
Abstract
Background
To describe pediatric Produce Prescription (PRx) interventions and their study designs, outcomes, and opportunities for future research.
Methods
A scoping review framework was used to describe PRx interventions published between January 2000 and September 2023. Articles from online databases were uploaded into Covidence. Data on study characteristics, outcomes of interest (health, food insecurity (FI), nutritional and culinary efficacy, and fruit and vegetable (F/V) consumption), and feasibility were extracted. The Mixed Methods Appraisal Tool (MMAT) was used for quality assessment.
Results
19 articles met inclusion criteria. Ten studies were quantitative, five were qualitative, and four used mixed-methods. Interventions included food vouchers (n = 14) or food box/pantries (n = 5). Four studies allowed food items in addition to F/Vs. Six studies measured changes in FI and five reported a statistically significant decrease. Seven studies measured changes in F/V consumption and five reported a statistically significant increase. One study reported a statistically significant reduction in child BMI z-score. Most studies reported high feasibility. Few studies used high-quality methods.
Conclusions
Pediatric PRx interventions show promising potential to reduce FI and improve diet quality and health-related outcomes. Future studies should utilize rigorous study designs and validated assessment tools to understand the impact of pediatric PRx on health.
Impact
-
This work offers a summary of programmatic outcomes including retention, redemption, incentives, nutrition education, study design and quality limitations to help inform future work.
-
We found positive impacts of pediatric produce prescriptions (PRx) on FI, F/V consumption, and nutritional knowledge and culinary skills.
-
More high-quality, rigorous studies are needed to understand the best delivery and design of PRx and their impact on child behavior and health outcomes.
-
This work provides support for the need for rigorous studies and the potential for PRx to play a role in multi-pronged strategies that address pediatric FI and diet-related disease.
Similar content being viewed by others

Introduction
A high-quality diet rich in fruits and vegetables (F/V) is associated with a decreased risk of chronic disease.1,2,3,4 However, few children and adults achieve the recommended daily F/V intake.5,6 Many factors limit an individual’s F/V intake,7,8 including socioeconomic status, food insecurity (FI), and a lack of access to adequate and nutritious food.9,10,11 In 2021, the prevalence of FI in the United States (U.S.) was 10.2%, but higher in households with children (12.5%) and in Black (19.8%) and Hispanic (16.2%) households.12 In adults, FI is associated with increased risk of chronic disease such as hypertension, diabetes, and stroke.13 While its association with risk of obesity, hypertension, and diabetes has been mixed in children,13 FI is associated with higher health care utilization and cost in children and families.14,15 It is also hypothesized that childhood FI could contribute to chronic diseases in adulthood, although there is not yet a clear understanding of this relationship. Given the disproportionate burden of FI in children and the rise in chronic conditions, such as diabetes, hypertension, and obesity in children over the past decade,16,17 FI and nutrition focused interventions are an important area for research.
Programs addressing FI and nutrition exist in school- and community-based settings.18,19,20 However, as FI and diet-related chronic disease are core medical concerns, interventions integrated within the healthcare setting are critical. According to the National Produce Prescription Coalition (NPPC) Produce Prescriptions (PRx) are “a medical treatment or preventative service for eligible patients due to diet-related health risks or conditions, food insecurity, or other documented challenges in access to nutritious foods, and are referred by a healthcare provider or health insurance plan. These prescriptions are fulfilled through food retailers and enable patients to access healthy produce with no added fats, sugars, or salt, at low or no cost to the patient. When appropriately dosed, PRx interventions are designed to improve healthcare outcomes, optimize medical spending, and increase patient engagement and satisfaction.”21 PRx interventions fall under the Food is Medicine framework (or Food as Medicine).22 These interventions work within the healthcare systems to offer patients with a diet-related chronic disease risk factor, such as prediabetes or obesity, and who may be at risk or experiencing food insecurity, greater access to produce. Low- or no-cost fresh, frozen, or canned produce and sometimes other food items such as non-perishable healthy staples (i.e. legumes/beans and whole grains) are offered through “incentives” such as redeemable vouchers or directly through provision of food by self-selection or pre-selection via pick-up or delivery. The goal of PRx is to help to prevent, manage, or treat diet-related disease.21,23,24 PRx studies have reported positive impacts on food security, health, and food intake among adults,25,26,27,28,29,30 as has been summarized in previously published reviews.23,31,32,33 The potential long-term health benefits of pediatric-focused PRx have not yet been well-studied given the relative novelty of this field.
