
Abstract
Alzheimer’s disease (AD) risk is increased in carriers of the apolipoprotein E (APOE) ε4 allele and decreased in ε2 allele carriers compared with the ε3ε3 genotype. The aim of this study was to determine whether: the APOE genotype affects brain grey (GM) or white matter (WM) structure; and if differences exist, the age when they become apparent and whether there are differential effects by sex. We used cross-sectional magnetic resonance imaging data from ~43,000 (28,494 after pre-processing) white British cognitively healthy participants (7,446 APOE ε4 carriers) aged 45–80 years from the UK Biobank cohort and investigated image-derived phenotypes (IDPs). We observed no statistically significant effects of APOE genotype on GM structure volumes or median T2* in subcortical structures, a measure related to iron content. The volume of white matter hyperintensities differed significantly between APOE genotype groups with higher volumes in APOE ε4ε4 (effect size 0.14 standard deviations [SD]) and ε3ε4 carriers (effect size 0.04 SD) but no differences in ε2 carriers compared with ε3ε3 carriers. WM integrity measures in the dorsal (mean diffusivity [MD]) and ventral cingulum (MD and intracellular volume fraction), posterior thalamic radiation (MD and isotropic volume fraction) and sagittal stratum (MD) indicated lower integrity in APOE ε4ε4 carriers (effect sizes around 0.2–0.3 SD) and ε3ε4 (effect sizes around 0.05 SD) carriers but no differences in ε2 carriers compared with the APOE ε3ε3 genotype. Effects did not differ between men and women. APOE ε4 homozygotes had lower WM integrity specifically at older ages with a steeper decline of WM integrity from the age of 60 that corresponds to around 5 years greater “brain age”. APOE genotype affects various white matters measures, which might be indicative of preclinical AD processes. This hypothesis can be assessed in future when clinical outcomes become available.
Similar content being viewed by others

Introduction
Carriers of the apolipoprotein E gene (APOE) ε4 allele (~ 25% of white Europeans) have a higher risk of Alzheimer’s disease (AD) (odds ratio of ~3 for heterozygotes and ~15 for homozygotes) while carriers of the rarer ε2 allele have a lower AD risk (odds ratio of 0.6) compared with carriers of the most common APOE ε3ε3 genotype [1, 2]. There may be an interaction between APOE genotype and sex because only female but not male ε4 heterozygotes showed increased AD risk [2], however, this view has recently been challenged by a much larger meta-analysis [3].
Magnetic resonance imaging (MRI) can be used to identify changes in brain structure in symptomatic AD patients [4]. In studies of familial AD cases and controls, differences in cortical thickness between participants carrying autosomal dominant AD genes and non-carriers can be observed years before onset of symptoms with some regions such as the precuneus and parahippocampus showing thinning ~10 years before disease onset [5]. Therefore, changes in brain structure in healthy adults carrying APOE ε4 might be MRI biomarkers of pre-symptomatic AD that could identify potential participants for clinical trials of AD prevention or treatment before the onset of clinical symptoms, at which point interventions might be more effective [6].
Although small cross-sectional studies reported significant effects of APOE genotype on grey matter (GM) ([7], N = 65 ε4 carriers) and white matter (WM) structures ([8], N = 275 ε4 carriers), most studies of APOE genotype effects did not report significant differences ([9,10,11,12,13,14,15], N = 40-1070 ε4 carriers). In adolescents APOE genotype was not associated with differences in brain structure in some ([16, 17], N = 120–340 ε4 carriers), although not all studies ([18, 19], N = 60-310 ε4 carriers). While some studies only reported effects of APOE genotype on brain regions that are affected by early AD pathology (e.g., refs. [7, 8]), such as the hippocampus and posterior cingulate cortex and their interconnecting tracts, there are also studies that show effects on regions across the whole brain (e.g., refs. [18, 19]). However, all of these studies were likely underpowered because they were small, or aggregated data from different MRI scanners with different data acquisition protocols and data analysis methods.
To more reliably estimate differences by APOE genotype, studies of a larger number of participants scanned with identical MRI hardware and data acquisition protocols are needed. In this study, we assessed whether, in about 43,000 (28,494 after pre-processing) UK Biobank participants with MRI brain scanning with a common protocol, APOE genotype affects brain grey or white matter structure across the whole brain and if differences exist, at what age they become apparent and whether there are differential effects by sex.
Materials and methods
Study design and participants
The UK Biobank (UKB) cohort is a large prospective epidemiological study of around 0.5 million participants [20]. Between 2006 and 2010 men and women aged 40 to 69 years were recruited and data collected on their lifestyle, environment, medical history and physical measures, along with biological samples. In 2014, UKB started to collect brain, heart and body imaging data from 100,000 UKB participants [21]. Data from 43,796 UK Biobank participants with pre-processed neuroimaging data released in February 2021 were included here.
Ethical approval
UKB has ethics approval from the North West Multi-centre Research Ethics Committee (MREC), which covers the UK (for more information, see: http://www.ukbiobank.ac.uk/ethics/). Informed consent was obtained from all subjects. This project was approved by UK Biobank (8835).
Genetic data
Procedures for genotyping in the UK Biobank are described in more detail elsewhere [22] and online on http://www.ukbiobank.ac.uk/scientists-3/genetic-data. For this project, APOE genotype information was derived from the combined allelic information of two SNPs, rs423958 and rs7412. Imputed and directly genotyped SNPs were identical where both were present but more participants had complete imputed genetic information available (99.8% vs ~85% for direct genotyping), so imputed genotypes were used in all analyses.
