
Abstract
Study design
Psychometric study.
Objectives
The aim of this study was to evaluate the internal consistency and validity of the Community Integration Questionnaire – Revised (CIQ-R) in Italian individuals with spinal cord injury (SCI).
Setting
Patients’ associations, foundations, sport clubs, and federations in Italy.
Methods
The psychometric properties were evaluated following international guidelines. Internal consistency was assessed using Cronbach’s alpha (α) coefficient, and test-retest reliability was assessed using intraclass correlation coefficient (ICC); concurrent validity was assessed through Pearson’s Correlation Coefficient with the Short Form-12 health survey (SF-12).
Results
The test was administered to 80 people with SCI. Cronbach’s α showed a value of 0.825 for the Home Integration subscale, while the other subscales and the total showed values <0.70. 30 of the 80 recruited individuals were submitted to test-retest, which showed ICC values ranging from 0.94 to 1. CIQ-R also showed a correlation between Physical Component Summary (PCS12) of the SF-12, and between Social Integration subscale’s score and PCS12 and Mental Component Summary (MCS12). Correlations are also shown between Productivity subscale and PCS12 and MCS12, as well as between the total score and PCS12 and MCS12.
Conclusion
This study provided Italian clinicians and researchers with the first international outcome measure for measuring community integration. The validation of this measurement tool for people with SCI allows to compare outcomes of various studies. It is useful for testing the effectiveness of a treatment in various diseases and define which treatment is more effective than others.
Similar content being viewed by others


Introduction
The restoration of social participation and community integration for individuals with disability is an important goal for all fields of rehabilitation and a particular focus for all kinds of healthcare professionals. Spinal Cord Injury (SCI) is an acute event after which individuals experiment a change in their functional and occupational performance, but also a reduction of social integration and participation in domestic and family environment, work and/or school activities and in their free time [1,2,3]. This is due not only to the symptoms related to the injury, but also to a number of factors such as the presence of psychological and emotional consequences and/or mobility sequelae, demographic variables, economic situation, level of education, social support but also environmental barriers that alter usual occupational roles and negatively influence Quality of Life (QoL) [2, 4,5,6]. Therefore, the definition of “community integration” also include elements such as independence, interpersonal relationships, and the possibility to actively participate in significant activities of daily living (ADLs) [7]. The importance of community integration’s features implies that an accurate measurement of the construct is an imperative for the rehabilitation in people with SCI, leading to the necessity to consider environmental assessment as a specific intervention. For this reason, having valid and reliable tools in clinical practice is fundamental, in order to obtain quantitative measures of community integration of people with SCI and identify the factors that adversely affect it, in order to improve and/or correct them.
Nowadays, scientific literature presents several tools that allow to measure functional disturbances and/or alterations in people with SCI. The large number of these tools is due to the fact that in clinical practice lot of attention is given to the functional recovery, as well as the autonomous performance of the basic ADLs. On the contrary, less attention is given to the frequent restrictions on social and community integration [8, 9].
Reintegration and social participation are considered fundamental in rehabilitation and specifically in Occupational Therapists’ practice, in order to allow individuals to regain their previous occupational roles or, if this is not possible, to create new ones [10, 11]. Because of this, it is necessary to have a valid and reliable tool that allows to measure the degree of community integration. Several scales have been already developed and used, but nowadays, the Community Integration Questionnaire – Revised (CIQ-R) is one of the most commonly used worldwide and translated in several languages [12,13,14]. The CIQ-R was validated for the Italian healthy population in 2021 [15]. Despite being designed for the assessment of people with traumatic brain injury (TBI), several research has been conducted on people with SCI [3, 16, 17], but the Italian version of the CIQ-R has not yet been validated on a sample of the same population. Moreover, in Italy, there is still no specific tool for this purpose.
For these reasons, the aim of the following study was to evaluate the internal consistency and validity of the CIQ-R in Italian in a group of individuals with SCI.
Methods
This study was conducted by a research group composed of medical doctors and rehabilitation professionals from the “Sapienza” University of Rome and from the “Rehabilitation & Outcome Measure Assessment” (R.O.M.A.) association. In the last few years, the R.O.M.A. association has dealt with the validation of many outcome measures in Italy [18,19,20,21,22,23,24,25,26,27,28].