To our knowledge, there is no published literature that summarizes pediatric-focused healthcare based PRx interventions. Furthermore, the rapid growth of the PRx interventions over the past 2–3 years renders a need for critical review of publications in the field. In particular, evidence for the impact of these initiatives on household FI and family dietary-related behaviors is lacking. This scoping review aims to describe the range of studies, interventions, and outcomes that exist in pediatric PRx interventions in healthcare settings and identify gaps and future directions for the field.
Methods
A protocol was developed based on the five-stepwise scoping review framework,34,35 which included defining the research question, creating search criteria, developing data gathering and analysis procedures, and reporting findings.
Relevant articles were assessed for eligibility using preset inclusion/exclusion criteria. Eligible articles described empirical studies, implementing a PRx in households with children <18 years old (yo); delivered its PRx within the U.S. healthcare system; reported child or adult FI, health, nutritional efficacy, or behavioral outcomes; and were published between January 2000 and September 2023. We also included PRx interventions that were primarily focused on F/V access but offered additional nutritious food items to provide a comprehensive review of interventions targeting F/V intake. Exclusion criteria were as follows: not in English; published before 2000; review articles; conducted outside of the U.S.; exclusively in adults; studies conducted outside of a healthcare system; studies without interventions or interventions that did not include a PRx component; and studies without measured outcomes.
Articles were obtained from online database searches on Pubmed, Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane, and Medline. A research librarian assisted in the creation of search terms, which included “food OR produce prescription OR vouchers OR programs OR pharmacy”, “pediatrics OR children OR adolescents”, “health outcomes”, and “food insecurity”. A full list of search terms can be found in Table 1. Articles were uploaded into Covidence (Veritas Health Innovation Ltd, Melbourne, Australia)36 for title and abstract screening, full-text review, and final determination of eligibility for data abstraction by two independent reviewers based on the pre-set inclusion/exclusion criteria. Disagreements between screeners were resolved with review by a third screener.
A data abstraction form and data reporting were guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.37 Data were abstracted to describe the study characteristics (study and intervention design, setting, inclusion/exclusion criteria. When reported by articles, the maximum incentive amounts offered per intervention were calculated using the reported amount, frequency, and duration of incentive offered), feasibility, and changes in health, FI status/severity, nutritional efficacy, and behaviors. Two independent reviewers extracted data for each article and an independent third reviewer reconciled discrepancies. A quality assessment of included studies was conducted using the Mixed Method Appraisal Tool (MMAT),38 which uses five criteria related to the appropriateness of the study design, representativeness of the population, adherence to the stated intervention, completeness of outcome data, and interpretation of the results to assess the methodological soundness of studies. Thus, each study received a rating on a scale of 0 to 5 corresponding to the quality of the study with respect to the stated primary outcome. Two independent reviewers evaluated each article and met regularly to come to a consensus on the quality rating for each study.
Results
Article screening
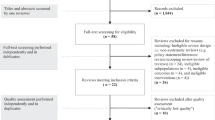
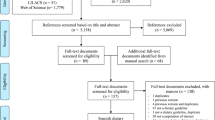
1980 articles underwent title and abstract screening of which 77 underwent full-text screening and 19 articles met eligibility criteria (Fig. 1), Of these 19 articles, four described results from one intervention.39,40,41,42 All 19 studies were published after 2014; the majority (n = 11) were published between 2020–2023.39,40,43,44,45,46,47,48,49,50,51

Figure 1 shows the flow from article identification to selection. The original database search yielded 2711 records. After duplicates were removed, there were 1980 unique citations. After screening by title and abstract, there were 77 eligible, full-text articles. Upon assessing eligibility, it was found that 59 full-text articles were not eligible: 15 did not include children, 11 had no affiliation with a healthcare institution or provider, 11 did not include a food or produce prescription, 11 were review articles, 4 did not have a full-text available, 3 were published outside the U.S., 2 were published prior to 2000, and 1 did not have measurement outcomes. A total of 19 studies were included for scoping review.
