outcomes are predicated on careful diagnosis. Orthodontic diagnosis involves distillation of a range of factors spanning patient concerns, dental health, facial pattern (including skeletal and soft tissue factors, and likely growth patterns) and occlusal features. Clear objectives should be formulated on the basis of thorough diagnosis. The quality of outcome, the prospective stability of treatment, optimal function and dental health all hinge on these pivotal considerations.
-
•
The advent of three-dimensional technologies and digital planning do not obviate the need for this cornerstone of planning. Similarly, while technological advances have helped to simplify the process of treatment for adult patients in particular, none have been shown to enhance treatment outcomes, in isolation. There are also accepted weaknesses inherent in certain systems.1 It is important, therefore, that the emphasis remains on the provision of quality care with a range of possible systems founded upon careful consideration, knowledge and planning.
-
2.
Key considerations when planning antero-posterior, vertical or transverse correction. Meaningful orthodontic change should be based on the likely implications of treatment on health, aesthetics and stability. This should further be balanced with the potential unwanted effects of any proposed (non-surgical or surgical) intervention. In particular, significant arch lengthening may risk advancement of the incisors which may lead to reduced periodontal support, while also destabilising the lower incisor position.2 Moreover, the advancement of the incisors may also have aesthetic implications. Similarly, in the transverse plane, crossbite correction can be achieved by maxillary arch expansion, mandibular arch constriction or a combination of these movements. The scope for lower arch constriction is more limited. However, it can be helpful and may serve to limit the amount of required upper arch expansion, which is accepted to be particularly unstable with excessive expansion also risking periodontal compromise.
-
3.
Consideration of prospective stability from the outset.There is an appreciation that tooth movement is an insidious and ongoing process with natural change unmitigated by orthodontics and genuine relapse following treatment also a potential risk. Diligent retention has proven effective in limiting both types of change in the longer term.3,4 However, there is also a recognition that specific treatment-related changes and features of malocclusion (eg anterior open bite correction due to extrusion of the anterior dentition in the presence of skeletal discrepancy) may be particularly unstable. As such, treatment planning decisions and informed consent processes should involve due consideration of the prospective stability of treatment.5
-
4.
Detailed inter- and intra-arch treatment objectives. Typically, full occlusal correction will be planned with Class I relationships targeted. However, it is also important that bespoke planning is undertaken for each dental arch concerning the intended position for both the upper and lower anteriors. Specifically, in a Class III case, for example, correction of the incisor relationship may be achieved by retracting the lower anteriors, in isolation; by advancing the maxillary incisors alone; or with a combination of these movements.
-
5.
A hierarchy of intervention for anchorage management. Optimal anchorage management is key to the fulfilment of intra- and inter-arch objectives. While space creation may well be required in order to achieve objectives, five further key elements exist. These range from simple and predictable interventions, which involve no additional risk or burden with wide potential application to more involved procedures (Fig. 1). The more invasive options may be required in cases of isolated arches with higher anchorage demands. However, by carefully considering objectives and planning, allied to careful use of the less invasive options, it may be possible to limit or obviate the need for these approaches. The range of possible options include:
Fig. 1 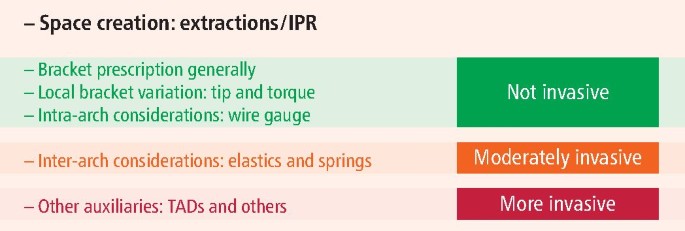
Antero-posterior anchorage control: a hierarchy
-
a.
Bracket prescription:A system appropriate for the arch should be selected. Specifically, ample palatal root torque on the maxillary incisors may be helpful in withstanding the risk of unwanted retroclination during retraction of the maxillary incisors during overjet reduction. However, palatal root torque may be unhelpful in certain Class II cases and may also increase posterior anchorage demands in the maxillary arch.
-
b.
Local bracket variations: The alteration of tip on canine brackets may be potent. In particular, reversal or artistic placement of canine brackets may be useful in limiting mesial tip expression. The latter may be unwanted in the maxillary arch in Class II and in the mandibular arch in Class III scenarios, in particular.
-
c.
Intra-arch considerations: Wire gauge can be varied particularly to titrate the amount of bucco-palatal torque expression. Classically, full torque expression of the mandibular incisors may be unwanted in Class III cases.
-
d.
Inter-arch auxiliaries: The use of inter-maxillary elastics and springs may be very effective in altering inter-arch relationships.6 Clearly, however, it is important to appreciate that these mechanics ether demand compliance, have associated patient impacts or both. They have reciprocal effects; for example, maxillary incisor retraction and lower incisor proclination with Class II elastics or flexible Class II correctors. Unwanted effects may of course be mitigated with adjunctive use of mini-implants or other compensations. However, the relative benefits of these auxiliaries in the antero-posterior plane should be balanced against these potential side effects.
-
e.
Other fixed auxiliaries: These include temporary anchorage devices (TADs) as well as palatal arches. There is equivocal evidence of benefit of trans-palatal arches; as such, TADs may well afford a more predictable means of maximal anchorage provision.7 However, failure with TADs does occur with associated risks including root contact and fracture of the screw.
-
a.

As educated practitioners, we should be trained in the use of any of these options in the correct scenario. However, with diagnostic skills and understanding, perhaps we should err on the side of keeping things as simple as possible? By exploring the least invasive options routinely, we may limit the need for more complex procedures with higher risk of failure or suboptimal compliance potentially leading to more predictable outcomes.
Predictability: that's a goal that we can all reasonably aim for, irrespective of the presenting malocclusion or the tool used to satisfy our clear and considered objectives.
References
Haouili N, Kravitz N D, Vaid N R, Ferguson D J, Makki L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop 2020; 158: 420-425.
Mills J R. The stability of the lower labial segment. A cephalometric survey. Dent Pract Dent Rec 1968; 18: 293-306.
Al-Moghrabi D, Johal A, O'Rourke N et al. Effects of fixed vs removable orthodontic retainers on stability and periodontal health: 4-year follow-up of a randomized controlled trial. Am J Orthod Dentofacial Orthop 2018; 154: 167-174.
Kocher K E, Gebistorf M C, Pandis N, Fudalej P S, Katsaros C. Survival of maxillary and mandibular bonded retainers 10 to 15 years after orthodontic treatment: a retrospective observational study. Prog Orthod 2019; doi: 10.1186/s40510-019-0279-8.
Fleming P S. Orthodontic treatment planning: can we plan for stability? Br Dent J 2021; 230: 717-721.
McNamara J A, Franchi L, McClatchey L M, Kowalski S E, Cheeseman C C. Evaluation of adolescent and adult patients treated with the Carriere Motion Class III appliance followed by fixed appliances. Angle Orthod 2021; 91: 149-156.
Sandler J, Murray A, Thiruvenkatachari B, Gutierrez R, Speight P, O'Brien K. Effectiveness of 3 methods of anchorage reinforcement for maximum anchorage in adolescents: A 3-arm multicenter randomized clinical trial. Am J Orthod Dentofacial Orthop 2014; 146: 10-20.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Fleming, P. Five tips for orthodontic practitioners. Br Dent J 231, 537–538 (2021). https://doi.org/10.1038/s41415-021-3657-9
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-021-3657-9
