
Abstract
Study design
Cross-sectional study.
Objectives
To provide data on the rates of sexual dysfunction (SD) among the Greek spinal cord injury (SCI) women and to investigate any association with demographic and clinical variables.
Setting
Greek territory.
Methods
Our sample was enrolled from rehabilitation institutes throughout Greece and included 30 women with SCI living in the community for at least 1 year after the primary inpatient rehabilitation program. They were assessed for SD using the Female Sexual Function Index (FSFI). Pearson’s test was performed to examine the correlation of SD with clinical—demographic parameters as defined by specific questionnaires: Satisfaction With Life Scale (SWLS), World Health Organization Quality of Life-BREF (WHOQOL-BREF), Spinal Cord Independence Measure (SCIM), Patient Health Questionnaire (PHQ-9), Craig Handicap Assessment and Reporting Technique (CHART).
Results
SD was revealed in 63.3% of the study participants. The mean FSFI score was 14.4. Pearson’s analysis showed that age was negatively correlated with FSFI scores (p = 0.006), while pain had a negative impact only on desire scores (p = 0.04). FSFI scores were negatively correlated with PHQ-9 (p = 0.04), while there was a positive correlation with SWLS (p = 0.003), SCIM (p = 0.013), and specific domains of WHOQOL-BREF (psychological, relations, environment), and CHART (mobility, social integration).
Conclusions
The rate of SD (63.3%) generally agrees with the findings of high rates in most of the literature, although it is rather lower, in comparison to other populations. Old age and depressive symptoms were the major identified determinants of SD.
Similar content being viewed by others


Introduction
Spinal cord injury (SCI) is a challenging medical entity that is responsible for long-term effects in almost all aspects of an individual’s everyday life. Vast changes in sensory, motor, and autonomic functions may require adaptation in the person’s sexual life [1, 2]. For women living with SCI, although their sexuality is being acknowledged more in recent years, research has been insufficient compared to the influence on men after SCI [3]. Women with SCI have menstrual cycles and can achieve pregnancies, but in many cases are considered to have a passive role during sexual intercourse. This might occur because changes in sexual function after neurological damage are more obvious in men, or because men consist of a larger group affected [4, 5].
Studies have concluded that while 65–80% of women with SCI are sexually active, that occurs to a lesser extent, and in 25% with lower satisfaction than before the injury [3, 6,7,8]. In a study conducted by Lombardi et al. with the use of the Female Sexual Function Index (FSFI), 59% of the women were reported to have one or more clinical characteristics of sexual dysfunction (SD) [9]. This has been mostly linked to mobility and sensation issues, spasticity, bladder and bowel control, and pain management [10]. Additionally, the loss of vaginal lubrication and orgasmic dysfunction have been observed in some cases. Moreover, the psychological state of the individual, socioeconomic factors, and the information provided on the matter during rehabilitation have been associated with the sexual health of this population. However, women have been found to experience depression or other psychological disorders more often than men after the injury [10].
A variety of studies have noted the impact the sexual health after SCI in the quality of life [2, 11]. Some studies regarding the matter of sexuality in women with SCI can be found in the literature, however there are none yet regarding the Greek population. In this study, we aim to investigate whether sexuality in women with SCI living in Greece is affected by factors regarding their condition, as well as if our findings are consistent with relative studies from other countries. This cross-sectional study hypothesizes that SD rates in women with SCI in Greece are similar to those reported in the rest of the world, with body pain levels and depressive symptoms being the main determinants of SD among the population of female individuals with SCI in Greece.
Methods
Participants/study design
Having permission to access the medical records of 17 rehabilitation departments from both public and private sectors that were located all across the Greek territory, we identified a total of 221 living female persons with acquired SCI of any etiology. The data were compiled during the period from February 2018 to April 2019. These women originated from different regions of Greece and they had completed their acute rehabilitation programs (defined as discharge from a rehabilitation department at least 1 year before the study). We excluded female individuals who were not legally adults (age under 18 years) and non-Greek speakers. Our criteria were met by 205 women, with ages between 22 and 76 years. We randomly selected 20% of the women with acquired SCI from each rehabilitation department (n = 41). From the recruited sample, 30 women accepted to participate in this study. All the involved Rehabilitation Departments granted us broad access to their medical files, facilitating the retrieval of any useful piece of information. The women participated self-willingly in this study and gave their written consent for their personal information to be used anonymously for research purposes. To achieve that, informed consent brochures were administered that conformed with the Helsinki declaration principles and Greek Medical ethics law (Hellenic State Law 3418/2005). The ethics committee of the Medical School of National and Kapodistrian University of Athens approved this study.
