
Abstract
In recent years, machine learning (ML) has been a promising approach in the research of treatment outcome prediction in psychosis. In this study, we reviewed ML studies using different neuroimaging, neurophysiological, genetic, and clinical features to predict antipsychotic treatment outcomes in patients at different stages of schizophrenia. Literature available on PubMed until March 2022 was reviewed. Overall, 28 studies were included, among them 23 using a single-modality approach and 5 combining data from multiple modalities. The majority of included studies considered structural and functional neuroimaging biomarkers as predictive features used in ML models. Specifically, functional magnetic resonance imaging (fMRI) features contributed to antipsychotic treatment response prediction of psychosis with good accuracies. Additionally, several studies found that ML models based on clinical features might present adequate predictive ability. Importantly, by examining the additive effects of combining features, the predictive value might be improved by applying multimodal ML approaches. However, most of the included studies presented several limitations, such as small sample sizes and a lack of replication tests. Moreover, considerable clinical and analytical heterogeneity among included studies posed a challenge in synthesizing findings and generating robust overall conclusions. Despite the complexity and heterogeneity of methodology, prognostic features, clinical presentation, and treatment approaches, studies included in this review suggest that ML tools may have the potential to predict treatment outcomes of psychosis accurately. Future studies need to focus on refining feature characterization, validating prediction models, and evaluate their translation in real-world clinical practice.
Similar content being viewed by others


Introduction
Schizophrenia (SCZ) is a major chronic psychiatric disorder that represents one of the top eight causes of disability worldwide [1], leading to demanding social, professional, and economic consequences [2, 3]. SCZ typically develops during early adulthood. It is characterized by positive, negative, and cognitive symptoms. While positive symptoms are characterized by hallucinations, delusions, and formal thought disorder, negative symptoms consist of a lack of volition and emotiveness with reduced speech output. Cognitive symptoms are characterized by cognitive deterioration in all domains of neuropsychological function [3].
Although the pathogenesis of SCZ is still unknown, multiple strands of evidence indicate that it is a progressive neurodevelopmental disorder [4]. Recent advances in research have suggested that SCZ is a multifactorial disorder with a combination of genetic and environmental risk factors involved in its pathogenesis. In recent years, genome-wide association studies have identified hundreds of genetic loci that were associated with SCZ proving its polygenic disorder nature [5]. Moreover, neuroimaging studies have played a central role in providing abundant evidence of structural and functional brain abnormalities in patients with SCZ at different phases of the disorder [6,7,8,9].
SCZ requires long-term treatment that is commonly based on antipsychotic medications, which are primarily indicated for the treatment of SCZ and psychotic disorders [10]. First-generation antipsychotics (FGAs), also known as typical antipsychotics, were developed in the 1950s [11]. The efficacy of this pharmacological class depends on its ability to reduce dopamine function by blocking the dopamine D2 family of postsynaptic receptors [3]. However, the occurrence of adverse effects associated with FGAs, in particular debilitating extrapyramidal side effects, led to the introduction of second-generation antipsychotics (SGAs), also known as atypical antipsychotics. The SGAs are potent 5-HT2a receptor antagonists and relatively weaker dopamine D2 antagonists and are associated with a substantially lower risk of neurologic adverse effects [12].
Treatment choices for patients with SCZ and psychotic disorders are currently based on treatment guidelines broadly depending on clinical conditions and symptom classification without reference to the patients’ biological background [13]. In this context, the identification of predictors of treatment response in patients with SCZ is a task of substantial importance to help clinicians make informed treatment initiation and personalize treatment decisions [14]. Specifically, over the last decades researchers have tried to identify specific factors involved in treatment response, leading to studies focusing on multiple variables, such as clinical, neuroimaging, and genetic characteristics, to create prognostic prediction models [15].
In recent years, machine learning (ML) approaches have been suggested to be a promising innovative tool with the potential to develop accurate and generalizable treatment response predictions about individuals with psychiatric disorders [15, 16]. ML is a subfield of artificial intelligence broadly defined as a computational strategy which employs algorithms that automatically determine methods and parameters learning from complex data to reach an optimal prediction [16,17,18]. Before ML analysis, a rigorous collection of relevant data and pre-processing steps are performed, then prediction models are trained and tested during the learning process [18]. Recently, ML research has used the power of large-scale, multidimensional databases and advanced biological data sources to develop prediction models for diagnostic, prognostic, and treatment selection procedures [15, 16]. Interestingly, ML techniques have been also used to predict treatment outcomes in patients with psychiatric disorders such as depression, showing good accuracies [19,20,21].
For SCZ, important advances have been made toward the identification of clinical and biological predictors of treatment response, especially in studies using large multisite treatment databases containing prospective data of individuals with an early course of psychosis [22, 23]. Indeed, ML techniques could help direct the early implementation of targeted interventions that have been shown to result in better clinical and functional outcomes for more vulnerable individuals [24]. Thus, mainly clinical [23] and neuroimaging data [25, 26] have been used as potential predictors of treatment outcomes in SCZ.
Given that SCZ is associated with magnetic resonance imaging (MRI) signal abnormalities, and that these have been associated with symptom profiles as well as outcome, neuroimaging measures have been considered promising biological markers for treatment outcome [26]. Especially in MRI studies, important findings have been discovered. Indeed, findings from structural MRI (sMRI) studies indicate that response to antipsychotics is associated with altered brain volumes in specific brain regions, while functional MRI (fMRI) studies observed increased baseline brain activity and connectivity in treatment responders [25].
Despite the increasing number of studies published in this area over recent years, the impact of ML on treatment response prediction in patients with psychosis is still unclear. No study to our knowledge has comprehensively reviewed the advancements and challenges of ML approaches in the development of therapeutical predictors in SCZ to date. In this context, this study aims to provide a comprehensive literature review of current knowledge about ML methodologies applied for the prediction of antipsychotic treatment response in individuals with early and chronic course of SCZ.
Methods
For the purpose of this review, a literature search was performed on the Pubmed database following the PRISMA guideline recommendations [27]. The following search words were used: “schizophrenia” OR “psychosis”, “treatment” OR “antipsychotics”, “machine learning” OR “prediction”. The electronic search was completed on all available years until March 15, 2022. Records were screened after the removal of duplicates based on the title, abstract, and full text. The selection process was conducted by two independent researchers. Disagreements were resolved by a third independent investigator.