Neuroimaging data
The neuroimaging data acquisition and pre-processing pipelines have been described previously [23, 24]. In brief, data used in this project were acquired at three imaging centres using identical MRI scanners (3 T Siemens Skyra, software VD13) and the standard Siemens 32-channel receive head coil. The scanning protocol consisted of structural T1-weighted MRI (T1), resting-state functional MRI (rsfMRI), task fMRI (tfMRI), T2-weighted fluid-attenuated inversion recovery (FLAIR) imaging, diffusion MRI (dMRI) and susceptibility-weighted MRI (swMRI). These different modalities provide information on GM structure (T1), functional connectivity (rsfMRI), brain activation in response to a specific task (tfMRI), volumes of white matter hyperintensities (FLAIR), WM structure/ connectivity (dMRI) and vascular lesions/ iron content (swMRI). Automated pre-processing pipelines were developed for the UK Biobank imaging data to create image-derived phenotypes (IDPs). For T1-weighted data, the IDPs analysed in this study were: total GM, WM and cerebrospinal fluid (CSF) volumes and GM volumes for cortical regions of interest (ROIs), not including the cerebellum, derived using the FAST algorithm as well as subcortical GM volumes derived using the algorithm FIRST. For FLAIR imaging, total volume of white matter hyperintensities (WMHs) was provided as an IDP. All volumetric IDPs (GM and WMH volumes) were corrected for head size using the volumetric scaling factor provided in the UK Biobank data before running statistical tests. The IDPs used from diffusion MRI were fractional anisotropy (FA), mean diffusivity (MD) and three neurite orientation dispersion and density imaging (NODDI) measures (intra-cellular volume fraction [ICVF], isotropic/ free water volume fraction [ISOVF] and orientation dispersion [OD]) averaged across skeletonised white matter tracts, excluding tracts in the cerebellum. The white matter tracts were defined by Alfaro-Almagro et al. [24] based on 48 standard-space tract masks developed by the group of Susumu Mori at Johns Hopkins University [25, 26]. Note that the two IDPs indicating different parts of the cingulum were renamed in this study to use more “standard” notation: the cingulum cingulate gyrus corresponds to the dorsal cingulum in standard notation and the cingulum hippocampus to the ventral cingulum [27]. For swMRI IDPs that denoted median T2* across subcortical structures were investigated. Functional data were not investigated in this study, only 1 IDP that indicated motion during the resting-state fMRI scan was used as a confounder in later analyses.
Medical history and physical measures
Self-reported medical history was used to define history of neurological or cerebrovascular disease or neurological cancers. Additionally, cardiovascular disease (CVD: angina, myocardial infarction, heart or cardiac problem, peripheral vascular disease, leg claudication/ intermittent claudication, arterial embolism, aortic aneurysm, aortic aneurysm rupture), CVD risk factors (hypertension, high cholesterol or diabetes, no distinction between type 1 and type 2), treated hypertension, hypocholesteraemia, or diabetes as well as maternal and paternal AD/ dementia family history were defined by participant report. Participants were classified as hypertensive if the average of two blood pressure measurements at the imaging visit were >= 140 mmHg for systolic blood pressure and/ or >= 90 mmHg for diastolic blood pressure.
Measurements of standing height and weight at the imaging visit were used to calculate body-mass index (BMI) for participants. If standing height was not measured at the imaging visit, measurements from previous visits were used but if weight was not measured at the imaging visit BMI was not calculated and treated as missing.
Other phenotype data
Townsend deprivation index was used as a measure of socioeconomic status [28]. Education was categorised into: no qualification, O-levels or equivalent, A levels or equivalent and University degree or equivalent (includes vocational and professional qualifications).
Exclusion criteria
Participants were excluded: (i) if they reported medical history of conditions that might lead to structural brain abnormalities or cognitive impairment, i.e. any central or peripheral nervous system or nerve tumour, any chronic neurological illness or nervous system trauma, any cerebrovascular disease or intracranial haemorrhage, any infection of nervous system, cranial nerve palsy, spinal cord disorder, epilepsy, or cerebral palsy, (ii) if their UK Biobank genetic quality control flag indicated unusually high heterozygosity or >5% missing genotype rate, or if information on kinship indicated that participants were related to individuals within the sample (3rd degree or closer), or if participants did not have a Caucasian genetic ethnic background, or if there was a mismatch between self-reported sex and genetic sex, or if they carried APOE genotypes other than ε2/ε2, ε2/ε3, ε3/ε3, ε3/ε4 or ε4/ε4, (iii) if they did not have complete MRI datasets with data from all structural modalities and the rsfMRI scan, were outliers (3 standard deviations (SD) above the mean) on head motion during the rsfMRI acquisition or on the number of outlier slices detected during pre-processing of the dMRI data. For the computation of cut-offs, all available MRI data were used irrespective of scan site.
Statistical analyses
Data were analysed with SAS version 9.4 and figures were prepared using R version 3.6.2 (https://cran.r-project.org/). APOE genotype groups were classified as ε2 carriers (genotypes ε2ε2 and ε2ε3), ε3 homozygotes (ε3ε3), ε4 heterozygotes (ε3ε4) or ε4 homozygotes (ε4ε4).
Baseline characteristics were compared between APOE genotype groups with analysis of variance (ANOVA) for continuous variables (age, Townsend deprivation index, BMI) or Pearson’s χ2 test for categorical variables (sex, education, CVD, hypertension, high cholesterol, diabetes, dementia family history).