Data collection—questionnaires
During a medical history interview and clinical examination, data concerning clinical and demographic information were collected by the physiatrist. The participants provided demographic data (age, family status, place of residence, education level, employment, the maintenance or start of a profession after the SCI). Clinical data related to the SCI were also collected, namely level of injury, degree of impairment according to ASIA Impairment Scale [12], years from injury, micturition type, and body pain severity. The level of pain was evaluated by asking participants to grade their pain on average throughout the whole week before the examination somewhere between zero and ten, in line with the Numerical Rating Scale (NRS), a widely used tool in individuals with SCI [13].
Then, the participants were assessed and scored on six questionnaires: FSFI, Satisfaction With Life Scale (SWLS), World Health Organization Quality of Life-BREF (WHOQOL-BREF), Spinal Cord Independence Measure (SCIM III), Patient Health Questionnaire-9 (PHQ-9), and Craig Handicap Assessment and Reporting Technique (CHART).
The FSFI questionnaire has been widely used to investigate the SD level in women. It targets six domains: arousal, lubrication, orgasm, desire, satisfaction, and pain. The questionnaire contains 19 multiple choice questions and it uses a five-point Likert scale with some scoring from 0–5 points and others 1–6 points. Each of the 19 questions has a specific multiplying factor ranging from 0.3 to 0.6, and corresponds to one of the six domains. In that way, each separate domain has a maximum score of 6, totaling the maximum score of the FSFI at 36 points. Also, the minimum score of each domain ranges from 0 to 1.2, making 2 points the minimum score of the questionnaire [14, 15]. Although scores of ≤26 most accurately captured clinically relevant SD (specificity = 0.733; sensitivity = 0.889), Wiegel et al. in their study proposed that we should also take into account the added utility of the individual domain scores (both within the model and conceptually) for estimating differential diagnoses across the various types of female SD [16]. For this reason, we also tested the scores of the subdomains of FSFI. The FSFI scoring has been the most used measurement tool for SD in women after SCI and is considered accurate and sensitive [17].
The SWLS is a scale used to evaluate subjective well-being and life satisfaction. The participant is required to grade on a seven-point scale their level of agreement with five sentences that target life satisfaction. The sum of each graded answer is evaluated as an overall score, which classifies the patient in one of seven categories of satisfaction or dissatisfaction [18]. The WHOQOL-BREF questionnaire has 26 questions addressing physical health, psychological health, social relationships, and environment. The answers produce a score on each of the four domains, which correspond to the level of satisfaction the person feels in each category [19].
The SCIM III consists of 19 items that evaluate three different tasks: self-care, mobility, and respiration/sphincter management. The total score ranges from 0 to 100 with higher scores representing higher functional independence and capability to perform activities of daily life regarding persons with SCI [20]. To measure the psychological state of each individual, the PHQ-9 was used. This widely used tool—including people with SCI—targets 9 different symptoms and its scores range from 0 to 27, with higher values meaning more severe depression [21]. The CHART measures six different domains (Physical independence, Cognitive independence, Mobility, Occupation, Social Integration, and Economic self-sufficiency). It evaluates the level of community participation of people with disabilities in their everyday life [22].
These questionnaires were all explained and subsequently answered by each participant during their interviews. That way, we acquired a broad database not only documenting the SD but also other measurable aspects.
Statistical analysis
We used the Statistical Package for the Social Sciences (SPSS) version 23 (SPSS Inc., Chicago, IL, USA) to calculate the prevalence of SD and its correlation with demographic data along with biological and psychological factors (age, marital status, type and duration of SCI, pain, life satisfaction, independence status, quality of life, depression, and mobility status). The normality of data was examined using Kolmogorov–Smirnov test. To examine the homogeneity of the study groups, Chi-square, and independent t-test were used. Pearson correlation (r) was used to clarify relationships between quantifiable variables. A p value < 0.05 was considered statistically significant.