The inclusion criteria for the studies were the following: (1) English language, (2) clinical trials, (3) human studies, (4) inclusion of subjects clinically diagnosed with SCZ or non-affective psychotic disorders, (5) use of treatment with antipsychotics, and (6) use of ML techniques to predict clinical outcome. For each publication, the following variables were extracted: sample characteristics, clinical information, ML analyses performed, performance measures, and main results.
Results
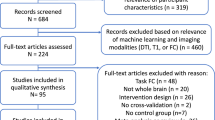
The database literature search resulted in 784 articles, which were screened for eligibility. Among them, 226 studies were duplicates. Then, 507 articles were excluded based on title and abstract review. The full text of the remaining 51 papers was checked for eligibility and 23 of them were excluded. Overall, a total of 28 articles were included in this review (Fig. 1). The main characteristics and findings of the included studies are summarized in Table 1.

Flow chart of study selection.
Clinical characteristics
The sociodemographic and clinical characteristics of participants in included studies are presented in Table 1. Among the 28 included publications, the majority of them considered only subjects with the first episode of psychosis (FEP) [23, 28,29,30,31,32,33,34,35,36,37], while 10 studies considered patients with chronic SCZ [38,39,40,41,42,43,44,45,46,47]. The remaining selected studies included both FEP and SCZ patients [48,49,50,51,52,53,54].
Regarding the pharmacological treatment that was used to explore outcome prediction in patients with psychosis, in the broad majority of included studies patients were treated with SGAs. Only in 2 studies subjects were treated only with FGAs, while in four studies both classes of antipsychotics were considered.
ML approaches
Importantly, the included studies used heterogeneous predictors and different ML approaches to develop models to predict treatment outcomes in individuals with psychotic disorders. Indeed, several sociodemographic, clinical, and neuroimaging measures have been used as variables, or features, for the ML analyses performed in the included studies.
Specifically, 23 studies used only one modality as input to the ML algorithms, for example only MRI or electroencephalography (EEG) data, while the other five studies combined or compared different modalities. In order to better analyze and compare different selected articles, in the present review results of single-modality studies and multi-modality studies have been presented separately in the following sections.
Among the single-modality studies, many of them used functional and structural brain features for developing an ML prediction model. Specifically, 6 studies used resting-state fMRI (rs-fMRI) data [29, 30, 33, 34, 52, 53] while 1 study analyzed task-based fMRI images [39]. Moreover, three studies used sMRI measures [31, 49, 50], three studies used EEG data [41, 43, 47], one study considered positron emission tomography (PET) data [54], and one study used proton magnetic resonance spectroscopy (MRS) data [36]. Conversely, eight studies used clinical and sociodemographic data as input features to the ML algorithms [23, 35, 37, 38, 40, 42, 44, 51]. Among the multi-modality studies, different sets of features were used together as input to the ML algorithms. Specifically, Cui et al. [48] used both sMRI and fMRI data, Wang et al. [46] used a combination of sMRI, fMRI, and cognitive data, Ambrosen et al. [28] considered sMRI, EEG, and cognitive data together, while Uematsu & Hisanobu [45] used sMRI and sociodemographic data. Finally, Ebdrup et al. [32] used sMRI, EEG, DTI, and neurocognitive test data separately for ML analyses.
Additionally, included studies differed in clinical outcomes that were used in the ML analyses. The broad majority of them used changes in scores of psychotic symptom severity scales, such as the Positive and Negative Syndrome Scale (PANSS) and the Brief Psychiatric Rating Scale (BPRS), as measures of clinical improvement [28,29,30,31, 33,34,35, 39, 41, 43, 44, 46, 48,49,50, 53, 54]. In many of these studies, ML methods were applied to predict binary outcomes (“response” versus “no response”, or “remission” versus “no remission”) to antipsychotic treatment [28, 29, 32, 35, 39, 41, 43, 44, 46, 48, 49, 51, 54] while several studies used ML techniques for predicting continuous values such as reduction rates of PANSS and BPRS. Additionally, as the definition of treatment outcome is not merely defined by the symptomatic response, but might base on complex clinical and social domains, other measures and scales assessing specific symptoms and functioning criteria were used as labels in many studies [23, 36,37,38, 40, 42, 45, 47, 51, 52]. Therefore, the heterogeneity and complexity of relevant outcome indicators pose a challenge in synthesizing results and generating robust overall conclusions of the relevance of the included studies. Moreover, the use of different outcome measures influenced the type of ML methodology applied to develop accurate and generalizable treatment prediction models.
Indeed, several ML methods have been applied to develop accurate and generalizable treatment prediction models. Different ML approaches used in studies included in this review could be divided into classification algorithms, generally used to categorize the data into different outcome classes, and regression algorithms, performed to predict a continuous outcome value based on the input features. Specifically, classification algorithms were operated by 14 studies [23, 32, 35, 37, 41, 43, 44, 46,47,48,49, 51, 52, 54] while regression algorithms were used by 12 studies [29,30,31, 33, 34, 36, 38, 40, 42, 45, 50, 53]. Additionally, two studies used both classification and regression algorithms to predict symptomatic improvement in patients with psychosis [28, 39].
Finally, a difference between studies regarding methodology was in the use of single or multiple ML approaches. Specifically, 17 studies used only one ML method to identify specific predictors and develop an accurate treatment prediction model [29,30,31, 33,34,35,36,37, 42, 45,46,47,48,49,50, 52, 53], while the remaining studies compared the accuracy of different ML methods [23, 28, 32, 38,39,40,41,42,43,44, 51, 54]. Specifically, several studies found that support vector regressor (SVR) has the highest and most consistent overall accuracy compared to different ML techniques [23, 41, 43, 54], suggesting that SVR can deal with imbalanced datasets more effectively than other ML approaches [23, 41]. Nevertheless, other studies showed that predictions on the same dataset were similar regardless of the different ML methods used [28, 32, 40, 51], while in one study a random forest algorithm performed best relative to other approaches [44]. Finally, one study that compared different ML methods and one deep learning (DL) approach showed that the best overall performances were achieved using DL, suggesting that DL might be a promising approach for treatment predictions in patients with psychosis and supporting the development of DL-based methods in future research [39].
