
Abstract
Study design
Descriptive.
Objective
The present aim was to define accelerometer cut-point values for wrist-worn accelerometers to identify absolute- and relative-intensity physical activity (PA) levels in people with motor-complete paraplegics (PP) and tetraplegics (TP).
Settings
Rehabilitation facility in Sweden.
Methods
The participants were 26 (19 men, 7 women) with C5–C8, AIS A and B (TP) and 37 (27 men, 10 women) with T7–T12 (PP), AIS A and B. Wrist-worn accelerometer recordings (Actigraph GT3X+) were taken during seven standardized activities. Oxygen consumption was measured, as well as at-rest and peak effort, with indirect calorimetry. Accelerometer cut-points for absolute and relative intensities were defined using ROC-curve analyses.
Results
The ROC-curve analyses for accelerometer cut-points revealed good-to-excellent accuracy (AUC >0.8), defining cut-points for absolute intensity (2, 3, 4, 5, 6, 7 METs for PP and 2 to 6 METs for TP) and relative intensity (30, 40, 50, 60, 70, and 80% for PP and 40–80% for TP). The cut-points for moderate-to-vigorous physical activity was defined as ≥9515 vector magnitude counts per minute (VMC) for PP and ≥4887 VMC/min for TP.
Conclusion
This study presents cut-points for wrist-worn accelerometers in both PP and TP, which could be used in clinical practice to describe physical activity patterns and time spent at different intensity levels.
Similar content being viewed by others


Introduction
Regular physical activity (PA) and the avoidance of prolonged daily sitting are important indicators for cardiovascular health, and affect health and function independently in the general population [1]. Persons with a spinal cord injury (SCI) and especially motor-complete paraplegia (PP) and motor-complete tetraplegia (TP), have lower PA levels and more sedentary than the general population [2, 3]. This may contribute to an increased incidence of cardiovascular disease (CVD) in the SCI population [4, 5]. Persons that are active at moderate-to-vigorous intensity PA (MVPA) for 150 to 300 min per week decrease the risk of CVD, in the general population [6]. The MVPA recommendation also has other health benefits such as maintaining healthy body weight and increasing physical function [6]. No similar robust, evidence-based recommendations are available for the SCI population, and proposed SCI guidelines have not yet been clinically established [7, 8].
Different methods are used to support and motivate persons to be more physically active. One of the most common methods, in the general population, to objectively measure PA intensity pattern is to use lightweight movement sensors, termed accelerometers [9] to record the acceleration of the wearer’s movement. The accelerometer provides a subsequent objective record of the absolute intensity, frequency and duration of the activity, summarized in ‘counts’ units.
In the general population, specific cut-points to describe intensity levels are available. For example, MVPA intensity is often described as mean counts per minute equal to three metabolic equivalents (METs). This describes intensity in absolute terms as multiples of resting energy expenditure (REE), where REE = 1 kcal kg h−1 [6, 10,11,12,13]. Nonetheless research to develop SCI-adapted cut-points is scarce and the results are equivocal [14, 15]. Using values from the general population to describe intensity levels is not feasible, since REE is lower (2.5–3.1 ml O2·kg−1·min−1) in the SCI population, with large intra-individual variance [16,17,18,19].
However, PA intensity may also be described in relative terms as intensity in relation to individual maximal aerobic capacity, as % of maximal oxygen uptake (VO2max or VO2peak). Relative intensity is recommended for populations where VO2peak is under 10 METs (35 ml O2·kg−1·min−1) [10]. The SCI population, especially individuals with TP, is one such specific population with lower physical function (VO2peak 5–10 MET) [10] due to autonomic response to PA.
Defining and developing SCI-specific cut-points, preferably separate cut-offs for PP and TP, for different intensity levels is essential to be able to objectively evaluate PA in free-living in research and to promote PA in clinical practice.
Hence, the present study aimed at defining accelerometer cut-points values for PP and TP with wrist-worn Actigraph GT3X+ for absolute and relative intensities, based on indirect calorimetry at resting, during activities and peak effort. Secondly, the study sought to propose accelerometer based cut-points for light, moderate and vigorous intensity levels for persons with PP and TP.