Results
A total of 30 women with SCI were included in the study. Most of the participants were paraplegic (93.3%) and with an incomplete injury (53.3%). The mean time since the initiation of the disability was 14.6 ± 9.4 years, and the mean duration of their initial inpatient rehabilitation program was 2.2 ± 1.1 months. The mean pain score of the sample according to the NRS was 3.1 ± 3.2. Table 1 shows the demographic and clinical characteristics of the patient groups.
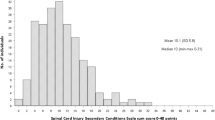
Regarding SD (total score on FSFI ≤ 26), our results reveal a rate of 63.3% among Greek women with SCI. The average FSFI score of the sample was 14.4 ± 13.7. All data, including the average FSFI subscale’s scores, are presented in Table 2.
Furthermore, we conducted Pearson’s correlation analysis for total FSFI and particular domain scores and clinical-demographic parameters such as age, years since injury, and NRS pain score. Age was found to have a negative correlation with all scores of FSFI; no association was found between the FSFI score and years since injury. The NRS pain score was negatively correlated with the Desire domain of FSFI. Table 3 shows all relevant correlations about age, years from injury, and the NRS pain score.
To examine the possible relation between SD and quality of life in our sample we conducted Pearson’s correlation analysis between FSFI scores and quality of life parameters according to WHOQOL-BREF. We found a positive significant correlation between WHOQOL-BREF Psychological subscale and Desire, Arousal, Lubrication and Orgasm FSFI domains, as well as with total FSFI score. Additionally, a positive significant correlation was found between WHOQOL-BREF Relations and Environment domains with all the domains of FSFI.
Moreover, Pearson’s correlation analysis was done to test the hypothesis that the independence of women with SCI has an impact on SD. We found a significant positive correlation between Self-care domain of SCIM and Desire, Arousal, Satisfaction, Pain domains of FSFI, as well as with the total score of FSFI. Positive correlations were found for Respiration Independence and all FSFI domains, but none in the case of Mobility Independence.
Regarding satisfaction with life, Pearson’s correlation analysis revealed a significant positive correlation between all domains of FSFI and SWLS domains. As far as for PHQ-9 score, the only significant correlations were with Arousal, Lubrication and Orgasm domains, as well as with total score of FSFI.
Finally, a Pearson’s correlation analysis was done between all domains of FSFI and CHART domains, to investigate any possible association between SD and the social reintegration levels of women after SCI. No association was found between the FSFI score (total and domains) and the Physical Independence, the Occupation, and the Economic Self-Sufficiency CHART domains. However, we identified a positive correlation between all domains of FSFI scores and CHART Mobility domain, between the Desire domain of FSFI and CHART Cognitive Independence domain, and between the CHART Social Integration domain and all FSFI domains except Pain.
All data regarding the correlation between FSFI scores and the above outcome measures are shown in Table 4.
Discussion
The rate of SD in women with SCI that consisted the sample of this study (63.3%) generally agrees with the findings of high rates in most of the international literature. However, studies from other countries of different continents, that have used the same methodology, have documented an even higher percentage of SD, around 80% [23, 24]. The difference that is observed can be possibly attributed to Greece being a fairly progressive country, therefore sexual satisfaction in general as well as in the population of this study is averaged between modern and conservative (sexually liberated) societies. The majority of women in Greece are literate, have access to the internet and medical professionals and psychologists. Additionally, this relative lower rate of SD maybe is the outcome of the limited number of tetraplegic individuals, only two women, in our sample. However, sexual education and advocacy are often suppressed mostly because of the religious and conservative background and the lack of sexual education, which makes seeking professional help for sexuality a taboo topic.