Instruments
The CIQ-R is an 18-items assessment tool designed to be a brief [15] questionnaire for measuring home, social, productivity integration, and electronic social networking [28]. It is the revised version of the Community Integration Questionnaire (CIQ) [29] and was designed at first to be administered to people with Traumatic Brain Injury (TBI) [30,31,32,33,34,35]. Recently, it has also been used in people with SCI and other physical disability [36], aphasia [6, 37], brain tumors [38], burn injuries [39], as well as young people with acquired and congenital disabilities living in nursing homes [40]. In the last 2 year a Croatian [41] and a Malay version [42] were published, the Italian version of the instrument is now been validated and has been administered in healthy population with no evidence of disability[15].
The questionnaire is divided in four sections: Home integration: active participation in home activities; Social integration: active participation in outdoor activities and interpersonal relations; Productivity: involvement in employment, education, and volunteer activities; Electronic Social Networking (ESN): participation in electronic social networking.
Scores are created by self-report of performance frequency, with additional weight given on necessity of assistance. Most CIQ-R items are scored from 0 to 2 and the subtotals for Home Integration (0–12), Social Integration (0–10), Productivity (0–7), and ESN (0–6) subscales are calculated, as well as the total score (0–35). A higher score indicates a higher level of community integration.
The CIQ-R can be completed directly with the person or by proxy, administered in person, by telephone, or can be self-administered. It takes approximately 10–15 min to complete.
Participants of this study were also asked to complete the Short Form 12 (SF-12) health survey, used as comparison tool. The SF-12 is a brief, self-administered, measure of health-related QOL. The 12 items allow to get a Physical Component Score (PCS) and a Mental Component Score (MCS), in which higher score indicate a better health status [43].
Participants
According to the inclusion criteria adopted, participants have to: (1) be at least 18 years of age or older; (2) have a SCI diagnosis for at least 6 months; (3) not be hospitalized in a post-acute ward.
Before administering the test, each eligible individual was informed about methods and objectives of the study, people interested in being enrolled signed a written consent, releasing their personal data.
Reliability and validity
Participants were asked to complete the CIQ-R first, and then the SF-12 for comparing health-related QoL assessment. To assess test-retest reliability, a subgroup of the sample was evaluated twice: they took the first test on day 1 and again after 14 days (day 14). For the evaluation of interrater reliability, on day 1, all participants form the whole population were evaluated by two different professionals.
The psychometric characteristics of the tool were assessed following the Consensus-Based Standards for the Selection of Health Status Measurement Instruments (COSMIN) checklist [44].
Internal consistency was examined using Cronbach’s alpha (α), to assess the interrelatedness of the items and the homogeneity on the scale. Values of Cronbach’s α higher than 0.70 were considered acceptable as an indicator of the satisfactory homogeneity of all the items within the total scale.
The interclass correlation coefficient (ICC) was evaluated to determine the test’s reliability. The ICC ranges from 0 (no agreement) to 1 (perfect agreement) and has been interpreted as follows: 0.00–0.25 = little, if any, correlation; 0.26–0.49 = a low correlation; 0.50–0.69 = a moderate correlation; 0.70–0.89 = a high correlation; and 0.9–1 = a very high correlation.
Criterion validity was evaluated using Pearson’s correlation coefficient to evaluate the correlation with the SF-12 health survey. The Pearson’s correlation coefficient was interpreted as follows: 0 indicated no linear relationship; +1/−1 indicated a perfect linear positive/negative relationship; a value between 0 and 0.3 (or 0 and −0.3) indicated a weak linear positive (negative) relationship; values from 0.3 to 0.7 (−0.3 and −0.7) indicated a moderate positive (negative) linear relationship; and values between 0.7 and 1.0 (−0.7 and −1.0) indicated a strongly positive (negative) linear relationship. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 23.0 for Windows, developed by the International Business Machine Corporation (IBM). The descriptions of the variables were carried out by using frequency tables, means, and standard deviation (SD).