Methods
The present study included a convenience population-based sample with 63 men and women with SCI. Thirty-seven (27 men, 10 women) had a motor-compete PP and 26 (19 men, 7 women) had a motor-complete TP. Inclusion criteria were SCI injury level C5–C8 (TP) and T7–T12 (PP); AIS A and B motor-complete, ≥1 year post-injury, age ≥18 years, with minimal spasticity (Baclofen treated), as reported on the spasm frequency scale (Penn) [20]. Exclusion criteria were known coronary artery disease, angina pectoris and chronic congestive heart failure, chronic obstructive pulmonary disease, hormone replacement therapy, or shoulder pain. Recruitment was through advertisements on SCI-specific websites and by word-of-mouth.
Assessment of VO2 during rest
REE was assessed in a laboratory (thermoneutral environment) with indirect calorimetry (The Oxycon Pro, Hoechberg Germany) in the morning after fasting overnight (8 h) [21]. All participants were instructed to avoid any vigorous activity 12 h before the test and to empty the bladder before the test began. The participants were placed in supine position and inspired/expired gases were measured using a ventilated hood for 30 min The lowest steady VO2 recorded for at least 10 min was used to calculate REE. Prior to testing, the metabolic equipment was calibrated with built-in procedures and verified with reference gases.
Assessment of VO2 during the standardized activities
This study is part of a larger project that includes data from oxygen consumption during 14 standardized activities [18, 19]. For the present study only six activities were included based on the way the activity is performed. Thus weight training, arm crank and ski-ergometer were excluded since the accelerometer cannot detect individual resistance (weight kg or Watt) for these activities. The activities included were, watching TV, computer work, wheeling indoors (standardized track on wooden floor), setting table (standardized track), wheeling outdoors (standardized track on asphalt) Borg rating of perceived exertion (RPE) 10–11, wheeling outdoors (standardized track asphalt) Borg RPE 13–14 [18, 19]. These activities capture intensity levels from sedentary to vigorous. In brief, each activity was performed for 6–7 min to be able to reach steady state. Heart rate (beats per minute) and speed (kilometers per hour) were measured together with oxygen consumption. Oxygen consumption was measured with indirect calorimetry (The Oxycon Mobile, Hoechberg Germany) and the systems were calibrated and verified with reference gases and room air before the start of each test in a new room and when changin from one person to another. The steady-state values for the last 3 min VO2 in L·min−1 were used to calculate % of VO2peak and MET- values that were used in the ROC-analysis. The procedures are more thoroughly described in previous articles [18, 19]. Bodyweight was measured to the nearest 0.1 kg and height was self-reported and HR was measured with chest-strap (Polar) connected to the Oxycon Mobile and time spent in moderate activity with validated questioner [22].
Assessment of VO2 during peak effort
The arm-ergometer (Ergomedic 891E Monark, Sweden) was placed on a height-adjusted table and the participant was seated in their own wheelchair. Individuals with poor hand function brought their own gloves and all participants were asked whether they wanted to be strapped to the wheelchair to retain upper-body balance. The test began with warm-up (3 min), followed by a short break, before being incremented until exhaustion [23, 24]. An individually designed protocol to achieve peak VO2 according to international laboratory procedures and previous studies [24] included self-paced cadence starting between 70 and 90 revolutions per minute (rpm) and ending around 100 to 120 rpm [25]. The resistance was chosen depending on level of injury and exercise status based on the test result from arm-ergometer during the same day. The resistance was subsequently increased (each minute) by 0.25 kg for TP subjects with low (10 W or 15 W) resistance during arm ergometer work and 0.5 kg for those with high (20 W or 25 W). For PP participants the resistance was increased by 0.5 kg for those with 36 W resistance during arm ergometer exercise and 0.75 kg for those with 42 W. The last 2–3 min of the test were individually managed according to the participant’s state of exhaustion as evaluated from visual/auditory contact (Borg RPE). The anticipated time to exhaustion was between 6 and 12 min. VO2 and HR during the test was measured continuously with a mobile open-circuit system (Jaeger Oxycon Mobile system (Hoechberg, Germany). All data were analyzed as 10-second averages and VO2peak was determined from the highest mean value during 30 seconds. Criteria for acceptance (all was needed)of the VO2peak measurement were: “levelling off” of VO2 despite increased resistance, RPE above 16, test time more than 6 min, supported by a respiratory quotient (RQ/RER) greater than 1.1. None of the participants wore leg wraps and/or abdominal binders.