The negative correlation between age and FSFI score in our study has also been reported in similar studies [23,24,25]. This is notable because the mean age of our sample was 48 years, therefore most women we interviewed were in an age that does not affect sexual relations and the existence of a partner as much as being an elder. However, we found no connection between the FSFI score and time since injury, contrary to the results of other studies from different countries [24, 26]. This could be partly attributed to the gradual adaptation and acceptance of the impact of the lesion to their sexual function or to the higher possibility of maintaining emotional and physical intimacy in a permanent sexual relationship as years pass post-injury. Although the meantime since injury in our sample was 14.9 years, we did not question, apart from the FSFI scale, important procedures such as type of sexual encounters, the management of problems such as autonomic dysreflexia or incontinence, and communication with health professionals and partners. As other studies have reviewed such information, further knowledge and research is necessary to investigate and interpret this finding.
Our study reports a negative impact of pain on sexual desire, which is also noted in the literature as a factor that affects negatively sexual activity [7, 27]. In the study of Sramkova et al. 13% of the interviewed women specify pain as the main negative factor for sexual activity [27]. Moreover, pain has been noted to affect the psychological state and thus hinder the sexual life of individuals with SCI [28]. Pain often causes fatigue, anxiety, anger, low self-esteem, poor sleep quality, increased spasticity, and therefore inhibits active sexual life.
In our study, the quality of life has been positively linked to most aspects of the FSFI scale. In a study published by Reitz, reported results of low sexual satisfaction were not related to the quality of life [29]. However, we must note that this study included both genders and in this specific correlation a possible difference was not specified, while this study was conducted in the Swiss population, a country notable for the high levels of quality of life that it offers.
According to our results, independence after SCI (especially self-care domain) has a positive impact on SD, as has also been reported by Merghati-Khoei et al. [30]. Another study from the USA noted as well that the participation in sexual intercourse is higher amongst women with lower lesions, with the most difference between cervical and thoracic lesions [31]. This also suggests that independence affects sexual function. Contrary to that, we witnessed no connection between Mobility Independence and the FSFI. We must consider that the vast majority in our sample were women with paraplegia, who have a significantly higher level of mobility independence compared to tetraplegic individuals, and this could impact our result.
In our analysis, both low satisfaction with life and the high PHQ-9 scores were associated with low FSFI scores. The satisfaction that an individual has with their life and their psychological state often reflects their perspectives of satisfaction with their sexual life. This is supported by Lombardi et al. [9] who noted that in many previous studies depression has seemed to negatively affect the sexual health of women with SCI. Harisson et al. [4] also connected feelings of anxiety and depression with SD in such a group of individuals.
In this study no statistically significant correlation was observed between the FSFI scores and the Physical Independence, the Occupation, and the Economic Self-Sufficiency CHART domains. This contrasts the results of two Iranian studies, that documented associations of work status, education, and living situation with SD in women with SCI [23, 30]. A higher level of education was also reported by Kreuter et al. as affecting positively the sexual function [1]. However, Moreno-Lozano et al. observed no association between the SCIM score, the socioeconomic status, and the level of education with the FSFI scale [24]. On the other hand, our results indicate that women with SCI that present with higher levels of social engagement and mobility within the community are more likely to present with normal sexual function. This could be interpreted by the higher possibility of socially active women with SCI to communicate frequently with male individuals, to date, and to be involved in romantic relationships.
Although we consider this study notable in a pivotal aspect of spinal cord medicine, we must recite some potential limitations. The absence of a control group to compare the results of our sample could provide us with further information about the domains of female SD linked to SCI. Moreover, the follow-up of the participants would result in a more thorough comparison of the socioeconomic factors and their impact. Other limitations include the fairly limited number of participants and the undersized number of tetraplegic women that we achieved to include. However, due to the lack of valid national records of people living with SCI in Greece, it is quite difficult to examine and follow up a large number of volunteers. Furthermore, the recruitment process (random selection of participants from departments all across the country) provides some evidence of representativeness but does not assure that the sample is representative. Also notable is the fact that we did not question our participants in physical matters regarding sexual life such as limitations brought by their injury (incontinence, spasticity, etc.) and the way those parameters may shift the sexual function. Additionally, the results highlighted that probable depression and satisfaction with life are associated with sexual life but the etiological relation was not clarified, as SD could affect the emotional well-being and vice versa.
More and thorough research in a larger sample and probably with a control group is pivotal in the verification of our results. Therefore, future research is needed to provide a more detailed panel of factors possibly affecting the sexual function of women after SCI (medications, smoking, alcohol use, etc.), and also to utilize information provided by the rehabilitation team during the inpatient and outpatient program. Further data will aid in the establishment of a better rehabilitation plan and subsequent improvement in the quality of care this group of patients receive.