Summary of single-modality studies
As previously reported, the broad majority of included studies used features extracted from a single modality as input to the ML algorithms. Many of them used neuroimaging measures to predict treatment outcomes in patients with psychosis, while others used clinical features.
sMRI features
Only three studies used structural neuroimaging features as input to the ML algorithms. Cui et al. [49] analyzed a cohort of 191 FEP and SCZ subjects, who were classified as responders or non-responders to antipsychotic treatment based on the reduction of PANSS scores. The input to the random forest (RF) classifier were different thalamic morphological features, such as volume and thickness. ML analyses showed that antipsychotic treatment response was predicted with an accuracy of 75%, suggesting that thalamus radiomic features can be promising in the definition of treatment selection.
Another sMRI study analyzed data of 44 FEP individuals treated with olanzapine for 8 weeks [31]. The gray matter volumes (GMV) of subregions of the superior temporal gyrus (STG) were used as input to an SVR, and the reduction rate of PANSS total score was the outcome measure. The SVR results exhibited a significant association between GMV of the STG and symptomatic improvement as effect of antipsychotic treatment.
Finally, Homan et al. [50] conducted an sMRI study on 82 FEP and early-diagnosed SCZ subjects treated with aripiprazole or risperidone for 12 weeks. They performed a partial least squares (PLS) regression using nodal degrees, calculated from brain cortical thickness, as predictors, and the continuous treatment response, based on the BPRS reduction, as output. Results of PLS regressions suggested that nodal degree in orbito- and prefrontal areas significantly contributed to the prediction of treatment response, with additional contributions from superior temporal regions.
In summary, these studies demonstrate structural radiomics approaches to predict the clinical response of antipsychotic treatment in early SCZ with significant accuracies. Specifically, GMV and thickness measures of specific brain regions, such as thalamic, temporal, and frontal areas, may represent important features that could play a role in the development of prognostic tools for individualized early treatment of SCZ [31, 49, 50].
fMRI features
Among the seven included fMRI studies, most of them considered resting-state activity and functional connectivity (FC) measures as predictive features, while only one used task-based functional brain activations as predictors. These studies showed substantial heterogeneity in the brain functional biomarkers that were found as meaningful predictors of antipsychotic treatment outcomes. Specifically, Blessing et al. [29] recruited 29 FEP subjects treated with SGAs for 8 weeks. They explored whether baseline brain functional connectivity (FC) predicted treatment response using the RF algorithm. ML analyses showed that hippocampal FC with insular–opercular cortex, superior frontal gyrus, precentral gyrus, and postcentral gyrus predicted treatment response with an accuracy of 89%.
Li et al. [33] recruited two independent samples of FEP patients treated with olanzapine for 8 weeks: one sample of 32 subjects as a training set and another sample with 44 subjects as a test set. The fractional amplitude of low-frequency fluctuation (fALFF) and SVR analysis were used to predict treatment response, showing a positive relationship between baseline fALFF levels in the left ventromedial putamen and improvement in positive symptoms. Moreover, the same SVR analyses were performed using global-brain FC (GFC), revealing a positive relationship between GFC in the bilateral anterior cingulate cortex and improvement in negative symptoms [34].
Also, Sarpal et al. [52] divided the cohort into a training set of 41 FEP subjects and a test set of 40 patients with chronic SCZ to develop a prognostic index based on rs-fMRI. A Cox regression analysis was performed in subjects classified as responders and non-responders. A striatal connectivity index was built from FC values between the striatum and 91 brain regions. The index significantly predicted the treatment response, and this result was validated in the independent cohort of antipsychotic-treated patients.
Shan et al. [53] explored whether the brain voxel-mirrored homotopic connectivity might predict individual treatment response in 21 patients with SCZ treated with olanzapine. An SVR analysis revealed that FC in the superior/middle prefrontal cortex at baseline could predict the symptomatic improvement of PANSS total, positive, and negative symptom subscale scores after 8 weeks of treatment.
Cao et al. [30] enrolled a small dataset of 43 FEP subjects for 10 weeks of risperidone treatment. By using SVR analysis and the FC of the superior temporal cortex with dorsal-lateral prefrontal, cingulate, temporal, and parietal cortices, this study predicted response to antipsychotic treatment at an individual level with an accuracy of 82.5%.
Finally, Smucny et al. [39] evaluated the ability of different ML and DL algorithms to predict symptomatic improvement in 65 patients with SCZ and 17 patients with bipolar disorder treated with SGAs by using fMRI frontoparietal activations during a continuous performance task as features. Higher overall performances were obtained using DL (accuracy of 70%) compared to ML algorithms, suggesting that DL might be a promising approach to predict treatment outcomes in SCZ.
In summary, despite a wide degree of methodological heterogeneity between the included studies, these findings suggest that fMRI features may contribute to the prediction of clinical outcomes in the early onset of psychosis with high accuracies. Specifically, several FC studies revealed that brain areas implicated in functional networks that play a key role in emotion and cognitive regulation were the most predictive features of treatment outcome and may be targets of antipsychotic treatment [29, 30, 34, 52, 53]. Moreover, it was found that also specific patterns of brain activation in cortical and subcortical brain regions may be useful for predicting treatment outcomes in the recent onset of psychosis [33, 39]. However, it is important to note that included studies presented several limitations, such as small sample sizes [29, 30, 33, 34, 39, 52, 53] and lack of replication samples [29, 30, 34, 39, 53].
Other neuroimaging features
Among studies that used other neuroimaging techniques as features for their ML analysis, Veronese et al. [54] used a PET approach to identify potential brain functional biomarkers of treatment stratification in 26 FEP subjects and 24 non-responsive SCZ patients. Linear and nonlinear ML analyses were performed; higher predictive power of treatment response was shown by linear SVM with an area under the curve (AUC) of 0.89 for striatal biomarkers, a good result that needs to take into consideration the small, but balanced, dataset.
Wood et al. [36] used proton MRS to investigate the predictive value of frontal and temporal spectroscopy measures in a modest dataset of 46 FEP patients treated with SGAs. An omnibus multivariate regressor was used to predict clinical and functional outcomes. It was found that N-acetylaspartate and choline-containing compounds to creatine and phosphocreatine ratio in the prefrontal cortex were significant predictors of antipsychotic treatment response.
EEG features
Interestingly, the three studies that used EEG features aimed to perform ML classification analysis on chronic treatment-resistant SCZ subjects treated with clozapine. Firstly, Khodayari-Rostamabad et al. [47] enrolled 37 subjects to conduct a kernelized PLS regression procedure, showing that a set of pre-treatment discriminative EEG features was able to predict clinical response to clozapine with an accuracy of 85%. The other studies that aimed to develop a prognostic algorithm based on pre-treatment EEG data compared different ML approaches. They found that SVM resulted to be the method with the highest accuracy (95.83% [41] and 89.90% [43] respectively) in discriminating between responders and non-responders to clozapine treatment. Should be noted that all three studies considered a small dataset, which was also unbalanced in one study [41].