Accelerometer measurements
The participants were fitted with the GT3X+ activity monitor (ActiGraph, Pensacola, FL) at the wrist of the dominant hand. A small (3.8 × 3.7 × 1.8 cm), lightweight (27 g) electronic device, the activity monitor recorded the acceleration of the participant´s movement in three axis/dimensions, providing an objective record of the intensity, frequency and duration of the activity performed during wear time, summarized in “counts” units. The activity monitor were worn during all activities and correlated to oxygen consumption (absolute and relative) and HR. The accelerometer was initialized and data downloaded and processed using the ActiLife v.6.10.1 software. Raw data sampling frequency was set to 30 Hz, and extracted as 60-s tri-axial epochs using vector magnitude as accelerometer output.
Data analysis
All VO2 data were analyzed using JLAB, Carefusion (Germany 234 GmbH, Hoechberg, Germany). The last 10 min of the REE data were analyzed and represent mean values. All data were tested for normal distribution and are presented as mean and ±SD analyzed with parametric tests. Non-normally-disturbed data are presented as interquartile range (IQR). REE was subtracted from total energy expenditure (TEE) to generate AEE for each activity, TEE-REE = AEE (kcal·min−1). The vector magnitude counts (VMC) from the GT3X+ were downloaded as 15-s averages for identification and later summed into 60-s averages. Intensity levels are expressed as percent (%) of peak oxygen consumption (VO2peak) or metabolic equivalents (SCI METs). SCI METs were calculated from individual REE since there was a large intra individual difference for REE in ml O2·kg−1·min−1. All values were stratified between 30, 40, 50, 60, 70, and 80% of VO2peak and 2, 3, 4, 5, 6, 7, and 8 SCI MET. Each intensity level was dichotomized as =1 if above the % of VO2peak or individual SCI MET (ex. ≥40.0% VO2peak or ≥3.0 SCI MET) or =0 if below that value (ex. <40% VO2peak or <3 SCI MET).
Spearman’s RHO correlation coefficients (r), were used to assess the association between the relative (%VO2peak), absolute individual MET and accelerometer GT3X+ VMC during all standardized activities. Spearman’s was categorized as strong 0.6–0.79 or very strong 0.8–1.0 [26]. Standardized instructions and calibration methods were used to reduce systematic errors. Accelerometer cut-points were identified with receiver-operating- characteristic (ROC)-curve analysis, where an area under the curve (AUC) of 0.5 indicates that the test is no better than chance, 0.6–0.7 poor, 0.7–0.8 fair, 0.8–0.9 good, 0.9–1 excellent while1.0 indicates a perfect test [27]. The optimal cut-points point is that closest to the upper left corner of the ROC-curve figure, which represents 100% sensitivity and 100% specificity. To identify the most appropriate sensitivity and specificity value as the cut-points, we used the distance to the upper left corner, Youden’s index [28]. When these distances were insufficient to separate two values, we used accuracy and diagnostic odds ratios (calculated from positive likelihood divided by negative likelihood) to choose the most appropriate cut-points. SPSS version 25.0 was used for the statistical analyses. The proposed accelerometer cut-points for light, moderate and vigorous intensity were derived from relative intensity [10, 11]. The decision was based on different criteria firstly, the recommendation to use relative intensity when the MET-value for VO2peak is below 10 MET. For example, VO2peak below 10 MET equals’ moderate intensity between 46 and 63% of VO2peak and VO2peak below 5 MET equals moderate intensity between 52 and 68% of VO2peak [10, 11]. Secondly, since this sample was widespread in age, BMI and PA level (no elite athletes) the abovementioned recommendation was best available option.