Study design, setting, and populations
See a summary of intervention delivery types in Fig. 2 and results in Table 2. Ten studies were quantitative,39,40,41,45,46,48,49,51,52,53 five were qualitative,42,44,50,54,55 and four used mixed methods.43,47,56,57 Of the 14 quantitative or mixed methods studies, 13 were longitudinal and one was cross-sectional.40 There were no were randomized control trials (RCTs), two studies utilized control groups to compare outcomes,40,52 and the remainder were pre-post comparisons. One study reported the aggregated outcomes from data collected across 9 program sites, but only three sites enrolled children, so we will only report on the pediatric programs and outcomes reported in this multi-site study.51 Fourteen took place in primary care settings, two in a school-based health system,43,54 two in subspecialty clinics,50,55 and one did not specify.51 In all but two cases,50,54 patients and families were directly referred to the program by a healthcare provider. In most cases this was a primary care provider (Pediatrician, Nurse Practitioner) and in some cases it was ancillary clinic staff or allied health professionals (Community Health Worker or Dietitian/Nutritionist). Eleven studies were conducted within urban settings,39,40,41,42,46,47,48,50,52,54,56 three within rural settings,43,44,45 and five did not specify.49,51,53,55,57 The number of participants ranged from four55 to 1,81751 with a geometric mean of 79. Twelve studies had health risk factors, FI status/severity, or income related inclusion criteria.43,44,45,46,47,48,49,51,53,55,56,57 Seven did not have health- or income-specific inclusion criteria.39,40,41,42,50,52,54 All studies included both adult and child participants. Children’s age ranges were <1 yo (n = 1),52 <6 yo (n = 3),45,47,48 2–18 yo (n = 7),39,41,44,46,51,53,57 0–15 yo (n = 1),54 and any age (0–18 yo) (n = 7).40,42,43,49,50,55,56

There were a total of 19 interventions evaluated, intervention models fell into two categories: voucher programs (n = 14) or box/pantry programs (n = 5). Thirteen voucher programs utilized farmers’ markets (FM) or retailers and one used an online produce market. Two voucher programs allowed redemption for other foods in addition to produce. Among box programs, two allowed self-selected produce and non-perishable items and three programs offered pre-selected F/Vs only. One provided delivery services and the rest were pick-up.
Incentive models
The intervention incentive models fell into two categories: voucher programs (n = 14),39,40,41,42,43,44,45,46,51,52,53,54,55,57 or box/pantry programs (n = 5).47,48,49,50,56 Thirteen voucher programs utilized farmers’ markets (FM) or retailers while one used an online produce market.43 All voucher programs allowed redemption for produce, though two programs allowed redemption for other food sold at FM locations, like meats, cheeses, baked goods,54 or culturally significant foods like blue cornmeal or dried steam corn.45 Among box programs, two allowed self-selected produce and non-perishable items48,56 and three programs offered pre-selected F/Vs only.47,49,50 One provided delivery services47 and the rest were pick-up only.
Distribution of incentives
There was wide variability in the amount, duration, and frequency of incentive distributions. Among voucher programs, the lowest distribution amount was a one-time voucher of $10 or $20.46 The highest incentive amount across all voucher interventions was $300 per month for 6–9 months, which would equal a theoretical maximum value of $2,700.51 The remaining voucher interventions were calculated to have a range of maximum incentives from a one-time distribution of $3054 to $900 over 6 months43,45 per household. Four interventions varied the voucher amount by family size43,45,51,53 and one varied voucher amount by FI status.46 Among box programs, three studies47,49,56 reported pounds of produce offered, which ranged from 8 to 30 pounds per distribution. One study described a “box” of produce per distribution50 while another study indicated the amount as “12 meals per household” per distribution.48 The range of calculated maximum amounts of food offered by box programs was 192 pounds over 12 months47 to 360 pounds over 6 months56 per household. One box program varied the food amount by family size.48 Among all studies, distribution frequencies occurred once during the intervention (n = 2),46,54 weekly (n = 2),43,50 twice monthly (n = 3),47,52,56 monthly (n = 5),44,45,49,51,53 and at each clinic visit (n = 4).39,40,41,42 Duration of programs ranged from 1.5 months57 to one year,39,47,49 with an average duration of six months.