Socio-demographical and clinical features
Noteworthy, several studies used different sociodemographic and clinical measures as features for ML analysis. Many of them found that important predictors of antipsychotic treatment outcome were baseline severity of psychotic symptoms [35, 37, 42, 44, 51] and comorbidities [23, 40], suggesting that ML models developed by including routinely available, patient-reportable information might present adequate predictive ability to be applied in clinical settings.
Most of these studies aimed to identify baseline measurable socio-demographical and clinical characteristics to predict treatment outcomes in chronic SCZ. Specifically, Anderson et al. [40] recruited 763 chronic SCZ patients and assessed baseline clinical predictors of treatment response using multivariate Cox and generalized linear regressions. The AUC of an ensemble of different models resulted in 0.75 for clinical remission. The most important predictors of remission were the use of long-acting injectable antipsychotics and the absence of psychiatric comorbidities.
In a study assessing 242 chronic SCZ patients treated with clozapine, the Least Absolute Shrinkage, and Selection Operator (LASSO) regression was used to develop a response prediction model [42]. The predictors of response to clozapine were severity of illness at baseline, female gender, and comorbid mood disorder.
Moreover, Legge et al. [38] recruited 1070 subjects with chronic SCZ or related psychotic disorders to investigate the ability of demographic and clinical premorbid factors to predict resistance to antipsychotic treatment. The authors performed a multivariate logistic regression and a conditional inference forest model, finding that earlier age at the onset of psychosis and poor premorbid functioning might be useful predictors of antipsychotic treatment outcome.
Additionally, many studies have found that measures of psychotic symptom severity at baseline might be considered adequate clinical predictors of antipsychotic treatment outcomes in patients with SCZ. Indeed, PANSS scores at baseline resulted to be the most predictive features in a study that enrolled 639 SCZ [44]. The RF algorithm performed best relative to other ML classifiers (SVM, LR, and Naïve Bayes) in terms of model ability to classify patients’ responses after 6 months of treatment, showing an AUC of 0.7 on the test set.
Moreover, Li et al., [51] compared different ML approaches (logistic regression, stochastic gradient descendent, gradient boosting decision tree, extreme gradient boosting, and RF) to predict social functioning improvement in 550 patients with SCZ treated with SGAs. The best AUC (0.86) was reached with RF, while the most important features were the use of mood stabilizers, social functioning, and PANSS total scores at baseline.
Furthermore, some studies used socio-demographical and clinical features to predict treatment outcome in FEP patients. Specifically, in a multicenter study that recruited two independent samples of 334 FEP patients in the training set and 108 FEP patients in the test set, pre-treatment clinical information, particularly psychosocial, sociodemographic, and psychometric variables were used as features for ML analysis to predict functional outcome after treatment with FGAs or SGAs [23]. Several algorithms, such as linear and nonlinear SVM, decision trees, and univariate and multivariate logistic regression were compared, obtaining the highest balanced accuracy (71.7%) by using nonlinear SVM on the test set. The most valuable predictors identified were largely psychosocial features, rather than symptom data: unemployment, poor education, functional deficits, and unmet psychosocial needs.
Soldatos et al. [35] recruited 270 FEP subjects and used SVM algorithms to classify remission and non-remission in patients treated with SGAs. Using items from validated clinical scales assessing psychotic symptom severity and functioning as features, the ML model significantly predicted early remission after treatment.
Finally, Wu et al. [37] used an ML method to develop antipsychotic treatment recommendations based on socio-demographical and clinical characteristics from 32277 FEP subjects. By using the individualized treatment rule (ITR) developed by applying a minimum loss–based ensemble ML method, the estimated treatment success rate was 51.7%. Results of this study suggested that an ITR developed using demographic and clinical predictors such as age, psychotic symptom severity, and the use of mood stabilizers or benzodiazepines, may be associated with an increase in the treatment success rate among FEP subjects.
Summary of multi-modality studies
In recent years, advances have been made toward combining data from multiple modalities, in order to improve treatment response prediction. In this review, we included five studies applying multimodal approaches to patients with psychosis for treatment response prediction. These studies have utilized features from a variety of modalities, including structural and functional neuroimaging, socio-demographical, and cognitive data.
Specifically, Ambrosen et al. [28] analyzed a cohort of 138 initially drug-naïve FEP patients. They used sMRI, EEG, and cognitive data in two independent ML approaches, one based on a single algorithm and the other incorporating an ensemble of algorithms. For the prediction of short- and long-term antipsychotic treatment response, ML analyses yielded non-significant results. Moreover, in another study assessing treatment response in 46 antipsychotic-naïve FEP patients by using EEG, sMRI, and neurocognitive features, none of the SVM algorithms predicted symptom remission [32].
Cui et al. [48] used sMRI and fMRI features to predict the early response to antipsychotic treatment in 148 SCZ subjects. The SVM method was used to construct the classification model based on LASSO features. The prediction accuracy was 80.38% for the model using fMRI features only, 69.68% for the model using sMRI features, and 85.03% for the model combining both features, highlighting the importance of multimodal neuroimaging approaches in treatment response prediction.
Uematsu & Hisanobu [45] employed multiple regression analysis to predict treatment response based on sMRI and socio-demographical features in 40 SCZ patients. The results of this study demonstrated that the size of the cerebellar vermis and specific clinical features, such as symptom severity rates and duration of hospitalization, were related to antipsychotic treatment response.
Finally, Wang et al. [46] recruited 57 SCZ patients to assess whether neuroimaging and genetic features are predictive of antipsychotic treatment outcomes. The extreme gradient boosting (XGBoost) ML method was employed to combine sMRI, fMRI, and the schizophrenia polygenic risk score (PRS) as predictive features. Considering the small dataset, the combination of MRI measures (especially fALFF, GMV, and surface curvature) and PRS predicted treatment response with an accuracy of 86%, suggesting the importance of neuroimaging and genetic predictors in ML studies.
In conclusion, studies that compared different features found that functional neuroimaging contributed the most to predictions of clinical outcomes of psychosis relative to specific structural neuroimaging [46, 48] and genetic features [46]. Nevertheless, most of the models that combined multiple features showed higher accuracy than single-modality models, suggesting that, due to the complexity and heterogeneity of psychotic disorders, multimodal approaches may be able to predict more accurate outcomes of antipsychotic treatment [46, 48]. However, these findings must be interpreted with caution due to inconclusive results reported in some of the included studies [28, 32].