Results
There was a significant difference for body mass between PP and TP, mean 72.9kg vs. 65.3 kg, and consequently BMI, mean 23.1 vs 20.5 (Table 1). Resting oxygen consumption LO2·min−1 for PP was 0.18 LO2 ·min−1 and 0.16 LO2·min−1 for TP (p = 0.13). The difference for resting oxygen consumption related to bodyweight (ml O2·kg−1·min−1) was 2.48 ml O2·kg−1·min−1 for PP and 2.56 ml O2·kg−1·min−1 for TP (p = 0.48). This gives a mean value for the whole group of 2.51 ml O2·kg−1·min−1. There was a large and significant difference for VO2peak 18.5 ml O2·kg−1·min−1for PP vs. 11.1 ml O2·kg−1·min−1 For TP, which equaled 8.0 (IQR 6.7–9.0) SCI METs for PP and, 4.7 (IQR 3.5–5.5) for TP (Table 1), calculated from individual REE. Moreover, there were no significant differences between men and women in VMC within each activity p > 0.07.
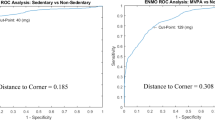
Relative intensities showed a “very strong and strong” (r = 0.9 PP and r = 0.77 TP) correlation to accelerometer VMC and “very strong” correlation for MET values r = 0.83 for PP and 0. 0.81 for TP (Fig. 1). The ROC analysis for accelerometer cut-points revealed excellent accuracy (AUC > 0.9) for relative intensities for PP and good to excellent accuracy (AUC > 0.8 and AUC > 0.9) for TP, see Table 2. The accuracy for absolute intensities was good-to-excellent for PP, with equal result for TP except for 6 SCI METs (AUC = 0.73). The ROC-analysis was done on group level as well as gender level for VMC cut-points. The result showed a median difference of 1.52 % (IRQ 5.47%) between the group-specific and male/female specific VMC cut-point and with better balance between false positive/negative rate for the group specific cut-points.

Correlation matrix between relative/absolute intensity and vector magnitude counts. RPE Borg ratings of perceived exertion, MET metabolic equivalent
Proposed accelerometer cut-points for light, moderate and vigorous intensity levels
As already stated, the VO2peak showed a MET value below 10 for PP and below 5 for TP, so the proposed cut-points were based on relative intensity, as recommended [6, 10]. The result for the recommended cut-points at light intensity (6997 VMC) shows a small improvement in accuracy where one measure point more is correct categorized by using the gender specific cut-points for persons with PP. The result for moderate (9515 VMC) and vigorous intensity (13239 VMC) for PP shows no difference in the number of correct categorize between men and women, or the rate of false positive/negative (Table 3). The result for the recommended cut-points for persons with TP at light (3462 VMC) intensity and moderate (4887 VMC) and, vigorous intensity (9279 VMC) show no difference between accuracy and false/negative rate by using the gender specific cut-points (Table 3). The result for the recommended cut-points for light and moderate intensity (Table 3) shows that 88% are correctly categorized and 6% for light intensity and 8% false positive (PP). Vigorous activity showed an accuracy of 96% and 1.4% FP. The result for persons with TP showed that 91% were correctly categorized at light intensity and 6% were FP. While 84% (moderate) and 86% (vigorous) were correct categorized and 3% vs. 7% were FP for persons with TP. We also describe the “sedentary” result, which was based on that there was only one person (TP) that had a VMC over 2000 within both groups during TV-watching. In addition, the low-light intensity is based on the VMC counts that were between sedentary and light intensity. Further, the questioner about time spent in moderate activity level showed that 48% of the participants with motor-complete PP and 68% of PP were active in moderate level for at least 45 min during a week.