Education
Twelve articles described a nutritional education component in their intervention.43,45,47,48,49,50,51,52,53,55,56,57 These included cooking classes,43,47,48,49,52 nutrition classes,45,51,53 booklets,56 individual coaching,55,57 videos,47 and written recipes.47,50 Four studies reported on frequency and/or duration of education, which corresponded to 24 h total,47 16 h,52 monthly sessions,53 and four total sessions.55 Incentive redemption was explicitly tied to education session attendance in two studies,45,48 otherwise, education was not mandatory for incentive redemption. Healthcare clinic staff or providers (Clinician, Nutritionist or Health Educator) were involved in delivering nutrition education in four47,48,52,53 out of the 12 programs that offered nutrition education.
Behavioral outcomes
Fifteen studies reported on food consumption patterns, food purchasing and cooking habits, and physical activity.39,40,41,42,43,44,45,47,49,50,51,52,55,56,57 Twelve studies reported F/V intake with qualitative (n = 3) or quantitative (n = 9) tools. Among the quantitative assessments of F/V intake, two studies43,49 used non-validated tools, and seven39,41,45,47,51,52,57 used validated instruments. Statistical testing was conducted in five studies.39,41,45,47,51 All five showed significant increases in child F/V intake, with increases in fruit intake of 30% from 0.6 to 0.8 servings per day (PD)41 and 43% (from 0.8 to 1.3 cups PD),47 a 33% increase in vegetable intake (from 0.7 to 0.9 servings PD),39 and a 31% and a 7.5% increase in total F/V intake (from 5.2 to 6.8 cups PD45 and from 3.47 to 3.73 cups PD,51 respectively). Two studies statistically tested and reported the change in adult caretaker F/V intake. One found a significant increase in adult vegetable intake (from 2.22 to 2.44 servings PD) and fruit intake (from 2.05 to 2.46 servings PD),49 while the other found a non-significant increase in adult F/V intake.47 One study reported families were more likely to shop at an FM in the month following the intervention compared to non-participants.40 Four studies reported changes in physical activity outcomes,44,45,52,57 in one study the increase was statistically significant.52
Food insecurity outcomes
Eleven studies39,42,43,44,45,47,49,53,54,55,56 evaluated changes in FI or food access; six used non-validated or qualitative assessment methods42,43,44,49,54,55 and five used validated FI instruments.39,45,47,53,56 Of these five, four39,45,47,53 measured FI severity using variations of the USDA Household Food Security Survey58 while the fifth56 used the Hunger Vital Sign (HVS) screener.59 Overall, these studies reported increased access to food, including F/V, and improved FI status of households. Among the five that utilized validated tools and conducted statistical testing, four reported significant improvements – two in FI status45,56 and two in FI severity.39,53 There were reported reductions in household FI status by 94% (100% at baseline to 5.9% at 6 months)56 and 17% (82% at baseline to 65% at 6 months)45 and reductions in FI severity by 55% (1.96 at baseline to 0.87 at 12 months)39 and 12.5% (from 0.72 at baseline to 0.81 at 6 months, this tool scored food security, so an increase is a reduction in FI severity).53 One study reported a “dose”-response effect on FI severity, indicating those with higher intervention participation (5–6 visits out of 6) had a greater reduction in FI severity than those who only attended 1–2 visits out of 6 (effect size β = 0.07).53 One reported non-significant improvements in FI severity.47 Only one study measured longitudinal change in FI as reported by the child and found a statistically significant reduction in their modified FI score from 1.88 at baseline to 1.04 at 12-months.39 Hager et al. reported household FI but it was not possible to disaggregate FI data in households with children from all households.51
Nutritional & culinary efficacy outcomes
Nutritional and culinary outcomes, including confidence, skills, knowledge, and attitudes towards the preparation, storage, consumption, and purchasing of foods, were reported by six studies.43,44,47,50,56,57 Three studies utilized qualitative measures43,44,50 and three utilized mixed measures,47,56,57 with two using validated questionnaires.47,57 There were no statistical analyses of nutrition and culinary outcomes, though all studies reported improved cooking skills and increased confidence in cooking, utilizing produce, and following recipes.
