
Abstract
Introduction
This study aims to determine if there is a difference in prostate cancer nomogram-adjusted risk of biochemical recurrence (BCR) and/or adverse pathology (AP) between African American (AAM) and Caucasian men (CM) undergoing radical prostatectomy (RP).
Methods
A retrospective review was performed of men undergoing RP in the Pennsylvania Urologic Regional Collaborative between 2015 and 2021. Cox proportional hazard regression models were used to compare the rate of BCR after RP, and logistic regression models were used to compare rates of AP after RP between CM and AAM, adjusting for the CAPRA, CAPRA-S, and MSKCC pre- and post-operative nomogram scores.
Results
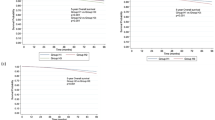
Rates of BCR and AP after RP were analyzed from 3190 and 5029 men meeting inclusion criteria, respectively. The 2-year BCR-free survival was lower in AAM (72.5%) compared to CM (79.0%), with a hazard ratio (HR) of 1.38 (95% CI 1.16–1.63, p < 0.001). The rate of BCR was significantly greater in AAM compared to CM after adjustment for MSKCC pre-op (HR 1.29; 95% CI 1.08–1.53; p = 0.004), and post-op nomograms (HR 1.26; 95% CI 1.05–1.49; p < 0.001). There was a trend toward higher BCR rates among AAM after adjustment for CAPRA (HR 1.13; 95% CI 0.95–1.35; p = 0.17) and CAPRA-S nomograms (HR 1.11; 95% 0.93–1.32; p = 0.25), which did not reach statistical significance. The rate of AP was significantly greater in AAM compared to CM after adjusting for CAPRA (OR 1.28; 95% CI 1.10–1.50; p = 0.001) and MSKCC nomograms (OR 1.23; 95% CI 1.06–1.43; p = 0.007).
Conclusion
This analysis of a large multicenter cohort provides further evidence that AAM may have higher rates of BCR and AP after RP than is predicted by CAPRA and MSKCC nomograms. Accordingly, AAM may benefit with closer post-operative surveillance and may be more likely to require salvage therapies.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


Data availability
The data that support the findings of this study are available on request from the Pennsylvania Urologic Regional Collaborative (PURC). The data are not publicly available due to institutional and patient privacy concerns.
References
Sanda MG, Cadeddu JA, Kirkby E, Chen RC, Crispino T, Fontanarosa J, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Part I: risk stratification, shared decision making, and care options. J Urol. 2018;199:683–90.
Gershman B, Maroni P, Tilburt JC, Volk RJ, Konety B, Bennett CL, et al. A national survey of radiation oncologists and urologists on prediction tools and nomograms for localized prostate cancer. World J Urol. 2019;37:2099–108.
Bauer JJ, Connelly RR, Seterhenn IA, Deausen J, Srivastava S, Mcleod DG, et al. Biostatistical modeling using traditional preoperative and pathological prognostic variables in the selection of men at high risk for disease recurrence after radical prostatectomy for prostate cancer. J Urol. 1998;159:929–33.
Moul JW, Connelly RR, Lubeck DP, Bauer JJ, Sun L, Flanders SC, et al. Predicting risk of prostate specific antigen recurrence after radical prostatectomy with the Center for Prostate Disease Research and Cancer of the Prostate Strategic Urologic Research Endeavor databases. J Urol. 2001;166:1322–7.
Schroeck FR, Sun L, Freedland SJ, Jayachandran J, Robertson CN, Moul JW. Race and prostate weight as independent predictors for biochemical recurrence after radical prostatectomy. Prostate Cancer Prostatic Dis. 2008;11:371–6.
Hamilton RJ, Aronson WJ, Presti JC Jr, Terris MK, Kane CJ, Amling CL, et al. Race, biochemical disease recurrence, and prostate–specific antigen doubling time after radical prostatectomy: results from the SEARCH database. Cancer. 2007;110:2202–9.
Nielsen ME, Han M, Mangold L, Humphreys E, Walsh PC, Partin AW, et al. Black race does not independently predict adverse outcome following radical retropubic prostatectomy at a tertiary referral center. J Urol. 2006;176:515–9.
Cooperberg MR, Pasta DJ, Elkin EP, Litwin MS, Latini DM, Du Chane J, et al. The University of California, San Francisco Cancer of the Prostate Risk Assessment score: a straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J Urol. 2005;173:1938–42.
Kattan MW, Eastham JA, Stapleton AM, Wheeler TM, Scardino PT. A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst. 1998;90:766–71.
Cooperberg MR, Hilton JF, Carroll PR. The CAPRA‐S score: a straightforward tool for improved prediction of outcomes after radical prostatectomy. Cancer. 2011;117:5039–46.
Kattan MW, Wheeler TM, Scardino PT. Postoperative nomogram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol. 1999;17:1499.
D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74.
Moreira DM, Presti JC, Aronson WJ, Terris MK, Kane CJ, Amling CL, et al. The effect of race on the discriminatory accuracy of models to predict biochemical recurrence after radical prostatectomy: results from the Shared Equal Access Regional Cancer Hospital and Duke Prostate Center databases. Prostate Cancer Prostatic Dis. 2010;13:87–93.
Bianco FJ Jr, Kattan MW, Scardino PT, Powell IJ, Pontes JE, Wood DP Jr. Radical prostatectomy nomograms in black American men: accuracy and applicability. J Urol. 2003;170:73–77.
Harrell FE. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. Vol. 608. New York: Springer; 2001.
Berg S, Tully KH, Sahraoui A, Tan WS, Krimphove MJ, Marchese M, et al. Inequity in selective referral to high-volume hospitals for genitourinary malignancies. Urol Oncol. 2020;38:582–9.
Park MY, Park KJ, Kim MH, Kim JK. Preoperative MRI-based estimation of risk for positive resection margin after radical prostatectomy in patients with prostate cancer: development and validation of a simple scoring system. Eur Radiol. 2021;31:4898–907.
Bernstein AN, Talwar R, Handorf E, Syed K, Danella J, Ginzburg S, et al. Assessment of prostate cancer treatment among black and white patients during the COVID-19 pandemic. JAMA Oncol. 2021;7:1467–73.
Author information
Authors and Affiliations
Contributions
Conceptualization: ME, ACR. Methodology, statistical analysis, and writing: ME. Data acquisition: KS. Review and editing: JD, SG, LB, JT, ET, EAS, BJ, JDR, TG, RU, ACR. Supervision: ACR.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Epstein, M., Syed, K., Danella, J. et al. Model risk scores may underestimate rate of biochemical recurrence in African American men with localized prostate cancer: a cohort analysis of over 3000 men. Prostate Cancer Prostatic Dis (2023). https://doi.org/10.1038/s41391-023-00727-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41391-023-00727-6
This article is cited by
-
Best of 2023 in Prostate Cancer and Prostatic Diseases
Prostate Cancer and Prostatic Diseases (2024)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}