Discussion
The main result is the SCI-specific wrist-worn accelerometer cut-points derived for both relative (% of VO2peak) and absolute (SCI METs), analyzed with high accuracy using ROC-curve analysis. Cut-point value for moderate intensity activity level (defined as 46% of VO2peak) was ≥9515 VMC with a span up to 13238 VMC which is the cut point for vigorous intensity level. The cut-point for moderate intensity (52% of VO2peak) was ≥4887 VMC with a span up to 9278 VMC, which is the cut point for vigorous intensity level for persons with TP.
Accelerometer cut-points for absolute and relative intensities
This study is, to our knowledge the first to define cut-points values for intensity of physical activities with ROC-analysis for both relative (% of VO2peak) and absolute (SCI METs) intensity levels in motor-complete SCI.
Two previous studies have defined SCI-specific cut-points for moderate-to vigorous physical activity (MVPA) using absolute intensity [14, 15]. The first included both PP and TP, and described moderate activity as 3 SCI MET = 8.1 ml O2·kg−1·min−1 with a cut-points value of 11652 VMC for both PP and TP [14]. The second study included a mix of neurological disorders, used the same 3 MET value as that in the general population = 10.5 ml O2·kg−1·min−1. This resulted in a cut-points value of 3644 VMC [15]. Our result combined with the abovementioned studies shows a large discrepancy for MVPA accelerometer cut-points. This might be partly because the two earlier studies used generalized group cut-points including both PP and TP [13] or a mix of neurological disorders [15]. Another associating factor for both those studies is that they based their cut-points value on multilevel linear regression analysis, while our study uses ROC-curve analysis. This reduces the variation across individual’s activity counts within the same activity [29]. ROC-curve analysis provides a pure index of accuracy by examining the test’s ability to discriminate between two conditions. This is done by testing every predictor variable and cut-point to identify the optimal predictor value and its associated cut-point [27]. This is described by the AUC, which gives the overall accuracy of the predictor and the probability that the cut-point correctly categorizes the specific level of intensity [29]. The result is a lower rate of misclassification compared to that in regression models [29]. The result for the AUC (PP) in this study suggests that the accuracy of the cut-points values for relative intensities is between excellent (AUC > 0.9) and good-to-excellent (AUC > 0.8). The high accuracy together with high sensitivity (true positive) and specificity (true negative) for each level of intensity is a basis for further validation studies. One factor that explains the high accuracy for the wrist-worn accelerometer in our group of PP and TP is that all activity energy expenditure is generated from the arms. Moreover, the decision to use the dominant wrist was made before any validation studies were published. The article by Garcia-Masso et al. [30], shows that slow and fast propulsion has lower error for dominant wrist compared to non-dominant wrist. So, using the dominant wrist for discriminate between different intensity levels seem valid.
A factor for the large variation between the present study and the two previously mentioned is related to the use of absolute vs. relative intensity to define cut-points. In the present study, VO2peak, at group level, was 18.5 (PP) and 11.1 (TP), which is comparable to previous studies that’s not based on elite athletes [31,32,33,34]. The result for the VO2peak as SCI MET based on the individual REE was 8.0 (IQR 6.7–9.0) for PP and 4.7 (IQR 3.5–5.5) for TP. Under these prerequisites it is recommended to use relative intensities to discriminate between different intensity levels [6]. For example, the recommendation for moderate intensity below 10 MET is equal to a relative intensity between 46 and 63% of VO2peak and below 5 MET it is equal to 52–68% of VO2peak [6, 10]. The explanation of this relates to the narrow span between resting oxygen consumption and VO2peak, especially for TP (4.7 SCI MET). Hence, one may argue that the correlation is higher between SCI MET values and VMC for TP (Fig. 1). However, the increase in oxygen consumption between SCI MET is large, and results in close-to-peak oxygen consumption already at 3 MET (Table 2). However, there is an on-going debate regarding the use of SCI MET verses the use of Ainsworth MET 3.5 ml O2·kg−1·min−1. Byrne et al. [35] described the MET-value as “one size does not fit all”, which seem plausible and could explain the different results for MET-values between SCI studies. In this study we chose describe MET-values from the individual REE since there was a large intra-individual difference. In this study we define accelerometer cut-points for sedentary, low light intensity, light, moderate and vigorous intensity levels (Table 3). Our light, moderate and vigorous intensity levels are based purely on the recommendation for intensity levels [10]. Moreover, the cut-points for sedentary and low light intensity were derived from the highest VMC during TV-watching in both groups and the low light intensity was the VMCs between sedentary and light intensity cut-points derived from the recommendation mentioned above [10].