Health outcomes
Only three studies measured biometrics and health outcomes such as weight, body mass index (BMI),45,51,52 and health status51 in children. One study showed a statistically significant decrease in BMI z-score (95.6 to 73.1) in children who were classified as having overweight or obesity at baseline.45 The other studies found no significant effect of the intervention on child weight.51,52 One study measured change in health status on a five-point scale (poor, fair, good, very good, excellent), and found a statistically significant likelihood of improving one level from baseline after program participation (for example going from poor to fair, or fair to good).51 One study measured change in depression screening scores in adult mothers and found a reduction in scores in women in the intervention arm and no significant change in scores in women in the control arm.52
Feasibility
Feasibility was measured primarily by enrollment of target population, perceived positive impact, and satisfaction in interventions both by adult participants and medical providers. All seven studies which looked at feasibility reported that their interventions were feasible and acceptable within the intended population.44,46,47,48,50,55,56
Retention and redemption
Retention rates ranged from 27%44 to 4.5%.41 Redemption ranged from below 20%52,56 to 80% or greater.43,55 Retention and redemption reporting methods were not standard across studies and some studies did not explicitly report on retention or redemption rates of their participants.
Summary of qualitative
Qualitative responses revealed decreased financial hardship and increased access to healthy affordable food.42,44,47,50,54,56 Perceived improvements in F/V consumption, number of home cooked meals, and culinary skills and shopping habits were common.42,43,44,47,50,54,55 In addition, household-level attitude changes towards healthy eating, increased family time, and increased involvement of children in the cooking process were reported.43,44,47,50,54 Qualitative statements also captured site-specific barriers to participation, concerns over sustainability of perceived impacts after the program ends,57 and the importance of healthcare-based delivery of programs as a motivation for participation.44 Studies which evaluated feasibility through stakeholders including families, food vendors, and program assistants showed favorable responses towards their programs.55,56,57
Quality appraisal and limitations
The majority of studies were feasibility or pilot studies with small sample sizes, which limits their generalizability and ability to assess the impact of an intervention. MMAT results, as presented in Table 2, reflect acceptable quality with regard to feasibility outcomes. However, with respect to outcomes related to FI and F/V intake, there was a lack of high-quality methods, including not using validated assessment tools, having incomplete data, not controlling for confounders in the design and analysis, and lacking or inappropriate statistical methods.
Lessons Learned
We have highlighted some considerations for implementation of pediatric PRx interventions in Table 3.
Discussion
To our knowledge, this is the first scoping review to describe pediatric PRx interventions. There is a rising interest in pediatric PRx, which coincides with the recent national traction that FI, food inequity, and nutrition insecurity have received as major public health concerns and policy priorities in the U.S.60 Our work adds to previous reviews of PRx interventions by incorporating recently published studies and focusing on pediatric and caretaker outcomes related to FI, food intake, nutrition and culinary efficacy, and the family perspective. Additionally, it offers a summary of programmatic outcomes of retention, redemption, incentive amounts, nutrition education, and study design and quality limitations to help inform future work. Overall, the studies reviewed reported positive impacts of PRx towards FI, consumption of F/V, nutritional knowledge and culinary skill in households with children. However, more high-quality, rigorous observational cohort and RCT studies need to be undertaken to understand the best delivery and design of PRx interventions and their impact on behavior and health outcomes. This scoping review provides support for the need for further rigorous study and the potential for PRx to play a role in multi-pronged strategies that address FI and diet-related disease in children.