To analyse effects of APOE genotype on brain structure, multiple linear regression was run for every IDP of interest to determine whether standardised means differed significantly between APOE genotype groups. The IDP was used as the dependent variable and APOE genotype group and confounders as independent variables. One IDP (volume of WMHs) was log-transformed before statistical analyses because the distribution was positively skewed. Before analyses all IDPs were standardised by dividing by their standard deviation. Results were displayed in ‘Manhattan’ style plots of p values for the heterogeneity of each IDP with APOE genotype categories.
Confounders
Models included age and age2, sex, age*sex, age2*sex, educational attainment and twenty principal components of genetic ancestry provided by UK Biobank. Models included neuroimaging confounders, as described previously [29, 30]: the volumetric scaling factor to correct for head size (only used in analyses of non-volumetric IDPs, volumetric IDPs were corrected for head size before statistical analyses), head motion and head motion2 from the rsfMRI analysis and head position (x, y, z) in the MRI scanner as linear and quadratic terms. Since z position and table position in the MRI scanner are highly anticorrelated (r = -0.91), table position was not used as confounder. Month of scan (calculated from the date of first scan) was also added as a categorical confounder to account for temporal drifts in the data. These confounders roughly correspond to the “simple” set of confounders in [30]. Analyses where data from different scan sites were combined (e.g. the replication dataset) were additionally adjusted for the scanner site and the interaction between the site and each imaging confounder.
Correcting for multiple comparisons
Bonferroni correction was applied to correct for multiple comparisons as follows. The alpha level of 0.05 was divided by the total number of modalities investigated, i.e. 4 (T1, dMRI, swMRI and FLAIR), to derive one alpha level per modality, i.e. 0.0125. Within modality, this alpha level was then divided by the number of brain regions investigated: 113 for T1, 200 for dMRI (40 regions*5 different diffusion measures), 14 for swMRI and 1 for FLAIR. This resulted in the following Bonferroni correction thresholds for the different modalities: p < 1 × 10−4 for T1, p < 6 × 10−5 for dMRI, p < 9 × 10−4 for swMRI and 0.0125 for FLAIR.
Discovery and replication dataset
The data were split based on the MRI scanner used for data acquisition. Cheadle was the discovery dataset (n = 17239) and Newcastle (n = 7465) and Reading (n = 3790) were combined as the replication dataset to determine whether IDPs passing the level of significance in the discovery analysis (‘hits’) could be replicated. The p value threshold for significance at replication per modality was 0.0125 divided by the number of significant hits in that modality in the discovery cohort.
Post-hoc analyses of hits in the discovery cohort
For the replicating hits within each modality likelihood ratio tests were used to assess whether hits in left and right hemisphere IDPs remained statistically significant after adjustment for their average level, and if they did not then the average level was used in further analyses.
Effects (in units of standard deviation of the IDP) of each APOE genotype in comparison to the ε3ε3 genotype were estimated. Analyses were first run separately for the discovery and replication dataset and then data from all scan sites were combined in one analysis, adjusted for site.
Sensitivity analyses were conducted altering the level of adjustment for age and neuroimaging confounders: finer adjustment for age using individual years of age as a single year categorical variable, no adjustment for neuroimaging confounders, rank inverse-normal transformation of all IDPs, age and neuroimaging confounders except for imaging centre. All sensitivity analyses were adjusted for twenty principal components of genetic ancestry.
Subgroup analyses
Subgroup analyses were conducted in a combined analysis of all datasets for hits that achieved replication. Differences in the strength of associations by sex and age, separately, were investigated in APOE ε3ε4 and ε4ε4 carriers compared with the APOE ε3ε3 genotype group. To determine more finely at what age APOE genotype differences start to become apparent a further analysis divided participants into five age groups (<55, 55-59, 60-64, 65-69, ≥70 years) and the strength of associations were compared between all APOE genotype groups in each of these age bins. Adjusted rate of cross-sectional change with age at imaging was calculated for all APOE genotype groups from linear regression of IDPs on age at imaging, principal components of genetic ancestry and the other imaging confounders.
Results
After data cleaning steps and applying exclusion criteria, these analyses include 28,494 participants (Supplementary Figure 1).
Participant characteristics at the imaging visit
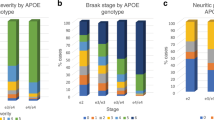
With absence of an APOE ε2 allele or a greater number of ε4 alleles, people had a greater prevalence of hypercholesterolemia and family history of AD (Table 1). APOE ε4 carriers were a median 1 year younger and a had a lower BMI compared with other genotypes. Other characteristics were similar by genotype.
Discovery analyses
In the discovery cohort, WM integrity of four tracts showed statistically significant differences between APOE genotype groups: dorsal cingulum, ventral cingulum, posterior thalamic radiation, and sagittal stratum (Fig. 1a). 3D-images of those brain structures can be found on https://identifiers.org/neurovault.collection:9357.

Measures shown are: a white matter, b grey matter, c swMRI and d volume of white matter hyperintensities. For IDPs that have left and right components, the x positions of left and right components are indicated with red and blue tick marks respectively. L and R is used to distinguish left from right. For grey matter structure, the markers have been ordered by brain region: whole brain, frontal lobe, temporal lobe parietal, occipital, and subcortical. An upwards pointing triangle indicates that the IDP is higher in participants with the APOE ε4ε4 genotype compared with the ε3ε3 genotype, a downwards pointing triangle indicates it is lower.