Our proposed cut-points are not linked to any health parameters. However, previous research in the SCI population has shown that relative intensities between 50 and 70% of VO2peak seem to be linked to health benefits such as better body composition and lower CVD risk in SCI [36]. Other studies report that the more time spent in non-exercise or leisure-time PA was related to lower LDL, BMI and fat mass [37,38,39]. However, the recommendations for duration and frequency are not conclusive; studies point towards 30–60 min per/day of moderate intensity activity [38, 40]. Hence, since we provide a large variation of cut-points for different intensity levels, future validation research could base MVPA on any suitable absolute or relative intensity accelerometer cut-points.
Strengths and limitation
One limiting factor was a large intra-individual difference for REE (ml O2·kg−1·min−1), which affects the result for energy turnovers with a fixed value. The results may best apply to none-elite athlete people within the same range of BMI, age, levels of injury and injury severity. Another limitation is that the correlations may be inflated because of the nesting of observations within participants. The decision of using the dominant wrist was taken before the article by Garcia-Masso et al. however the conclusion from that article were that it is possible to collect data from either wrist [30]. Hence, the non-dominant wrist seems to be beneficial in some situations and vice versa [15, 30]. Strengths compared to previous literature include the sample size, the heterogeneous sample of individuals and the inclusion of seventeen women, which enables important and clinically relevant gender comparisons. In addition, the extensive protocol for the activities was collected under real-life conditions, for ecological validity, together with both REE and VO2peak. Another strength is the use of ROC-curve analysis instead of logistic or multilevel linear regression analysis when identifying the accelerometer cut-points for different intensity levels; and that the cut-points were assessed separately for motor-complete PP and motor-complete TP and men and women.
Conclusion
This study defines, with high accuracy, ROC-curve based, accelerometer cut-points for both PP and TP. The cut-points may be used in both research and clinical rehabilitation settings to describe activity patterns and time spent at different PA intensity levels. The cut-points for moderate-to-vigorous physical activity were defined as ≥9515 for PP and ≥4887 VMC/min for TP. The result is valuable tool to describe time spent in different intensity levels; both for persons with SCI in rehabilitation or free-living and in research regarding CVD. However, future studies are needed to confirm the cut-points and define cut-points for other injury levels.
Data archiving
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
04 December 2019
A Correction to this paper has been published: https://doi.org/10.1038/s41393-019-0397-7
References
Ekblom-Bak E, Ekblom B, Hellenius ML. Less sitting as important as increased physical activity. Lakartidningen. 2010;107:587–8.
Noreau L, Shephard RJ, Simard C, Pare G, Pomerleau P. Relationship of impairment and functional ability to habitual activity and fitness following spinal cord injury. Int J Rehabil Res Int Z fur Rehabil Rev Int de Rech de Readapt. 1993;16:265–75.
Buchholz AC, McGillivray CF, Pencharz PB. Physical activity levels are low in free-living adults with chronic paraplegia. Obes Res. 2003;11:563–70.
Myers J, Lee M, Kiratli J. Cardiovascular disease in spinal cord injury: an overview of prevalence, risk, evaluation, and management. Am J Phys Med Rehabi Feb. 2007;86:142–52.
Lavis TD, Scelza WM, Bockenek WL. Cardiovascular health and fitness in persons with spinal cord injury. Phys Med Rehabil Clin North Am. 2007;18:317–31.
2018 Physical Activity Guidelines Advisory Committee Physical Activity Guidelines Advisory Committee Report. Vol. 2018 (https://health.gov/paguidelines/report/pdf/CommitteeReport.pdf 2018).
Ginis KAM, van der Scheer JW, Latimer-Cheung AE, Barrow A, Bourne C, Carruthers P, et al. Correction: evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and a new guideline. Spinal Cord. 2018;56:1114.