The emergent nature of pediatric PRx is reflected in the prevalence of pilot feasibility and acceptability studies utilizing non-randomized experimental designs. These studies provide a foundational understanding of the various design and implementation strategies of PRx interventions and explore their potential impact on FI and nutrition-related behavior and knowledge. They also provide a rich qualitative perspective of PRx participant experiences, which can help to define the priorities, needs, and assets of the individuals and communities for whom such interventions are being implemented. There was a wide diversity of study settings, a small number of studies, and lack of rigorous methods, limiting the ability to make generalizations about optimal PRx delivery models from this data. The review explored the relationship between PRx intervention characteristics (incentive amount, type, duration; retention and redemption; offering nutrition education, and assessment methods) and FI and produce intake outcomes but found no obvious patterns. As such, further studies are needed to determine the most efficacious intervention design. The optimal delivery and design of PRx interventions are also likely to differ based on the clinical context and the needs of the target population. Future PRx interventions should determine feasibility and efficacy within specific populations, focusing on strengths, challenges and cultural norms that impact participation and outcomes. The research highlighted herein suggests that increasing accessibility to healthy food by overcoming barriers related to transportation, cost, knowledge, and skills is an important part of interventions that positively impact healthy eating and purchasing patterns. Other research suggests prioritizing cultural considerations in food provision and educational programming is also important.61
An important next step in the research continuum for pediatric PRx is utilizing more rigorous study designs such as RCTs that include robust program evaluation methods, validated measurable outcomes, and sufficient sample sizes to detect statistically and clinically significant behavioral and health changes. While there are important ethical considerations to randomizing families with children for critically needed nutritional resources, RCTs can be conducted equitably with thoughtful methodology. For example, RCTs could explore PRx interventions with different frequencies, durations, delivery methods, produce quantities, participant choice, and various nutrition education components to better understand the efficacy of various PRx modalities and moderating factors. Programmatic outcomes such as retention and redemption rates should be reported to better understand the programmatic success and “dose” of produce prescription being provided.
While food as medicine approaches such as PRx are often used to treat disease in adult populations, a sole focus on treatment of disease may limit the potential impact of these interventions in children. The studies reviewed support the use of pediatric PRx as primarily preventive of adverse long-term health outcomes in children who are at-risk of diet related disease, while also addressing acute nutritional needs. PRx interventions offer an opportunity to impact the developmental trajectory of children by exposing them to a wide variety of tastes and flavors early in life, which promotes healthy eating behaviors later in life.62 Children typically have a slower onset of observable clinical abnormalities and visible signs of disease, however preventing diet-related, chronic disease through PRx may provide cost savings within the healthcare system in these future adults.63,64 Pediatric population health has the potential for impacts on a national level, as these current students will soon become workforce adults and eventually become utilizers of Medicare, so behavior changes now are perhaps incredibly powerful for long-term healthcare implications. As such, prevention-related markers, such as micro-environmental, self-efficacy, and behavioral changes, including increased F/V intake, nutritional knowledge gained, and improved food security, which are predictive of long-term health outcomes, may be highly appropriate outcomes to assess the impact of pediatric-focused PRx within a relatively healthy, resilient, and young population and long-term, cohort follow-ups in increments of 5 years would be beneficial. However, the choice of measured outcomes to assess impact, whether clinical metrics or behavioral or environmental proxies of health, will depend on the target population, program goals, duration of the study, and capacity of the research team.
Although some of the articles reviewed measured these proxy outcomes, it is difficult to compare across studies due to the heterogeneity of study designs and assessment tools used. The articles examined utilized three different methods to assess household FI: qualitative interviews, HVS screener, or variations of the USDA food security screener. Studies that utilize the HVS or qualitative tools are not able to determine severity of household FI, making cross-study comparison of the impact of PRx on FI depth difficult. Additionally, PRx interventions may reduce the severity of household and child-level FI rather than eliminate FI, making longitudinal assessments of household and child-level FI severity an important consideration of their evaluation. Standardized measurements are also needed for diet-related outcomes. The studies in this review that reported diet-related outcomes utilized a mix of qualitative, non-standardized single items, and standardized validated questionnaires. Previous adult PRx systematic and scoping reviews have also described difficulty encountering heterogeneous outcome measurements.32,65 A major step toward rigorously evaluating PRx interventions came with the 2018 Farm Bill, which funds the Gus Schumacher Nutrition Incentive Program (GusNIP). GusNIP attempts to standardize evaluation outcomes with shared metrics across studies.66 Forthcoming data will help identify optimal evaluation strategies that balance participant burden with the need for high-quality data and provide valuable insight into the impact of these programs. Future studies should consider using the free, validated, standardized tools identified by GusNIP to assess severity of FI and changes in F/V intake, in addition to any other stated primary outcomes, so comparison across studies can be done. Many PRx interventions are funded by philanthropic organizations in community health settings and may have little or no in-house technical support for evaluation. However, it is critical for PRx interventions to conduct program evaluation and research using standardized assessment methods and to disseminate results, which may require a multidisciplinary team of community, academic, and clinical collaborators and study budgets should reflect adequate funding for these efforts.