Discussion
Prediction of treatment outcomes remains a significant challenge for psychiatry in the current era of personalized medicine. The increasing availability of large-scale datasets contributed to the development of sophisticated ML approaches, which have improved the accuracy of prediction over the use of conventional statistical models by capturing complex, nonlinear relationships in the data [55]. In recent years, ML methods have been seen as a promising approach for the automatic and robust prediction of treatment outcomes in psychosis. In this context, several studies have been conducted to identify predictive biomarkers that may contribute to direct the choice of antipsychotic treatment in patients with psychotic disorders.
The present article offers a narrative review of the original research studies that made use of ML approaches and multi-source features to predict clinical outcomes in patients with FEP or chronic SCZ treated with antipsychotics. The purpose of this review was to explore the role of various ML methods to determine suitable biomarkers for outcomes in the treatment of psychosis. Advancements in neuroimaging, electrophysiology, genetics, and clinical and cognitive testing in recent years have opened opportunities for the identification of quantitative biomarkers that may help the prediction of clinical outcomes in psychosis.
The majority of included studies considered structural and functional neuroimaging biomarkers as predictive features used in ML analysis. Indeed, in recent years ML approaches have been successfully applied for the analysis of neuroimaging data for the investigation of SCZ [56]. It is important to note that, despite considerable clinical and analytical heterogeneity, most of the reviewed studies found that the use of neuroimaging biomarkers predictors was associated with the high accuracy of ML models. Specifically, several studies showed that resting-state FC measures could represent effective predictive biomarkers of antipsychotic treatment efficacy. This is in line with the results of a recent meta-analysis showing that rs-fMRI network segregation and integration metrics are consistent determinants of treatment response in SCZ [57].
Additionally, we included studies investigating other neurobiological markers, such as electrophysiological and genetic data, as predictors of treatment response in psychosis. Interestingly, in line with the fMRI evidence, studies that used pre-treatment EEG data as features found significant accuracy in the prediction of clinical response to clozapine therapy in treatment-resistant SCZ, suggesting that EEG features might be effective predictors of response to antipsychotic treatment in patients with specific characteristics [43]. Moreover, although genome-wide genotype data show promise in aiding clinical decision-making in psychiatry [58], only one study has found a potential contribution of polygenic risk scores in the prediction of antipsychotic medication treatment outcomes in SCZ [46].
It is important to mention that many studies investigated potential sociodemographic and baseline psychopathological predictors of antipsychotic treatment outcomes in psychosis. Included studies showed that clinical features, such as specific sociodemographic characteristics, symptom severity, and comorbidities, allow individualized prognostic predictions in people with SCZ or FEP. Noteworthy, establishing robust and generalizable clinical predictors of response to antipsychotics could improve the pathophysiological understanding of SCZ and the development of new treatments based on patient characteristics [59]. Moreover, accessible clinical predictors could have implications for identifying patients that would likely benefit from specific treatments, thus enhancing the personalized management of patients [60].
Nevertheless, although single-modality features allow individualized prognostic prediction with significant accuracy, this accuracy may not be sufficient for translation in real-world clinical practice. In recent years, several studies suggested to improve predictive value by combining information from different types of data using a multi-modality ML framework [61,62,63]. Specifically, most of included studies combined MRI measures with other neuroimaging, genetic, or clinical features. Examining the additive effects of combining two or more types of features, the predictive value of neuroimaging metrics could be improved [46, 48]. Although these findings must be interpreted with caution, evidence from most of the reviewed studies applying multimodal ML supports the utility of combining multiple features to provide comprehensive information for the personalized management of psychotic patients.
However, heterogeneity in ML methods, prognostic features, treatment approaches, and clinical presentation complicate the identification of robust and reproducible clinical and biological markers of treatment outcomes in psychosis [59]. In this context, several factors need to be taken into consideration as they influence the performance of the classifiers, limiting the joint interpretation of the study findings.
Specifically, approximately half of the studies reviewed employed less than 60 subjects, which is a limitation because a small sample size could lead to overfitting, showing a high accuracy that would not be replicated when the model is applied to a new dataset. As shown by the studies reviewed, the ones with the lowest accuracies were the ones with the biggest dataset. Nevertheless, good performance was reached even with big datasets showing that ML can be used to reliably predict the treatment outcome. Thereby, dataset size should be taken into consideration by researchers when applying ML algorithms to their data showing realistic performance measures. Also, when using classifiers, classes should be balanced, otherwise, the accuracy could be misleading. In our study, most works with unbalanced datasets overcome this problem using balanced accuracy as a performance measure to evaluate classifiers. Finally, an independent dataset should be used to test the classifiers and show the potentiality and replicability of the algorithm. Most of the studies reviewed did not employ a test set, while its importance is clear when the accuracy measures for both the training and the test set are reported showing a lower accuracy for the test set [35, 37, 49]. Among the limitations of the studies reviewed, there is the absence in some cases of quantitative performance measures like precision, sensitivity, and specificity. Besides, it should be considered that an important issue of the ML approach is to choose the suitable dataset to be analyzed to predict the outcome of interest and since there are not any studies reporting negative results, we can speculate that papers tend to be published only when they show some consistent results. Therefore, unreliable datasets are usually dismissed and not reported in the literature; this is a bias that needs to be considered.
Finally, prognostic factors of treatment outcome were investigated at different phases of psychosis. Indeed, many studies used ML methods to identify antipsychotic outcome predictors in drug-naïve FEP patients, providing computational models to optimize the treatment at the early stage of SCZ. Notably, increase treatment efficacy and reduce adverse effects of antipsychotics is a crucial task in individuals with FEP, with a relevant impact on illness outcomes [64, 65]. Conversely, several studies used ML techniques to predict treatment response in the chronic course of SCZ. Remarkably, considering that chronic SCZ has a high burden for patients and healthcare services, the identification of prognostic factors that could help clinical management and treatment effectiveness is important to prevent illness progression [66]. However, differences in clinical manifestations and a large number of features must be evaluated, and many treatment strategies have to be tested. In this context, recent research has highlighted the importance of outcome prediction in treatment-resistant SCZ [67]. Several studies included in this review focused on clinical and neurobiological predictors of treatment-resistant SCZ outcomes, showing that ML approaches may improve the prediction accuracy of responsiveness to clozapine treatment [41,42,43].