The WM integrity measures that showed genotype differences were: MD (left only) for the dorsal cingulum; ICVF, MD (both left and right) and FA (right only) for the ventral cingulum; MD and ISOVF (both left and right) for the posterior thalamic radiation; and MD (left and right) for the sagittal stratum. In each tract, WM integrity was lower (increased MD and ISOVF, decreased FA and ICVF) in APOE ε4ε4 carriers compared with the ε3ε3 genotype. Additionally, total WMH volume differed statistically significantly between APOE genotype groups with higher volumes in carriers of APOE ε4ε4 genotype (Fig. 1d).
In contrast, there were no statistically significant differences in volumes of grey matter structures (Fig. 1b) or median T2* in subcortical structures (Fig. 1c) between APOE genotype groups.
Replication analyses
The significance threshold for the replication analysis with data from the other two imaging centres was 0.0125 / 12 hits = 1.0 × 10−3 for the analysis of white matter IDPs and 0.0125 for the volume of white matter hyperintensities.
The following WM integrity IDPs differed significantly by genotype (in the same direction) in both the discovery and replication cohort: MD in the left dorsal cingulum; ICVF and MD in the left and right ventral cingulum; MD and ISOVF in the left and right posterior thalamic radiation; and MD in the left and right sagittal stratum (Fig. 2a). The association of APOE genotype with WMH volume was also replicated (Fig. 2b). An analysis of all IDPs in the replication cohort provided visual confirmation that patterns in the Manhattan plots for the discovery cohort were replicated (Supplementary Figure 2).

The measures shown are: a white matter IDPs and b volume of white matter hyperintensities. L and R is used to distinguish left from right. An upwards pointing triangle indicates that the IDP is higher in participants with the APOE ε4ε4 genotype compared with the ε3ε3 genotype, a downwards pointing triangle indicates it is lower.
Independence of left and right WM hits
In the discovery data, there was no evidence that APOE genotype associations with WM integrity differed by side of tract (left or right) (Supplementary Table 1), so an average of both tracts was used in subsequent analyses.
Sensitivity analyses
Sensitivity analyses were conducted for one white matter IDP (MD in the posterior thalamic radiation). They showed very similar results for all analyses irrespective of the types of adjustments (Supplementary Figure 3).
Comparison of WM integrity and WMH volumes between APOE genotype groups
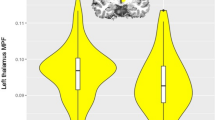
For the IDPs that achieved replication for statistically significant effects of APOE genotype, effects were investigated further to determine, which APOE genotype groups differed significantly from APOE ε3ε3 carriers. APOE ε4ε4 carriers showed the largest differences of 0.14–0.31 standard deviations (SDs) compared with ε3ε3 carriers, ε3ε4 carriers showed very small but statistically significant differences of around 0.05 SDs and ε2 carriers did not differ significantly from ε3ε3 carriers. Thus, the effect size for APOE ε4 homozygotes was much stronger than twice the effect for APOE ε3ε4 carriers (Fig. 3).

The APOE ε3ε3 genotype is the reference group. On the left, there are results for separate analyses for the discovery (red) and replication (blue) dataset. On the right there are results for the combined analysis of all data.
Subgroup analyses by sex and age
For the IDPs that achieved replication for heterogeneity across APOE genotype, there was no strong evidence for effect modification by sex given the number of comparisons when comparing APOE ε3ε4 or ε4ε4 carriers with the reference genotype APOE ε3ε3 (Fig. 4). The comparison of results of two age groups (< 65 years) and (≥ 65 years) indicated that effects differed markedly in APOE ε4ε4 carriers where the older age group showed double or more the effect sizes of the younger group, in particular for WM integrity in the posterior thalamic radiation and sagittal stratum; effects of the APOE ε3ε4 genotype were similar for both age groups (Fig. 4).

Comparison of APOE ε3ε4 (left) and APOE ε4ε4 carriers (right) with the reference group APOE ε3ε3 by sex (male vs female) and by age group (<65 vs ≥65 years) for the IDPs that achieved replication for heterogeneity by APOE genotype.
A more detailed analysis of 5-year age groups showed worsening WM integrity (increase in MD and decrease in ICVF) and an increase in WMH volume with age for all APOE genotype groups in this cross-sectional analysis. For APOE ε2 carriers, ε3ε3 and ε3ε4 genotypes the WM integrity worsened at a similar rate with age, whereas for the APOE ε4ε4 genotype there was a higher rate of change per year from the age group 55–59 years. The mean difference in WM integrity between APOE ε4ε4 carriers and all other genotype groups from age group 65-69 years onwards corresponded to the mean IDP difference seen with around 5 years greater age cross-sectionally over the whole population (Fig. 5).

IDPs are standardised to a mean of zero and a standard deviation of one. APOE ε2 carriers are shown in yellow, ε3 homozygotes in green, ε4 heterozygotes in blue and ε4 homozygotes in red.
Discussion
In this analysis of neuroimaging data from 28,494 UK Biobank participants we found statistically significant effects of APOE genotype on WM integrity and WMH volume but did not observe statistically significant effects on GM volumes or subcortical swMRI measures.
White matter structure
Effects of APOE genotype on several measures of WM integrity were observed: MD in the dorsal cingulum; ICVF and MD in the ventral cingulum; MD and ISOVF in the posterior thalamic radiation and MD in the sagittal stratum. WM integrity was lower (lower ICVF, higher MD) in those with highest AD risk. However, differences were greatest between APOE ε4 homozygote and ε3ε3 carriers, small but consistent between ε4 heterozygotes and ε3ε3 carriers but not statistically significant between ε2 carriers and ε3ε3 carriers. Therefore, APOE genotype differences in WM integrity did not clearly map to AD risk, which is lowest in ε2 carriers [2], but were based on negative effects of the APOE ε4 allele only.