While interventions specifically addressing populations participating in FNPs were not included in this review, there is well-established evidence that these programs can improve FI, decrease poverty, and improve health outcomes.67 Although supplemental, these programs often comprise a major portion of family food budgets and remain inadequate for addressing the needs of families struggling with FI,68,69 leading to early benefit exhaustion associated with reduced perceived healthfulness of diet67,70 and maladaptive eating patterns.71 Furthermore, populations that face FI and diet-related chronic illnesses are often more likely to experience additional social risk factors, so effective strategies must continue to advocate for policies that comprehensively address social inequities related to the income and wealth gap that can co-occur in families with FI.72 PRx interventions can be one part of a multi-pronged approach, in addition to other policies aimed at enhancing the purchasing power of families with limited resources, including assistance for better income, housing, and employment opportunities, to buffer complex and multifactorial social determinants of health.73
Future studies should focus on exploring the impact and sustainability of PRx interventions within healthcare systems. Some barriers to the sustainability of PRx interventions include the cost, complexity, and capacity of integrating PRx within existing clinical settings.74 Although these interventions may require a large initial investment, they may provide long term healthcare cost savings. Additionally, the clinician-patient relationship may be enhanced by clinicians offering PRx as a resource for families with FI. Offering resources in response to positive clinical screening may serve as a “trust catalyst” when engaging with patients about social determinants or sensitive diet-related chronic disease topics.75 The success of integrating medically tailored meals (MTMs) within major state and private insurance systems serves as an example for the potential future of PRx at-large.76 To demonstrate impact and sustainability of pediatric PRx interventions, the field must undertake hypothesis-driven studies, powered to measure clinically significant changes in FI, and health-related behaviors and health outcomes. Additionally, future studies should conduct cost-effectiveness analysis with respect to healthcare utilization to understand the benefit of PRx within a healthcare system. Ultimately, if proven effective, the route of sustainability would be for federal policy to align and insurance coverage of PRx as medical interventions. A question remains, whether PRx interventions can be short-term interventions or whether they need to be sustained for a longer period of time to see long-term impacts. The goal may be to intervene during a window of opportunity, to expose, educate, and establish long-term healthy behaviors that can alter an individual’s trajectory of disease risk, putting them on a path of healthy lifestyle behaviors that will last a lifetime.
This study has some limitations. Eligible studies were limited to PRx interventions within a healthcare system, which excluded community and FNPs. While these are important programs, they were outside the scope of this review and have been described elsewhere.18,19,20,77 Search criteria were limited to the U.S. and excluded studies conducted before 2000. However, most studies were published within the last two years and have broad geographic range, making this scoping review timely and somewhat generalizable. Lastly, being a scoping review, the study was unable to measure aggregated outcomes and effect sizes across studies.
Conclusion
The studies explored here show that PRx interventions may support household food security and improve nutritional knowledge and F/V intake in children and adult caregivers. While quantitative health metrics are currently lacking, longer-term evaluation of pediatric PRx outcomes will help identify the impact of these programs on health outcomes across the lifespan. Additional research in this field should continue to explore qualitative experiences while also incorporating more rigorous study designs, larger sample sizes, quantitative analyses of behavioral and health outcomes, cost-effectiveness assessments, and tracking of healthcare utilization. This work will require a multi-disciplinary approach that includes the family unit, community resources, the healthcare team, payers, and trained evaluators with standardized tools to offer the most useful information to promote the advancement and integration of PRx interventions.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Mozaffarian, D., Hao, T., Rimm, E. B., Willett, W. C. & Hu, F. B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 364, 2392–2404 (2011).
Aune, D. et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 46, 1029–1056 (2017).
Afshin, A. et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393, 1958–1972 (2019).
Boushey, C. et al. Dietary patterns and all-cause mortality: a systematic review. https://nesr.usda.gov/2020-dietary-guidelines-advisory-committee-systematic-reviews/dietary-patterns-subcommittee/dietary-patterns-all-cause-mortality, https://doi.org/10.52570/NESR.DGAC2020.SR0108 (2020).