Results
Participants
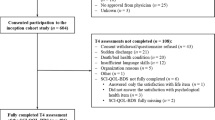
A total of 80 individuals with SCI, recruited from January to March 2019 from patients’ associations, foundations, sport clubs, and federations within the national territory, participated to this study and were assessed with the Italian version of CIQ-R. At the time of administration, recruited sample had an average age of 46 years (SD 11.74). All results and demographic characteristics are shown in Table 1.
Reliability and validity
The internal consistency and the construct validity were calculated on all 80 included individuals. The Home Integration subscale only showed and Cronbach’s alpha value ≥0.70 while for the three subscale (Social Integration, Productivity, Electronic Social Networking Integration) as well as for the total score Cronbach’s alpha coefficients were <0.70. Results are shown in Table 2.
Test-retest reliability procedures were performed for 30 out of the 80 included individuals. The analysis was carried out ICC, with values ranging from a minimum of 0.94 to a maximum of 1, results are presented in Table 3.
Pearson’s correlation coefficient showed a correlation between the total score of CIQ-R and Physical Component Summary (PCS12) of the SF-12 health survey and between Social Integration subscale’s score and PCS12 and Mental Component Score (MCS12). Correlations are also shown between the “Productivity” subscale and PCS12 and MCS12, as well as between the total score and PCS12 and MCS12 of the gold standard. Results are shown in Table 4.
Discussion
The aim of this study was to evaluate the internal consistency and validity of the Community Integration Questionnaire – Revised (CIQ-R) in Italian individuals with SCI.
Cronbach’s alpha coefficient showed a good internal consistency for the Home Integration (HI) subscale only (α = 0.825), coherently with the validation carried out on people with SCI by the two main developers of the CIQ-R [16]. More specifically, the value of the Italian alpha turns out to be the highest, compared to the α = 0.79 in the validation of Kratz et al. Moreover, HI subscale shows α values ≥0.70 even when an item is deleted. It is, therefore, possible to affirm that HI subscale results to have the greatest sensitivity in measuring the level of individual’s integration in family life and participation to domestic activities. On the contrary, Social Integration, Productivity and Electronic Social Networking Integration subscales showed lower alpha values, respectively α = 0.40, α = 0.13, and α = 0.43. The same results for the total score, in which we have α = 0.627, not statistically significant and slightly lower than the validation cited before.
The lowest alpha values are found for the Productivity subscale: this is probably due to the fact that this subscale is composed of two elements only, which are different from each other and show very high scores compared to the maximum score obtained in the other three subscales.
However, similar results were obtained in the validation on healthy subjects with the following values of Cronbach’s alpha 0.639 (Total), 0.820 (Home Integration), 0.395 (Social Integration), 0.003 (Productivity), 0.539 (ESN Integration),
About test-retest reliability, ICC has been calculated and its values are statistically significant, with values between 0.94 and 1: it means that the assessment tool has an excellent stability after repeated measurements. In this case, results are consistent with all the validations present in scientific literature, regardless of the type of sample taken into consideration [2, 12, 45]. Consequently, it is possible to affirm that the tool has an excellent test-retest reliability: giving the same test to the same individuals on two different occasions, its results are consistent over time.
About concurrent validity, there is a correlation between Social Integration (SI) subscale and the physical and mental components (PCS12 and MCS12) of the SF-12 health survey, with Pearson’s correlation coefficient respectively r = 0.236 with p < 0.01 and r = 0.327 with p < 0.05. There is also a correlation between Productivity subscale and PCS12, with values of r = 0.310, and between the total score of the CIQ-R with PCS12 (r = 0.251) and MCS12 (r = 0.291). These results are similar with those of the Italian validation on healthy people and the Persian validation study [12] and the validation in a sample of individuals with physical disabilities [36]. This statement refers in particular to the correlation between SI and MCS12 (with values of r = 0.327 in Italy, r = 0.39 in Persia and r = 0.30 in subjects with physical disability), as well as between Productivity and PCS12 (with values of r = 0.25, r = 0.38 and r = 0.30) and Total Score and MCS12 (with values of r = 0.29, r = 0.30 and r = 0.34).