Tweedy SM, Beckman EM, Connick MJ, Geraghty TJ, Theisen D, Perret C, et al. Correspondence re "Evidence-based scientific exercise guidelines for adults with spinal cord injury: an update and new guideline". Spinal Cord. 2018;56:406–8.
Liu S, Gao RX, Freedson PS. Computational methods for estimating energy expenditure in human physical activities. Med Sci sports Exerc. 2012;44:2138–46.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci sports Exerc. 2011;43:1334–59.
FYSS 2017 : fysisk aktivitet i sjukdomsprevention och sjukdomsbehandling, (Läkartidningen förlag AB, Stockholm, 2016).
Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr., Montoye HJ, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci sports Exerc. 1993;25:71–80.
Conger SA, Bassett DR. A compendium of energy costs of physical activities for individuals who use manual wheelchairs. Adapt Phys Act Q. 2011;28:310–25.
McCracken LA, Ma JK, Voss C, Chan FHN, Martin Ginis KA, West CR. Wrist accelerometry for physical activity measurement in individuals with spinal cord injury - a need for individually calibrated cut-points. Arch Phys Med Rehabil. 2017;99:684–689.
Learmonth YC, Kinnett-Hopkins D, Rice IM, Dysterheft JL, Motl RW. Accelerometer output and its association with energy expenditure during manual wheelchair propulsion. Spinal cord. 2016;54:110–4.
Collins EG, Gater D, Kiratli J, Butler J, Hanson K, Langbein WE. Energy cost of physical activities in persons with spinal cord injury. Med Sci sports Exerc. 2010;42:691–700.
Lee MZ, Hedrick W, B Fernhall B. Determining metabolic equivalent values of physical activities for persons with paraplegia. Disabil Rehabil. 2010;32:336–43.
Holmlund T, Ekblom-Bak E, Franzen E, Hultling C, Wahman K. Energy expenditure after spinal cord injury in people with motor-complete tetraplegia or motor-complete paraplegia. Spinal Cord. 2017;56:274–283.
Holmlund T, Ekblom-Bak E, Franzen E, Hultling C, Wikmar LN, Wahman K. Energy expenditure in people with motor-complete paraplegia. Spinal Cord. 2017;55:774–781.
Penn RD. Intrathecal baclofen for severe spasticity. Ann N Y Acad Sci. 1988;153:157–66.
Haugen HA, Chan LN, Li F. Indirect calorimetry: a practical guide for clinicians. Nutrition Clin Practice. 2007;22:377–88.
Flank P, Fahlstrom M, Bostrom C, Lewis JE, Levi R, Wahman K. Self-reported physical activity and risk markers for cardiovascular disease after spinal cord injury. J Rehabil Med. 2014;46:886–90.
Leicht CA, Tolfrey K, Lenton JP, Bishop NC, Goosey-Tolfrey VL. The verification phase and reliability of physiological parameters in peak testing of elite wheelchair athletes. Eur J Appl Physiol. 2013;113:337–45.
Sperlich PF, Holmberg HC, Reed JL, Zinner C, Mester J, Sperlich B. Individual versus Standardized Running Protocols in the Determination of VO2max. J sports Sci Med. 2015;14:386–93.
Beltz NM, Gibson AL, Janot JM, Kravitz L, Mermier CM, Dalleck LC. Graded exercise testing protocols for the determination of VO2max: historical perspectives, progress, and future considerations. J Sports Med. 2016;2016:3968393.
Bland JM, Altman DG. Cronbach's alpha. Brit Med J. 1997;314:572–572.
Zweig MH, Campbell G. Receiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicine. Clin Chem. 1993;39:561–77.
Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3:32–5.
Jago R, Zakeri I, Baranowski T, Watson K. Decision boundaries and receiver operating characteristic curves: new methods for determining accelerometer cutpoints. J Sports Sci. 2007;25:937–44.