Conclusions
The present study evaluated the rates of SD in a non-representative sample of female individuals with SCI that reside in Greece and estimated them at somewhat lower levels compared to similar studies from other countries. Moreover, it illustrated the correlation of SD parameters with several clinical and sociodemographic variables that deserve specific attention by clinicians when classifying women regarding SD risk. Precise monitoring for SD in women with SCI who suffer from severe body pain and depressive symptoms, in those presenting with low functional independence levels and limited social inclusion, and especially in the older ones, is strongly suggested.
Considering the predictors of SD in the female SCI population is of great importance; the knowledge of the specific characteristics of the women with SCI that are at high risk to present with SD can direct the adjustment of intervention guidelines and health care practices for this population. Our findings could also guide further research on the efficiency of medical protocols for the prevention and management of SD in women with SCI. Furthermore, our results indicate that decreasing the rates of SD in the population of women with SCI might have favorable effects on satisfaction with life, quality of life, emotional well-being, social participation, and functional capacity, as all those five parameters were robustly associated with various domains of sexual health.
Data availability
The datasets generated during the present study are available from the corresponding author on reasonable request.
References
Kreuter M, Taft C, Siosteen A, Biering-Sorensen F. Women’s sexual functioning and sex life after spinal cord injury. Spinal Cord. 2011;49:154–60.
Anderson KD, Borosoff JF, Johnson RD, Stiens SA, Elliott SL. The impact of spinal cord injury on sexual function: concerns of the general population. Spinal Cord. 2007;45:328–37.
Ferreiro-Velasco ME, Barca-Buyo A, de la Barrera SS, Montoto-Marqués A, Vázquez XM, Rodríguez-Sotillo A. Sexual issues in a sample of women with spinal cord injury. Spinal Cord. 2005;43:51–5.
Harrison J, Glass CA, Owens RG, Soni BM. Factors associated with sexual functioning in women following spinal cord injury. Paraplegia. 1995;33:687–92.
Forsythe E, Horsewell JE. Sexual rehabilitation of women with a spinal cord injury. Spinal Cord. 2006;44:234–41.
Sipski ML, Alexander CJ. Sexual activities, response and satisfaction in women pre- and post spinal cord injury. Arch Phys Med Rehabil. 1993;74:1025–9.
Kreuter M, Siosteen A, Biering-Sorensen F. Sexuality and sexual life in women with spinal cord injury: a controlled study. J Rehabil Med. 2008;40:61–9.
Roop S, Sharma SC. Sexuality and women with spinal cord injury. Sex Disabil. 2005;23:21–33.
Lombardi G, Del Popolo G, Mencarini M, Celso M. Sexual rehabilitation in women with spinal cord injury: a critical review of literature. Spinal Cord. 2010;48:1–8.
Anderson KD, Borisoff JF, Johnson RD, Stiens SA, Elliott SL. Spinal cord injury influences psychogenic as well as physical components of female sexual ability. Spinal Cord. 2007;45:349–59.
Reitz A, Tobe V, Knapp PA, Schurch B. Impact of spinal cord injury on sexual health and quality of life. Int J Impot Res. 2004;16:167–74.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves D, Jha A, et al. International standards for neurological classification of spinal cord injury (Revised 2011). J Spinal Cord Med. 2011;34:535–46.
Bryce TN, Budh CN, Cardenas DD, Dijkers M, Felix ER, Finnerup NB, et al. Pain after spinal cord injury: an evidence-based review for clinical practice and research. Report of the National Institute on Disability and Rehabilitation Research Spinal Cord Injury Measures Meeting. J Spinal Cord Med. 2007;30:421–40.
Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208.
Meston CM. Validation of the Female Sexual Function Index (FSFI) in women with female orgasmic disorder and in women with hypoactive sexual desire disorder. J Sex Marital Ther. 2003;29:39–46.
Wiegel M, Meston C, Rosen R. The Female Sexual Function Index (FSFI): cross-validation and development of clinical cutoff scores. J Sex Marital Ther. 2005;31:1–20.