There have been conflicting findings in the literature of possible APOE genotype effects on white matter structure in smaller studies, e.g. positive in [31] or no associations in [9, 32]. In their analysis of a smaller UK Biobank sample Lyall et al. [33] did not find significant effects of APOE genotype on a general factor of FA (gFA), which is a single factor capturing common variance across all white matter tracts. We show here that the differences between genotypes are very localised and mainly driven by the APOE ε4ε4 genotype, which is why, in combination with the smaller study size, they might not have been picked up by Lyall et al. (2020).
The analyses of NODDI measures provide insight into the microstructural properties and biological mechanisms underlying the observed differences. ICVF is a measure of neurite density that is also related to myelination and ISOVF is thought to reflect CSF contamination [34]. Therefore, APOE genotype effects on WM integrity in the ventral cingulum could be driven by neuronal mechanisms and in particular reduced myelination, a process that might play a role in early AD development [35, 36]. The ventral cingulum connects the hippocampus, parahippocampal areas and entorhinal cortex with the posterior cingulate cortex and retrosplenial cortex [27], i.e. areas that show neuronal and synapse loss early in AD [37]. Reduced white matter integrity of this tract has been shown in patients with mild cognitive impairment and AD [27]. A study combining dMRI and histopathology showed that reduced FA and increased MD of the ventral cingulum were associated with higher Braak stages of neurofibrillary tangle pathology in AD patients [38]. Therefore, the findings of reduced integrity of the ventral cingulum here might be indicative of preclinical AD pathology in those at higher genetic AD risk.
In contrast, APOE genotype effects on MD and ISOVF of the posterior thalamic radiation could reflect localised expansion of ventricles, a well-known feature of AD pathology that correlates with cognitive decline [39]. APOE genotype differences in MD in the dorsal cingulum and sagittal stratum were not accompanied by differences in NODDI measures, so the biological mechanisms underlying differences in those tracts are unclear. However, there are previous reports that have shown reduced WM integrity of these tracts in cognitively impaired patients [40, 41].
Effects of age and sex on WM integrity
We conducted an exploratory analysis of WM integrity across the age range in this sample, which indicated that APOE ε4ε4 carriers seem to deviate from the other APOE genotype groups particularly from the age group of 55-59 years. The differences in WM integrity measures in APOE ε4ε4 carriers compared with all other genotype groups correspond to WM integrity measure changes over 5 years in this cross-sectional study. Therefore, they might indicate faster ageing processes in older APOE ε4ε4 carriers. If confirmed in longitudinal studies, this would point to a role of APOE genotype on changes associated with preclinical AD processes rather than effects that exist across the lifespan. This would fit with some larger studies in children and adolescents that have reported no significant effects of APOE genotype on brain structure at younger ages [16, 17].
We did not find any evidence of differences between men and women in APOE genotype effects on brain structure. This would support a recent meta-analysis that reported no sex differences in APOE genotype effects on AD risk [3].
White matter hyperintensities
There have been conflicting reports in the literature investigating possible APOE genotype effects on WMH volume, e.g. positive association in [42], no association in [43]. Significant effects of APOE genotype on WMH volumes have been reported previously in a smaller sample of UK Biobank data [33] and our results are consistent with that report. WMHs are one marker of cerebral small vessel disease [44]. Therefore, APOE genotype might affect AD risk via effects on the vasculature in the brain.
Effect sizes
While we reliably observed effects of APOE genotype on WM structure and WMH volumes, the effect sizes for differences between groups were generally modest with 0.3 SDs or less. On the one hand, this has implications for follow-up MRI studies of APOE genotype effects on brain structure, which need to have large enough sample sizes to be able to detect small effects. On the other hand, it is unclear whether these modest changes can be translated into MRI biomarkers that would be sensitive enough to detect preclinical changes associated with AD development on an individual basis.
Grey matter structure
In this study, we did not observe any significant effects of APOE genotype on volumes of GM structures. This is not necessarily surprising since most studies with larger sample sizes do not report effects on GM structure in cognitively healthy participants, with many focusing specifically on the hippocampus [9, 12,13,14, 45]. This is the largest and most homogenous study that investigated effects on GM structure and did not find any effects. However, it is clear from histopathological studies that GM structures, particularly in the medial temporal lobe, are affected early by neuronal loss in AD development [37]. These changes might be too localised to translate into volumetric differences that can be detected with the IDP MRI measures used in this study. Additionally, histopathological studies have shown that synaptic loss can exceed and predate neuronal loss [37]. It is possible that WM integrity MRI measures investigated here are sensitive enough so that these preclinical changes in neuronal connectivity can be detected here.
Susceptibility-weighted imaging
Similarly, we did not find any significant effects on median T2* in subcortical structures. Increased iron levels that affect median T2* [46], particularly in subcortical structures, have been reported in AD patients [47]. However, there is no study to date that investigated APOE genotype effects on median T2* levels. SWI is sensitive to iron accumulation and therefore bleeding events. A number of meta-analyses reported significant APOE genotype effects on volumes of cerebral microbleeds [42, 48]. Therefore, it might be more appropriate to use the T2* signal to identify localised microbleeds and investigate the volumes of these bleeds, similar to the analysis of WMHs in this paper, rather than averaging the signal across structures.