In conclusion, future research in this field should create prediction models presenting adequate predictive ability applied at different stages of SCZ illness. Indeed, SCZ and psychotic disorders are among the principal causes of global disability and are also associated with significant economic costs for patients, caregivers, and society overall [54, 68]. A recent study highlights that the total estimated burden of SCZ doubled in the last years [68] and its cost is estimated to be greater than the annual costs of all cancers combined [69]. Antipsychotic drugs are central to treatment, but clinicians are currently unable to predict response using standard clinical interviews [46], which contributes to relatively low response rates, longer and more frequent hospital stays, and an increase in overall disease burden. Hence, the development of more sophisticated predictive methods to be used in everyday clinical practice seems necessary to optimize treatment plans as early as possible. Although this is likely to increase clinical management costs in the short term, effective prediction tools would certainly reduce overall costs over a medium-to-long timeframe. Indeed, the inclusion of methods such as MRI or other neurobiological markers to rapidly optimize treatment plans would lead to a reduction of relapses over time, a lower hospitalization rate, and an improved course of illness for the patient, which ultimately reduces costs for the health system.
Limitations
Several limitations need to be considered when interpreting the findings of this review. First, included studies were heterogeneous in design, choice of prognostic features, ML algorithms, implementation, and result validation. These methodological differences must be taken into consideration when evaluating and comparing predictive models. Second, many studies used relatively small samples, especially those that considered electrophysiological and neuroimaging features as input to the ML algorithms. Indeed, small datasets can lead to the overfitting of ML models and produce results that will not replicate in independent samples. Third, many studies presented a lack of replication samples, limiting the validation of predictive models on independent cohorts. Furthermore, the heterogeneity of prognostic features limited the synthesis of results and the generation of robust overall conclusions. Finally, participants recruited in the included studies presented heterogeneous clinical characteristics (e.g., illness stage), which can require specific predictive biomarkers and treatment management. These factors should be carefully examined before recommending the use of clinical or neurobiological predictors of antipsychotic treatment outcomes in subjects with psychosis. Future studies need to focus on refining feature characterization to improve prediction accuracy, validate prediction models, and evaluate their implementation in clinical practice.
Conclusion
This literature review examined the findings from ML approaches used to predict antipsychotic treatment outcomes in patients with psychosis. Many neuroimaging, neurophysiological, genetic, sociodemographic, and clinical features were identified as putative predictors of clinical outcomes in patients with FEP and chronic SCZ treated with antipsychotics. Despite considerable clinical and analytical heterogeneity, most of the included studies considering single-modality or multi-modality features predicted responses to antipsychotics with good accuracy. Interestingly, by examining the additive effects of combining multi-source features, the predictive value of ML models could be improved. However, heterogeneity among studies in terms of considered features, ML methodology, and clinical characteristics like stages of the illness complicate the identification of both clinical and biological markers of response, remission, and recovery after antipsychotic treatment. In conclusion, although ML is a promising approach in the research of treatment outcome prediction in psychosis, further research is required to identify the actual benefits of ML in this area. With ML tools becoming more accessible for researchers and clinicians, it is expected that the field will continue to grow and that novel applications will follow.
References
World Health Organisation. The WHO World Health Report 2001 - Mental Health: New Understanding, New Hope. Geneva: World Health Organization, 2001.
Kahn RS, Sommer IE, Murray RM, Meyer-Lindenberg A, Weinberger DR, Cannon TD, et al. Schizophrenia. Nat Rev Dis Prim. 2015;1:15067. Published online
Jauhar S, Johnstone M, McKenna PJ. Schizophrenia. Lancet 2022;399:473–86.
McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia - An Overview. JAMA Psychiatry. 2020;77:201–10./span>
Schizophrenia Working Group of the Psychiatric Genomics Consortium. Biological insights from 108 schizophrenia-associated genetic loci. Nature 2014;511:421–2.
Fornito A, Zalesky A, Pantelis C, Bullmore ET. Schizophrenia, neuroimaging and connectomics. Neuroimage. 2012;62:2296–314.
Dong D, Wang Y, Chang X, Luo C, Yao D. Dysfunction of large-scale brain networks in schizophrenia: a meta-analysis of resting-state functional connectivity. Schizophr Bull. 2018;44:168–81.
O’Neill A, Mechelli A, Bhattacharyya S. Dysconnectivity of large-scale functional networks in early psychosis: A meta-analysis. Schizophr Bull. 2019;45:579–90.
Del Fabro L, Schmidt A, Fortea L, Delvecchio G, D'agostino A, Radua J, et al. Functional brain network dysfunctions in subjects at high-risk for psychosis: a meta-analysis of resting-state functional connectivity. Neurosci Biobehav Rev. 2021;128:128–101.
Goff DC. The pharmacologic treatment of schizophrenia-2021. JAMA. 2021;325:175–6.
Haddad PM, Correll CU. The acute efficacy of antipsychotics in schizophrenia: a review of recent meta-analyses. Ther Adv Psychopharmacol. 2018;8:303–18.
Lally J, MacCabe JH. Antipsychotic medication in schizophrenia: a review. Br Med Bull. 2015;114:169–79.
Correll CU, Martin A, Patel C, Benson C, Goulding R, Kern-Sliwa J, et al. Systematic literature review of schizophrenia clinical practice guidelines on acute and maintenance management with antipsychotics. Schizophrenia. 2022;8:5.
Rutledge RB, Chekroud AM, Huys QJ. Machine learning and big data in psychiatry: toward clinical applications. Curr Opin Neurobiol 2019;55:152–9.
Chekroud AM, Bondar J, Delgadillo J, Doherty G, Wasil A, Fokkema M, et al. The promise of machine learning in predicting treatment outcomes in psychiatry. World Psychiatry. 2021;20:154–70.
Dwyer DB, Falkai P, Koutsouleris N. Machine learning approaches for clinical psychology and psychiatry. Annu Rev Clin Psychol 2018;14:91–118.
Sidey-Gibbons JAM, Sidey-Gibbons CJ. Machine learning in medicine: a practical introduction. BMC Med Res Methodol. 2019;19:64.
Iniesta R, Stahl D, McGuffin P. Machine learning, statistical learning and the future of biological research in psychiatry. Psychol Med. 2016;46:2455–65.