The correlation of the CIQ-R with the PCS12 of the SF-12 health survey can be interpreted as that the level of reintegration of the individual is influenced by his/her level of functioning, physical health, and the presence or absence of any types of disease or pain. The questionnaire is correlated with both domains of SF-12 (PCS12 and MCS12), so that we can assume that patients’ community integration is significantly linked to his/her psychological and physical well-being. The better the functional and psychological state, the greater the degree of community reintegration and participation in all the most important living environments for the patient himself.
Limitations of the study
The present study showed some limitations.
First of all there is no correlation with a gold standard due to the fact that the specific tools for the Community Integration assessment are not validated in Italian yet.
Moreover, from the analysis of the individual scores of each participant, the results depend on numerous variables, such as demographic characteristics (age, sex, educational level), the level and completeness of lesion, the presence of architectural barriers and/or environmental facilitators.
Because of this, it is recommended to administer the CIQ-R together with other measurement tools or instruments, in order to take into account these variables and obtain the most objective measurement possible. The CIQ-R data are also limited to adults of working age (18 years or older): an expansion of this range is required in order to expand the statistical survey.
Moreover, as already underlined by other studies and validations, the tool could also be improved by the addition of specific items to evaluate preinjury status for each item, in order to represent the difference between preinjury and postinjury status [16].
Conclusion
The Italian version of the CIQ-R has showed to be a valid and reliable tool to assess the global level of community integration in people with SCI. The total results of this study showed statistically significant psychometric properties for use the Italian CIQ-R in clinical and research settings of individuals with SCI. This tool also provides useful evidence for rehabilitation and specifically for Occupational Therapy practice, because its scores allows to obtain the degree of reintegration and participation in daily life and important activities after the SCI diagnosis. Occupational Therapists can develop specific intervention plans in order to allow the re-acquisition of old occupational roles or, if this is not possible, the creation of new ones.
Data availability
The data that supports the findings of this study are available from corresponding upon reasonable request.
References
Sander AM, Fuchs KL, High WM, Hall KM, Kreutzer JS, Rosenthal M, et al. The community integration questionnaire revisited: Assessment of facor structure and validity. Arch Phys Med Rehabil. 1999;80:1303–8.
Callaway L, Winkler D, Tippett A, Herd N, Migliorini C, Willer B, et al. The community integration questionnaire - revised: Australian normative data and measurement of electronic social networking. Aust Occup Ther J. 2016;63:143–53.
Kratz AL, Chadd E, Jensen MP, Kehn M, Kroll T. An examination of the psychometric properties of the community integration questionnaire (CIQ) in spinal cord injury. J Spinal Cord Med. 2015;38:446–55.
Wilier B, Ottenbacher KJ, Coad M Lou. The community integration questionnaire a comparative examination. Am J Phys Med Rehabil. 1994;73:103–11.
Gerber GJ, Gargaro J, McMackin S. Community integration and health-related quality-of-life following acquired brain injury for persons living at home. Brain Inj. 2016;30:1552–60.
Lee H, Lee Y, Choi H, Pyun SB. Community integration and quality of life in aphasia after stroke. Yonsei Med J. 2015;56:1694–702.
Mccoll MA, Carlson P, Johnston J, Minnes P, Shue K, Davies D, et al. The definition of community integration: Perspectives of people with brain injuries. Brain Inj. 1998;12:15–30.
Scelza WM, Kirshblum SC, Wuermser LA, Ho CH, Priebe MM, Chiodo AE, et al. Spinal cord injury medicine. 4. community reintegration after spinal cord injury. Arch Phys Med Rehabil. 2007;88:S71–5.
Forchheimer M, Tate DG. Enhancing community re-integration following spinal cord injury. NeuroRehabilitation. 2004;19:103–13.
Gibson RW, Amico MD, Jaffe L, Arbesman M. Occupational therapy interventions for recovery in the areas of community integration and normative life roles for adults with serious mental illness: A systematic review. Am J Occup Ther. 2011;65:247–56.
D’Amico ML, Jaffe LE, Gardner JA. Evidence for interventions to improve and maintain occupational performance and participation for people with serious mental illness: A systematic review. Am J Occup Ther. 2018;72:7205190020p1–1.
Negahban H, Fattahizadeh P, Ghasemzadeh R, Salehi R, Majdinasab N, Mazaheri M, et al. The Persian version of community integration questionnaire in persons with multiple sclerosis: translation, reliability, validity, and factor analysis. Disabil Rehabil. 2013;35:1453–9.