Limitations
We only included UK Biobank participants with Caucasian genetic ethnic background in this study, i.e. of white British ancestry, because APOE genotype effects on AD risk differ by ethnicity [49] and in turn effects on brain structure might differ as well, and the numbers of participants from other ancestries were too small for separate analysis. Therefore, the results might not be generalisable to other genetic and ethnic backgrounds.
In this large-scale investigation of UK Biobank data we decided to focus on IDPs and did not analyse the native imaging data directly. It is currently unclear whether the use of IDPs, which are obtained by averaging measures such as T2* or FA/MD across structures or tracts, is the best way to identify changes that might happen on a smaller scale and only affect certain parts of a structure. This would become visible in analyses conducted on a voxel-by-voxel basis but not necessarily in the analysis of IDPs averaged across the whole structure.
Additionally, it is important to note that even where we did find significant differences, the effect sizes were modest. This is a cross-sectional study and we do not yet know which participants will go on to develop AD in the coming decades. Therefore, we can only speculate whether the differences between APOE genotypes in white matter integrity might be caused by preclinical AD processes. Participants in the UK Biobank have also been shown to be healthier than the general population [50] and we only included cognitively healthy participants in this study. Therefore, one possible reason why we mostly report null effects could be that a large number of participants will either not develop AD or develop AD relatively late in their life. This would affect our ability to capture the effects of preclinical AD using APOE genotype as a substitute measure for AD risk.
However, evidence from cross-sectional histopathological and PET studies suggests that APOE genotype does affect processes that are relevant at preclinical AD, e.g. the accumulation of amyloid plaques [14, 51]. Our results suggest that these changes might only translate into modest structural changes visible using MRI modalities.
Conclusion
In this comprehensive analysis of APOE genotype effects on brain structure in 28,494 white British UK Biobank participants we showed consistent significant effects on WMH volume and WM integrity of the dorsal and ventral cingulum, posterior thalamic radiation and sagittal stratum in men and women. We did not observe significant differences between APOE genotype groups in volumes of GM structures or median T2* in subcortical structures. APOE genotype effects on WM integrity in the ventral cingulum may be driven by neuronal mechanisms and reduced myelination. We saw that APOE ε4 homozygotes appear to have lower WM integrity at older ages with a potentially steeper decline of WM integrity from the age of 60 that corresponds to around 5 years greater “brain age”. Therefore, APOE genotype effects might be associated with preclinical AD. Whether this is the case may become clear in future, when these participants have been followed up for clinical outcomes and AD detected.
Pre-registration
The pre-registered study protocol is available on doi: https://doi.org/10.17605/OSF.IO/BRN3H. Changes from the pre-registered protocol are described in the supplementary methods.
Open data
UK Biobank is an open access resource and researchers can apply to use the data following procedures outlined on their website: https://www.ukbiobank.ac.uk/enable-your-research.
Code availability
Computer code used to generate the results and figures is available from the corresponding author upon reasonable request.
Change history
28 March 2024
Pre-registration
The pre-registered study protocol is available on doi: 10.17605/OSF.IO/BRN3H. Changes from the pre-registered protocol are described in the supplementary methods.
Open data
UK Biobank is an open access resource and researchers can apply to use the data following procedures outlined on their website: https://www.ukbiobank.ac.uk/enable-your-research. were removed from Acknowledgements to a separate entry.
References
Corder EH, Saunders AM, Strittmatter WJ, Schmechel DE, Gaskell PC, Small GW, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science. 1993;261:921–3.
Farrer LA, Cupples LA, Haines JL. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease: a meta-analysis. JAMA. 1997;278:1349–56.
Neu SC, Pa J, Kukull W, Beekly D, Kuzma A, Gangadharan P, et al. Apolipoprotein E genotype and sex risk factors for Alzheimer disease: a meta-analysis. JAMA Neurol. 2017;74:1178–89.
Frisoni GB, Fox NC, Jack CR, Scheltens P, Thompson PM. The clinical use of structural MRI in Alzheimer disease. Nat Rev Neurol. 2010;6:67–77.
Gordon BA, Blazey TM, Su Y, Hari-Raj A, Dincer A, Flores S, et al. Spatial patterns of neuroimaging biomarker change in individuals from families with autosomal dominant Alzheimer’s disease: a longitudinal study. Lancet Neurol. 2018;17:241–50.
Elmaleh DR, Farlow MR, Conti PS, Tompkins RG, Kundakovic L, Tanzi RE. Developing effective Alzheimer’s disease therapies: clinical experience and future directions. J Alzheimers Dis. 2019;71:715–32.
Haller S, Montandon M-L, Rodriguez C, Ackermann M, Herrmann FR, Giannakopoulos P. APOE * E4 is associated with gray matter loss in the posterior cingulate cortex in healthy elderly controls subsequently developing subtle cognitive decline. Am J Neuroradiol. 2017;38:1335–42.
Operto G, Cacciaglia R, Grau-Rivera O, Falcon C, Brugulat-Serrat A, Ródenas P, et al. White matter microstructure is altered in cognitively normal middle-aged APOE-ε4 homozygotes. Alzheimers Res Ther. 2018;10:48.
Henson RN, Suri S, Knights E, Rowe JB, Kievit RA, Lyall DM, et al. Effect of apolipoprotein E polymorphism on cognition and brain in the Cambridge Centre for Ageing and Neuroscience cohort. Brain Neurosci Adv. 2020;4:239821282096170.
Lim YY, Williamson R, Laws SM, Villemagne VL, Bourgeat P, Fowler C, et al. Effect of APOE genotype on amyloid deposition, brain volume, and memory in cognitively normal older individuals. J Alzheimers Dis. 2017;58:1293–302.