Alexander MS, Brackett NL, Bodner D, Elliott S, Jackson A, Sonksen J, et al. Measurement of sexual functioning after spinal cord injury: preferred instruments. J Spinal Cord Med. 2009;32:226–36.
Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49:71–5.
The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;28:551–8.
Itzkovich M, Gelernter I, Biering-Sorensen F, Weeks C, Laramee MT, Craven BC, et al. The Spinal Cord Independence Measure (SCIM) version III: reliability and validity in a multi-center international study. Disabil Rehabil. 2007;29:1926–33.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Whiteneck GG, Charlifue SW, Gerhart KA, Overholser JD, Richardson GN. Quantifying handicap: a new measure of long-term rehabilitation outcomes. Arch Phys Med Rehabil. 1992;73:519–26.
Hajiaghababaei M, Javidan AN, Saberi H, Khoei EM, Khaifa DA, Koenig HG, et al. Female sexual dysfunction in patients with spinal cord injury. Spinal Cord. 2014;52:646–9.
Moreno-Lozano M, Durán-Ortíz S, Pérez-Zavala R, Quinzaños-Fresnedo J. Sociodemographic factors associated with sexual dysfunction in Mexican women with spinal cord injury. Spinal Cord. 2016;54:746–9.
Otero-Villaverde S, Ferreiro-Velasco M, Montoto-Marqués A, Salvador de la Barrera S, Arias-Pardo AI, Rodriguez-Sotillo A. Sexual satisfaction in women with spinal cord injuries. Spinal Cord. 2015;53:557–60.
Biering-Sørensen I, Hansen RB, Biering-Sørensen F. Sexual function in a traumatic spinal cord injured population 10-45 years after injury. J Rehabil Med. 2012;44:926–31.
Sramkova T, Skrivanova K, Dolan I, Zamecnik L, Sramkova K, Kriz J, et al. Women’s sex life after spinal cord injury. Sex Med. 2017;5:255–9.
Tzanos IA, Mavrogenis A, Gioti K, Papagelopoulos P, Panagiotopoulos E. Depressive mood in individuals with spinal cord injury (SCI) living in Greece. Spinal Cord. 2018;56:883–9.
Reitz A, Tobe V, Knapp PA, Schurch B. Impact of spinal cord injury on sexual health and quality of life. Int J Impot Res. 2004;16:167–74.
Merghati-Khoei E, Emami-Razavi SH, Bakhtiyari M, Lamyian M, Hajmirzaei S, Ton-Tab Haghighi S, et al. Spinal cord injury and women’s sexual life: case–control study. Spinal Cord. 2017;55:269–73.
Jackson AB, Wadley V. A multicenter study of women s self-reported reproductive health after spinal cord injury. Arch Phys Med Rehabil. 1999;80:1420–8.
Acknowledgements
We would like to give thanks to all individuals that consisted of the sample of the current study and also the Greek rehabilitation institutes that provided us availability to their medical data.
Author information
Authors and Affiliations
Contributions
IAT was the principal investigator, designed the study, collected the data, and was responsible for the methods, results, and conclusion sections, as well as contributing to the introduction and discussion. MT performed the data analysis and contributed to the methods and results sections. MN was responsible for the introduction and discussion sections, as well as contributing to the methods. CK co-designed the study protocol, contributed to data collection, and participated in the revision of the final version of the manuscript. All authors have read and approved the submitted final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
The ethics committee of the Medical School of the National and Kapodistrian University of Athens approved the present study. We certify that all participants received consent brochures that conformed with the Helsinki declaration principles and the Greek Medical ethics law (Hellenic State Law 3418/2005).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tzanos, IA., Tzitzika, M., Nianiarou, M. et al. Sexual dysfunction in women with spinal cord injury living in Greece. Spinal Cord Ser Cases 7, 41 (2021). https://doi.org/10.1038/s41394-021-00404-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-021-00404-7
This article is cited by
-
A Scoping Review of Literature on Sexual Health and Wellness in Women with Spinal Cord Injury
Sexuality and Disability (2024)
-
Relationship between hyperuricemia with deposition and sexual dysfunction in males and females
Journal of Endocrinological Investigation (2022)