Saeki S, Okazaki T, Hachisuka K. Concurrent validity of the community integration questionnaire in patients with traumatic brain injury in Japan. J Rehabil Med. 2006;38:333–5.
Tršinski D, Tadinac M, Bakran Ž, Klepo I. Utility of the Croatian translation of the community integration questionnaire-revised in a sample of adults with moderate to severe traumatic brain injury. Disabil Rehabil. 2018;41:1711–8.
Ioncoli M, Berardi A, Tofani M, Panuccio F, Servadio A, Valente D, et al. Crosscultural validation of the community integration questionnaire-revised in an italian population. Occup Ther Int. 2020;2020:8916541. https://doi.org/10.1155/2020/8916541.
Callaway L, Enticott J, Farnworth L, McDonald R, Migliorini C, Willer B, et al. Community integration outcomes of people with spinal cord injury and multiple matched controls: A pilot study. Aust Occup Ther J. 2017;64:226–34.
Ahmed N, Quadir MM, Rahman MA, Alamgir H. Community integration and life satisfaction among individuals with spinal cord injury living in the community after receiving institutional care in Bangladesh. Disabil Rehabil. 2018;40:1033–40.
Panuccio F, Berardi A, Marquez MA, Messina MP, Valente D, Tofani M, et al. Development of the Pregnancy and Motherhood Evaluation Questionnaire (PMEQ) for evaluating and measuring the impact of physical disability on pregnancy and the management of motherhood: a pilot study. Disabil Rehabil. 2020;4:1–7.
Berardi A, Regoli E, Tofani M, Valente D, Fabbrini G, Fabbrini A, et al. Tools to assess the quality of life in patients with Parkinson’s disease: a systematic review. Expert Rev Pharmacoeconomics Outcomes Res. 2021;21:55–68.
Berardi A, Panuccio F, Pilli L, Tofani M, Valente D, Galeoto G. Evaluation instruments for executive functions in children and adolescents: a systematic review. Expert Rev Pharmacoecon Outcomes Res. 2021;21:885–96. https://doi.org/10.1080/14737167.2021.1908889.
Galeoto G, Formica MC, Mercuri NB, Santilli V, Berardi A, Castiglia SF, et al. Evaluation of the psychometric properties of the Barthel index in an Italian ischemic stroke population in the acute phase: a cross-sectional study. Funct Neurol. 2019;34:29–34.
Panuccio F, Galeoto G, Marquez MA, Grassi ML, Scialpi A, Tofani M, et al. General Sleep Disturbance Scale (GSDS-IT) in people with spinal cord injury: a psychometric study. Spinal Cord. 2020;58:1183–8.
Tofani M, Candeloro C, Sabbadini M, Field D, Frascarelli F, Lucibello L, et al. A study validating the Italian version of the Level of Sitting Scale in children with cerebral palsy. Clin Rehabil. 2019;33:1810–8.
Galeoto G, Scialpi A, Grassi ML, Berardi A, Valente D, Tofani M, et al. General sleep disturbance scale: translation, cultural adaptation, and psychometric properties of the Italian version. Cranio - J Craniomandib Pr. 2019;39:326–34.
Parente M, Tofani M, De Santis R, Esposito G, Santilli V, Galeoto G. The role of the occupational therapist in disaster areas: Systematic review. Occup Ther Int. 2017;2017:6474761. https://doi.org/10.1155/2017/6474761.
D’Alvia L, Pittella E, Fioriello F, Maugeri A, Rizzuto E, Piuzzi E, et al. Heart rate monitoring under stress condition during behavioral analysis in children with neurodevelopmental disorders. In: 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA). IEEE; 2020. pp 1–6.
Levi G, Colonnello V, Giacchè R, Piredda ML, Sogos C. Building words on actions: Verb enactment and verb recognition in children with specific language impairment. Res Dev Disabil. 2014;35:1036–41.
Aceti F, Carluccio GM, Meuti V, Piperno F, Sogos C, Straniero Sergio B, et al. Parental care and post partum depression: a case report. Riv Psichiatr. 2012;47:221–5.