Luo X, Jiaerken Y, Yu X, Huang P, Qiu T, Jia Y, et al. Affect of APOE on information processing speed in non-demented elderly population: a preliminary structural MRI study. Brain Imaging Behav. 2017;11:977–85.
Khan W, Giampietro V, Banaschewski T, Barker GJ, Bokde ALW, Büchel C, et al. A multi-cohort study of ApoE ɛ4 and amyloid-β effects on the hippocampus in Alzheimer’s disease. J Alzheimers Dis. 2017;56:1159–74.
Habes M, Toledo JB, Resnick SM, Doshi J, Van der Auwera S, Erus G, et al. Relationship between APOE genotype and structural MRI measures throughout adulthood in the study of health in pomerania population-based cohort. Am J Neuroradiol. 2016;37:1636–42.
Jack CR, Wiste HJ, Weigand SD, Knopman DS, Vemuri P, Mielke MM, et al. Age, sex, and APOE ε4 effects on memory, brain structure, and β-amyloid across the adult life span. JAMA Neurol. 2015;72:511–9.
Lissaman R, Lancaster TM, Parker GD, Graham KS, Lawrence AD, Hodgetts CJ. Tract-specific differences in white matter microstructure between young adult APOE ε4 carriers and non-carriers: a replication and extension study. Neuroimage Rep. 2022;2:100126.
Dell’Acqua F, Khan W, Gottlieb N, Giampietro V, Ginestet C, Bouls D, et al. Tract based spatial statistic reveals no differences in white matter microstructural organization between carriers and non-carriers of the APOE ɛ4 and ɛ2 alleles in young healthy adolescents. J Alzheimers Dis. 2015;47:977–84.
Khan W, Giampietro V, Ginestet C, Dell’Acqua F, Bouls D, Newhouse S, et al. No differences in hippocampal volume between carriers and non-carriers of the ApoE ε4 and ε2 alleles in young healthy adolescents. J Alzheimers Dis. 2014;40:37–43.
Chang L, Douet V, Bloss C, Lee K, Pritchett A, Jernigan TL, et al. Gray matter maturation and cognition in children with different APOE ε genotypes. Neurology. 2016;87:585–94.
Dean DC, Jerskey BA, Chen K, Protas H, Thiyyagura P, Roontiva A, et al. Brain differences in infants at differential genetic risk for late-onset Alzheimer disease: a cross-sectional imaging study. JAMA Neurol. 2014;71:11–22.
Allen N, Sudlow C, Downey P, Peakman T, Danesh J, Elliott P, et al. UK Biobank: current status and what it means for epidemiology. Health Policy Technol. 2012;1:123–6.
Sudlow C, Gallacher J, Allen N, Beral V, Burton P, Danesh J, et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12:e1001779.
Bycroft C, Freeman C, Petkova D, Band G, Elliott LT, Sharp K, et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562:203–9.
Miller KL, Alfaro-Almagro F, Bangerter NK, Thomas DL, Yacoub E, Xu J, et al. Multimodal population brain imaging in the UK Biobank prospective epidemiological study. Nat Neurosci. 2016;19:1523–36.
Alfaro-Almagro F, Jenkinson M, Bangerter NK, Andersson JLR, Griffanti L, Douaud G, et al. Image processing and Quality Control for the first 10,000 brain imaging datasets from UK Biobank. NeuroImage. 2018;166:400–24.
Mori S, Crain BJ. MRI Atlas Of Human White Matter (Elsevier, 2006).
Wakana S, Caprihan A, Panzenboeck MM, Fallon JH, Perry M, Gollub RL, et al. Reproducibility of quantitative tractography methods applied to cerebral white matter. NeuroImage. 2007;36:630–44.
Bubb EJ, Metzler-Baddeley C, Aggleton JP. The cingulum bundle: anatomy, function, and dysfunction. Neurosci Biobehav Rev. 2018;92:104–27.
Phillimore P, Beattie A, Townsend P. Widening inequality of health in northern England, 1981-91. BMJ. 1994;308:1125–8.
Elliott LT, Sharp K, Alfaro-Almagro F, Shi S, Miller KL, Douaud G, et al. Genome-wide association studies of brain imaging phenotypes in UK Biobank. Nature. 2018;562:210–6.
Alfaro-Almagro F, McCarthy P, Afyouni S, Andersson JLR, Bastiani M, Miller KL, et al. Confound modelling in UK Biobank brain imaging. NeuroImage. 2021;224:117002.
Operto G, Molinuevo JL, Cacciaglia R, Falcon C, Brugulat-Serrat A, Suárez-Calvet M, et al. Interactive effect of age and APOE-ε4 allele load on white matter myelin content in cognitively normal middle-aged subjects. NeuroImage Clin. 2019;24:101983.
Nyberg L, Salami A, The APOE. ε 4 allele in relation to brain white-matter microstructure in adulthood and aging. Scand J Psychol. 2014;55:263–7.
Lyall DM, Cox SR, Lyall LM, Celis-Morales C, Cullen B, Mackay DF, et al. Association between APOE e4 and white matter hyperintensity volume, but not total brain volume or white matter integrity. Brain Imaging Behav. 2020;14:1468–76.
Zhang H, Schneider T, Wheeler-Kingshott CA, Alexander DC. NODDI: practical in vivo neurite orientation dispersion and density imaging of the human brain. NeuroImage. 2012;61:1000–16.