Sajjadian M, Lam RW, Milev R, Rotzinger S, Frey BN, Soares CN, et al. Machine learning in the prediction of depression treatment outcomes: A systematic review and meta-analysis. Psychol Med. 2021;51:2742–51.
Pigoni A, Delvecchio G, Madonna D, Bressi C, Soares J, Brambilla P. Can machine learning help us in dealing with treatment resistant depression? A review. J Affect Disord. 2019;259:21–26.
Komatsu H, Watanabe E, Fukuchi M. Psychiatric neural networks and precision therapeutics by machine learning. Biomedicines. 2021;9:403.
Koutsouleris N, Kambeitz-Ilankovic L, Ruhrmann S, Rosen M, Ruef A, Dwyer DB, et al. Prediction models of functional outcomes for individuals in the clinical high-risk state for psychosis or with recent-onset depression: a multimodal, multisite machine learning analysis. JAMA Psychiatry. 2018;75:1156–72.
Koutsouleris N, Kahn RS, Chekroud AM, Leucht S, Falkai P, Wobrock T, et al. Multisite prediction of 4-week and 52-week treatment outcomes in patients with first-episode psychosis: a machine learning approach. Lancet Psychiatry. 2016;3:935–46.
Mourao-Miranda J, Reinders AA, Rocha-Rego V, Lappin J, Rondina J, Morgan C, et al. Individualized prediction of illness course at the first psychotic episode: A support vector machine MRI study. Psychol Med. 2012;42:1037–47.
Goda Taarcijonas BS, Deepak K, Sarpal MD. Neuroimaging markers of antipsychotic treatment response in schizophrenia: an overview of magnetic resonance imaging studies. Neurobiol Dis. 2019;131:104209.
Dazzan P, Arango C, Fleischacker W, Galderisi S, Glenthøj B, Leucht S, et al. Magnetic resonance imaging and the prediction of outcome in first-episode schizophrenia: a review of current evidence and directions for future research. Schizophr Bull 2015;41:574–83.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev Esp Nutr Hum y Diet. 2016;20:1.
Ambrosen KS, Skjerbæk MW, Foldager J, Axelsen MC, Bak N, Arvastson L, et al. A machine-learning framework for robust and reliable prediction of short- and long-term treatment response in initially antipsychotic-naïve schizophrenia patients based on multimodal neuropsychiatric data. Transl Psychiatry. 2020;10:276.
Blessing EM, Murty VP, Zeng B, Wang J, Davachi L, Goff DC. Anterior hippocampal–cortical functional connectivity distinguishes antipsychotic naïve first-episode psychosis patients from controls and may predict response to second-generation antipsychotic treatment. Schizophr Bull 2019;46:680–9.
Cao B, Cho RY, Chen D, Xiu M, Wang L, Soares JC, et al. Treatment response prediction and individualized identification of first-episode drug-naïve schizophrenia using brain functional connectivity. Mol Psychiatry 2018;25:906–13.
Cui X, Deng Q, Lang B, Su Q, Liu F, Zhang Z, et al. Less reduced gray matter volume in the subregions of superior temporal gyrus predicts better treatment efficacy in drug-naive, first-episode schizophrenia. Brain Imaging Behav. 2021;15:1997–2004.
Ebdrup BH, Axelsen MC, Bak N, Fagerlund B, Oranje B, Raghava JM, et al. Accuracy of diagnostic classification algorithms using cognitive-, electrophysiological-, and neuroanatomical data in antipsychotic-naïve schizophrenia patients. Psychol Med. 2019;49:2754–63.
Li H, Guo W, Liu F, Chen J, Su Q, Zhang Z, et al. Enhanced baseline activity in the left ventromedial putamen predicts individual treatment response in drug-naive, first-episode schizophrenia: results from two independent study samples. EBioMedicine. 2019;46:248–55.
Li H, Ou Y, Liu F, Chen J, Zhao J, Guo W, et al. Reduced connectivity in anterior cingulate cortex as an early predictor for treatment response in drug-naive, first-episode schizophrenia: A global-brain functional connectivity analysis. Schizophr Res. 2020;215:337–43.
Soldatos RF, Cearns M, Nielsen MØ, Kollias C, Xenaki LA, Stefanatou P, et al. Prediction of early symptom remission in two independent samples of first-episode psychosis patients using machine learning. Schizophr Bull. 2022;48:122–33.
Wood SJ, Berger GE, Lambert M, Conus P, Velakoulis D, Stuart GW, et al. Prediction of functional outcome 18 months after a first psychotic episode: a proton magnetic resonance spectroscopy study. Arch Gen Psychiatry. 2006;63:969–76.
Wu CS, Luedtke AR, Sadikova E, Tsai HJ, Liao SC, Liu CC, et al. Development and validation of a machine learning individualized treatment rule in first-episode schizophrenia. JAMA Netw Open. 2020;3:1921660.
Legge SE, Dennison CA, Pardiñas AF, Rees E, Lynham AJ, Hopkins L, et al. Clinical indicators of treatment-resistant psychosis. Br J Psychiatry. 2020;216:259–66.
Smucny J, Davidson I, Carter CS. Comparing machine and deep learning-based algorithms for prediction of clinical improvement in psychosis with functional magnetic resonance imaging. Hum Brain Mapp. 2021;42:1197–205.
Anderson JP, Icten Z, Alas V, Benson C, Joshi K. Comparison and predictors of treatment adherence and remission among patients with schizophrenia treated with paliperidone palmitate or atypical oral antipsychotics in community behavioral health organizations. BMC Psychiatry. 2017;17:346.
Ciprian C, Masychev K, Ravan M, Reilly JP, Maccrimmon D. A machine learning approach using effective connectivity to predict response to clozapine treatment. IEEE Trans Neural Syst Rehabil Eng. 2020;28:2598–607.
Fonseca de Freitas D, Kadra-Scalzo G, Agbedjro D, Francis E, Ridler I, Pritchard M, et al. Using a statistical learning approach to identify sociodemographic and clinical predictors of response to clozapine. J Psychopharmacol. 2022;36:498–506.
Masychev K, Ciprian C, Ravan M, Manimaran A, Deshmukh AA. Quantitative biomarkers to predict response to clozapine treatment using resting EEG data. Schizophr Res. 2020;223:289–96.
Podichetty JT, Silvola RM, Rodriguez-Romero V, Bergstrom RF, Vakilynejad M, Bies RR, et al. Application of machine learning to predict reduction in total PANSS score and enrich enrollment in schizophrenia clinical trials. Clin Transl Sci. 2021;14:1864–74.