Lombardi F, Orsi M, Mammi P, Brianti R, Mazzucchi A. Validità del Community Integration Questionnaire (CIQ) e dati normativi per l’Italia. Giorn It Med Riab. 1997;1:23–34.
Tomaszewski R, Mitrushina M. Utility of the Community Integration Questionnaire in a sample of adults with neurological and neuropsychiatric disorders receiving prevocational training. Disabil Rehabil. 2016;38:1016–22.
Constant CR, Gerber C, Emery RJH, Søjbjerg JO, Gohlke F, Boileau P, et al. A review of the Constant score: Modifications and guidelines for its use. J Shoulder Elb Surg. 2008;17:355–61.
Migliorini C, Enticott J, Callaway L, Moore S, Willer B. Community integration questionnaire: Outcomes of people with traumatic brain injury and high support needs compared with multiple matched controls. Brain Inj. 2016;30:1201–7.
Cicerone KD, Mott T, Azulay J, Friel JC. Community integration and satisfaction with functioning after intensive cognitive rehabilitation for traumatic brain injury. Arch Phys Med Rehabil. 2004;85:943–50.
Ritchie L, Wright-St Clair VA, Keogh J, Gray M. Community integration after traumatic brain injury: A systematic review of the clinical implications of measurement and service provision for older adults. Arch Phys Med Rehabil. 2014;95:163–74.
Johnston MV, Goverover Y, Dijkers M. Community activities and individuals’ satisfaction with them: Quality of life in the first year after traumatic brain injury. Arch Phys Med Rehabil. 2005;86:735–45.
Hirsh AT, Braden AL, Craggs JG, Jensen MP. Psychometric properties of the Community Integration Questionnaire in a heterogeneous sample of adults with physical disability. Arch Phys Med Rehabil. 2011;92:1602–10.
Dalemans RJ, de Witte LP, Beurskens AJ, van den Heuvel WJ, Wade DT. Psychometric properties of the community integration questionnaire adjusted for people with aphasia. Arch Phys Med Rehabil. 2010;91:395–9.
Kaplan CP. Community integration questionnaire for patients with brain tumor: a comparative study. Am J Phys Med Rehabil. 2000;79:243–6.
Esselman PC. Burn rehabilitation: an overview. Arch Phys Med Rehabil. 2007;88:S3–6.
Winkler D, Farnworth L, Sloan S, Brown T. Moving from aged care facilities to community-based accommodation: outcomes and environmental factors. Brain Inj. 2011;25:153–68.
Tršinski D, Tadinac M, Bakran Ž, Klepo I. Utility of the Croatian translation of the community integration questionnaire-revised in a sample of adults with moderate to severe traumatic brain injury. Disabil Rehabil. 2019;41:1711–8.
Razaob NA, Tham SY, Mohd Rasdi HF, Wan Yunus F, Kadar M. Translation, validation and reliability testing of community integration questionnaire-revised (CIQ-R) malay version: a preliminary study. Occup Ther Heal Care. 2020;34:32–47.
Ware JE, Kosinski M, Keller SD. A 12-Item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–33.
Mokkink LB, de Vet HCW, Prinsen CAC, Patrick DL, Alonso J, Bouter LM, et al. COSMIN risk of bias checklist for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27:1171–9.
Fraga-Maia HMS, Werneck G, Dourado I, Fernandes R, de CP, Brito LL. Translation, adaptation and validation of “community integration questionnaire.”. Cienc e Saude Coletiva. 2015;20:1341–52.
Author information
Authors and Affiliations
Contributions
Substantial contributions to conception and design: AB, GG, MI. Drafting and revising the article critically for important intellectual content: GG, FP, MAM. Final approval of the version to be published: MT, AB, DV.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Ethics committee approval is not required for this study, this research involves secondary use of clinical data, which is provided without any identifier or group of identifiers that would allow attribution of private information to an individual. Informed consent was obtained from all participants for being included in the study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Panuccio, F., Galeoto, G., Valente, D. et al. Psychometric properties of the Community Integration Questionnaire – Revised (CIQ-R) in an Italian population with spinal cord injury. Spinal Cord Ser Cases 8, 18 (2022). https://doi.org/10.1038/s41394-022-00486-x
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-022-00486-x