Garcia-Masso X, Serra-Ano P, Garcia-Raffi LM, Sanchez-Perez EA, Lopez-Pascual J, Gonzalez LM. Validation of the use of Actigraph GT3X accelerometers to estimate energy expenditure in full time manual wheelchair users with spinal cord injury. Spinal cord. 2013;51:898–903.
Haisma JA, van der Woude LHV, Stam HJ, Bergen MP, Sluis TAR, Bussmann JBJ. Physical capacity in wheelchair-dependent persons with a spinal cord injury: a critical review of the literature. Spinal Cord. 2006;44:642–52.
Kressler J, Jacobs K, Burns P, Betancourt L, Nash MS. Effects of circuit resistance training and P timely protein supplementation on exercise-induced fat oxidation in tetraplegic adults. Top Spinal Cord Inj Rehabil. 2014;20:113–22.
Lovell D, Shields D, Beck B, Cuneo R, McLellan C. The aerobic performance of trained and untrained handcyclists with spinal cord injury. Eur J Appl Physiol. 2012;112:3431–7.
Gauthier C, Arel J, Brosseau R, Hicks AL, Gagnon DH. Reliability and minimal detectable change of a new treadmill-based progressive workload incremental test to measure cardiorespiratory fitness in manual wheelchair users. J Spinal Cord Med. 2017;40:759–67.
Byrne NM, Hills AP, Hunter GR, Weinsier RL, Schutz Y. Metabolic equivalent: one size does not fit all. J Appl Physiol. 2005;99:1112–9.
van der Scheer JW, Martin Ginis KA, Ditor DS, Goosey-Tolfrey VL, Hicks AL, West CR, et al. Effects of exercise on fitness and health of adults with spinal cord injury: a systematic review. Neurology. 2017;89:736–45.
Hetz SP, Latimer AE, Buchholz AC, Martin Ginis KA. Increased participation in activities of daily living is associated with lower cholesterol levels in people with spinal cord injury. Arch Phys Med Rehabil. 2009;90:1755–9.
Buchholz AC, Martin Ginis KA, Bray SR, Craven BC, Hicks AL, Hayes KC, et al. Greater daily leisure time physical activity is associated with lower chronic disease risk in adults with spinal cord injury. Appl Physiol, Nutr, Metab = Physiol Appl, Nutr et Metab. 2009;34:640–7.
Jorgensen S, Svedevall S, Magnusson L, Martin Ginis KA, Lexell J. Associations between leisure time physical activity and cardiovascular risk factors among older adults with long-term spinal cord injury. Spinal Cord. 2019;57:427–433.
Ginis KA, Arbour-Nicitopoulos KP, Latimer AE, Buchholz AC, Bray SR, Craven BC, et al. Leisure time physical activity in a population-based sample of people with spinal cord injury part II: activity types, intensities, and durations. Arch Phys Med Rehabil. 2010;91:729–33.
Acknowledgements
We thank all the participants and Mikael Flockheart for all help with the data collection.
Author contributions
TH was responsible conducting the search, screening potentially eligible studies, extracting and analyzing data, interpreting results, creating ’Summary of findings’ tables, and writing the report. EEB was responsible for designing the assessment protocol, analyzing and interpreting results. She revised the manuscript for important intellectual content. EF contributed to the design, revised the manuscript for important intellectual content and interpreting results. CH contributed to acquire data and provided feedback on the report. KW was responsible for designing the assessment protocol, analyzing and interpreting results. She revised the manuscript for important intellectual content. All of the abovementioned authors approved the final version.
Funding
This study was supported by the Promobilia Foundation, the Märta and Gunnar V. Philipson Foundation, the Norrbacka-Eugenia Foundation, the Swedish Association for Survivors of Accident and Injury (RTP), the Spinalis Foundation and NEURO Sweden.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. Each participant provided written informed consent, and ethical approval was obtained from the Stockholm region ethics committee, registration number 2011/1989–31/1.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Holmlund, T., Ekblom-Bak, E., Franzén, E. et al. Defining accelerometer cut-points for different intensity levels in motor-complete spinal cord injury. Spinal Cord 58, 116–124 (2020). https://doi.org/10.1038/s41393-019-0308-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-019-0308-y