Nasrabady SE, Rizvi B, Goldman JE, Brickman AM. White matter changes in Alzheimer’s disease: a focus on myelin and oligodendrocytes. Acta Neuropathol Commun. 2018;6:22.
De Strooper B, Karran E. The cellular phase of Alzheimer’s disease. Cell. 2016;164:603–15.
Serrano-Pozo A, Frosch MP, Masliah E, Hyman BT. Neuropathological alterations in Alzheimer disease. Cold Spring Harb Perspect Med. 2011;1:a006189.
Kantarci K, Murray ME, Schwarz CG, Reid RI, Przybelski SA, Lesnick T, et al. White-matter integrity on DTI and the pathologic staging of Alzheimer’s disease. Neurobiol Aging. 2017;56:172–9.
Chou Y-Y, Leporé N, Saharan P, Madsen SK, Hua X, Jack CR, et al. Ventricular maps in 804 ADNI subjects: correlations with CSF biomarkers and clinical decline. Neurobiol Aging. 2010;31:1386–1400.
Sepehrband F, Cabeen RP, Barisano G, Sheikh‐Bahaei N, Choupan J, Law M, et al. Nonparenchymal fluid is the source of increased mean diffusivity in preclinical Alzheimer’s disease. Alzheimers Dement. 2019;11:348–54.
Nir TM, Jahanshad N, Villalon-Reina JE, Toga AW, Jack CR, Weiner MW, et al. Effectiveness of regional DTI measures in distinguishing Alzheimer’s disease, MCI, and normal aging. NeuroImage Clin. 2013;3:180–95.
Schilling S, DeStefano AL, Sachdev PS, Choi SH, Mather KA, DeCarli CD, et al. APOE genotype and MRI markers of cerebrovascular disease: Systematic review and meta-analysis. Neurology. 2013;81:292–300.
Paternoster L, Chen W, Sudlow CLM. Genetic determinants of white matter hyperintensities on brain scans: a systematic assessment of 19 candidate gene polymorphisms in 46 studies in 19,000 subjects. Stroke. 2009;40:2020–6.
ter Telgte A, van Leijsen EMC, Wiegertjes K, Klijn CJM, Tuladhar AM, de Leeuw F-E. Cerebral small vessel disease: from a focal to a global perspective. Nat Rev Neurol. 2018;14:387–98.
Roshchupkin GV, Adams HH, van der Lee SJ, Vernooij MW, van Duijn CM, Uitterlinden AG, et al. Fine-mapping the effects of Alzheimer’s disease risk loci on brain morphology. Neurobiol Aging. 2016;48:204–11.
Yao B, Li T, Gelderen P, Shmueli K, Dezwart J, Duyn J. Susceptibility contrast in high field MRI of human brain as a function of tissue iron content. NeuroImage. 2009;44:1259–66.
Langkammer C, Ropele S, Pirpamer L, Fazekas F, Schmidt R. MRI for iron mapping in Alzheimer’s disease. Neurodegener Dis. 2014;13:189–91.
Maxwell SS, Jackson CA, Paternoster L, Cordonnier C, Thijs V, Salman RA-S, et al. Genetic associations with brain microbleeds: systematic review and meta-analyses. Neurology. 2011;77:158–67.
Belloy ME, Andrews SJ, Le Guen Y, Cuccaro M, Farrer LA, Napolioni V, et al. APOE genotype and Alzheimer disease risk across age, sex, and population ancestry. JAMA Neurol. 2023;80:1284.
Fry A, Littlejohns TJ, Sudlow C, Doherty N, Adamska L, Sprosen T, et al. Comparison of sociodemographic and health-related characteristics of UK biobank participants with those of the general population. Am J Epidemiol. 2017;186:1026–34.
Abner EL, Neltner JH, Jicha GA, Patel E, Anderson SL, Wilcock DM, et al. Diffuse amyloid-β plaques, neurofibrillary tangles, and the impact of APOE in elderly persons’ brains lacking neuritic amyloid plaques. J Alzheimers Dis. 2018;64:1307–24.
Acknowledgements
This research has been conducted using the UK Biobank resource under application number 8835 (PI: Sarah Parish). We would like to thank UK Biobank participants and research team members who collected the data and administered the data release. We are especially grateful to the UK Biobank brain MRI team, in particular Prof Stephen Smith and Dr Fidel Alfaro-Almagro, who delivered pre-processed MRI data to UK Biobank. This work was supported by grants to the University of Oxford from the UK Medical Research Council through its funding of the MRC Population Health Research Unit (MC_ UU_00017/5); and the British Heart Foundation. VH was supported through a Nuffield Department of Population Health Intermediate Fellowship. CEM was supported by the NIHR Oxford Health Biomedical Research Centre. For the purpose of open access, the authors have applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising.
Author information
Authors and Affiliations
Contributions
Verena Heise: conceptualisation, data curation, formal analysis, methodology, project administration, software, validation, visualisation, and writing – original draft preparation; Alison Offer: data curation, formal analysis, software, validation, visualisation, and writing – review and editing; William Whiteley: conceptualisation and writing – review and editing; Clare Mackay: conceptualisation, supervision, and writing – review and editing; Jane Armitage: conceptualisation, supervision, and writing – review and editing; Sarah Parish: conceptualisation, funding acquisition, methodology, resources, supervision, and writing – review and editing
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heise, V., Offer, A., Whiteley, W. et al. A comprehensive analysis of APOE genotype effects on human brain structure in the UK Biobank. Transl Psychiatry 14, 143 (2024). https://doi.org/10.1038/s41398-024-02848-5
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-024-02848-5