Masayuki U, Hisanobu K. Cerebellar vermal size predicts drug response in schizophrenic patients: a magnetic resonance imaging (MRI) study. Prog Neuropsychopharmacol Biol Psychiatry. 1988;12:837–48.
Wang M, Hu K, Fan L, Yan H, Li P, Jiang T, et al. Predicting treatment response in schizophrenia with magnetic resonance imaging and polygenic risk score. Front Genet. 2022;13:848205.
Khodayari-Rostamabad A, Hasey GM, MacCrimmon DJ, Reilly JP, de Bruin H. A pilot study to determine whether machine learning methodologies using pre-treatment electroencephalography can predict the symptomatic response to clozapine therapy. Clin Neurophysiol 2010;121:1998–2006.
Cui LB, Fu YF, Liu L, Wu XS, Xi YB, Wang HN, et al. Baseline structural and functional magnetic resonance imaging predicts early treatment response in schizophrenia with radiomics strategy. Eur J Neurosci. 2021;53:1961–75.
Cui LB, Zhang YJ, Lu HL, Liu L, Zhang HJ, Fu YF, et al. Thalamus radiomics-based disease identification and prediction of early treatment response for schizophrenia. Front Neurosci. 2021;15:682777.
Homan P, Argyelan M, DeRosse P, Szeszko PR, Gallego JA, Hanna L, et al. Structural similarity networks predict clinical outcome in early-phase psychosis. Neuropsychopharmacology. 2019;44:915–22.
Li Y, Zhang L, Zhang Y, Wen H, Huang J, Shen Y, et al. A random forest model for predicting social functional improvement in Chinese patients with schizophrenia after 3 months of atypical antipsychotic monopharmacy: A cohort study. Neuropsychiatr Dis Treat. 2021;17:847–57.
Sarpal DK, Argyelan M, Robinson DG, Szeszko PR, Karlsgodt KH, John M, et al. Baseline striatal functional connectivity as a predictor of response to antipsychotic drug treatment. Am J Psychiatry. 2016;173:69–77.1
Shan X, Liao R, Ou Y, Ding Y, Liu F, Chen J, et al. Increased homotopic connectivity in the prefrontal cortex modulated by olanzapine predicts therapeutic efficacy in patients with schizophrenia. Neural Plast. 2021;2021:9954547.
Veronese M, Santangelo B, Jauhar S, D'ambrosio E, Demjaha A, Salimbeni H, et al. A potential biomarker for treatment stratification in psychosis: evaluation of an [18F] FDOPA PET imaging approach. Neuropsychopharmacology. 2021;46:1122–32.
Chen JH, Asch SM. Machine learning and prediction in medicine — Beyond the peak of inflated expectations. N. Engl J Med. 2017;376:2507–9.
Veronese E, Castellani U, Peruzzo D, Bellani M, Brambilla P. Machine learning approaches: from theory to application in schizophrenia. Comput Math Methods Med. 2013;2013:867924.
Mehta UM, Ibrahim FA, Sharma MS, Venkatasubramanian G, Thirthalli J, Bharath RD, et al. Resting-state functional connectivity predictors of treatment response in schizophrenia – A systematic review and meta-analysis. Schizophr Res. 2021;237:153–65.
Murray GK, Lin T, Austin J, McGrath JJ, Hickie IB, Wray NR. Could polygenic risk scores be useful in psychiatry?: a review. JAMA Psychiatry. 2021;78:210–9.
Carbon M, Correll CU. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin Neurosci. 2014;16:505–24.
Ortiz BB, Higuchi CH, Noto C, Joyce DW, Correll CU, Bressan RA, et al. A symptom combination predicting treatment-resistant schizophrenia – A strategy for real-world clinical practice. Schizophr Res. 2020;218:195–200.
Koutsouleris N, Dwyer DB, Degenhardt F, Maj C, Urquijo-Castro MF, Sanfelici R, et al. Multimodal machine learning workflows for prediction of psychosis in patients with clinical high-risk syndromes and recent-onset depression. JAMA Psychiatry. 2021;78:195–209.
Lei D, Pinaya WHL, Young J, van Amelsvoort T, Marcelis M, Donohoe G, et al. Integrating machining learning and multimodal neuroimaging to detect schizophrenia at the level of the individual. Hum Brain Mapp. 2020;41:1119–35.
Pettersson-Yeo W, Benetti S, Marquand AF, Joules R, Catani M, Williams SC, et al. An empirical comparison of different approaches for combining multimodal neuroimaging data with support vector machine. Front Neurosci. 2014;8:189.
Crespo-Facorro B, Pelayo-Teran JM, Mayoral-van Son J. Current data on and clinicalinsights into the treatment of first episode nonaffective psychosis: a comprehensive review. Neurol Ther. 2016;5:105–30.
Suvisaari J, Mantere O, Keinänen J, Mäntylä T, Rikandi E, Lindgren M, et al. Is it possible to predict the future in first-episode psychosis. Front Psychiatry. 2018;9:580.
Jobe TH, Harrow M. Long-term outcome of patients with schizophrenia: A review. Can J Psychiatry. 2005;50:892–900.
Smart SE, Keȩpińska AP, Murray RM, Maccabe JH. Predictors of treatment resistant schizophrenia: a systematic review of prospective observational studies. Psychol Med. 2021;51:44–53.
Kadakia A, Catillon M, Fan Q, Williams GR, Marden JR, Anderson A, et al. The economic burden of schizophrenia in the United States. J Clin Psychiatry. 2022;83:22m14458.
Thaker GK, Carpenter WT. Advances in schizophrenia. Nat Med. 2001;7:667–71.
Acknowledgements
This study was partially supported by the Italian Ministry of Health, with the grants Ricerca Corrente 2023 to PB and GR-2019-12370616 to EM, and by the BIAL Foundation Grant Program 2020/21, n. 288/2020 to EM and EB.
Author information
Authors and Affiliations
Contributions
LDF, EM, and ADA designed the study and methodology. LDF with EB searched the literature, selected, and reviewed the collected studies. LDF, EB, FS, and ADA wrote the first draft of the manuscript. EM and PB revised the manuscript. All authors agreed with the final content of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Del Fabro, L., Bondi, E., Serio, F. et al. Machine learning methods to predict outcomes of pharmacological treatment in psychosis. Transl Psychiatry 13, 75 (2023). https://doi.org/10.1038/s41398-023-02371-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-023-02371-z