Lee, S. H., Moore, L. V., Park, S., Harris, D. M. & Blanck, H. M. Adults meeting fruit and vegetable intake recommendations — United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 71, 1–9 (2022).
Lange, S. J. et al. Percentage of adolescents meeting federal fruit and vegetable intake recommendations — Youth risk behavior surveillance system, United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 70, 69–74 (2021).
Chapman, K. et al. Exploring perceptions and beliefs about the cost of fruit and vegetables and whether they are barriers to higher consumption. Appetite 113, 310–319 (2017).
Mook, K., Laraia, B. A., Oddo, V. M. & Jones-Smith, J. C. Food security status and barriers to fruit and vegetable consumption in two economically deprived communities of Oakland, California, 2013–2014. Prev. Chronic Dis. 13, 150402 (2016).
Leung, C. W., Epel, E. S., Ritchie, L. D., Crawford, P. B. & Laraia, B. A. Food insecurity is inversely associated with diet quality of lower-income adults. J. Acad. Nutr. Diet. 114, 1943–1953.e2 (2014).
Kral, T. V. E., Chittams, J. & Moore, R. H. Relationship between food insecurity, child weight status, and parent-reported child eating and snacking behaviors. J. Spec. Pediatr. Nurs. 22, e12177 (2017).
Shankar, P., Chung, R. & Frank, D. A. Association of food insecurity with children’s behavioral, emotional, and academic outcomes: a systematic review. J. Dev. Behav. Pediatr. 38, 135–150 (2017).
USDA ERS - Key Statistics & Graphics. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/key-statistics-graphics/.
Te Vazquez, J., Feng, S. N., Orr, C. J. & Berkowitz, S. A. Food insecurity and cardiometabolic conditions: a review of recent research. Curr. Nutr. Rep. 10, 243–254 (2021).
Wurster Ovalle, V. M., Beck, A. F., Ollberding, N. J. & Klein, M. D. Social risk screening in pediatric primary care anticipates acute care utilization. Pediatr. Emerg. Care 37, e609–e614 (2021).
Palakshappa, D. et al. Food insecurity was associated with greater family health care expenditures in the US, 2016–17: study examines the relationship between food insecurity and family health care expenditures. Health Aff. (Millwood) 42, 44–52 (2023).
Tönnies, T. et al. Projections of Type 1 and Type 2 diabetes burden in the U.S. population aged; 20 years through 2060: the SEARCH for diabetes in youth study. Diabetes Care 46, 313–320 (2023).
Childhood Obesity Facts | Overweight & Obesity | CDC. https://www.cdc.gov/obesity/data/childhood.html (2022).
Chan, C. L., Tan, P. Y. & Gong, Y. Y. Evaluating the impacts of school garden-based programmes on diet and nutrition-related knowledge, attitudes and practices among the school children: a systematic review. BMC Public Health 22, 1251 (2022).
Seguin-Fowler, R. A. et al. Community supported agriculture plus nutrition education improves skills, self-efficacy, and eating behaviors among low-income caregivers but not their children: a randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 18, 112 (2021).
Briefel, R. R. et al. A cluster randomized controlled trial of a home-delivered food box on food security in chickasaw nation. J. Acad. Nutr. Diet. 121, S46–S58 (2021).
National Produce Prescription Collaborative - NPPC. National Produce Prescription Collaborative - NPPC https://www.nppc.health.
Mozaffarian, D., Blanck, H. M., Garfield, K. M., Wassung, A. & Petersen, R. A food is medicine approach to achieve nutrition security and improve health. Nat. Med. 28, 2238–2240 (2022).
Veldheer, S. et al. A systematic scoping review of how healthcare organizations are facilitating access to fruits and vegetables in their patient populations. J. Nutr. 150, 2859–2873 (2020).
What We Do. Wholesome Wave https://www.wholesomewave.org/what-we-do.
Oliveira, J. B., To, L., De La Cruz, Y. & Schneider, G. W. Prompting a fresh start for adults with food insecurity and increased bmi: a case series of four patients in a food prescription program. Cureus https://doi.org/10.7759/cureus.13857 (2021).
Schlosser, A. V. et al. “The coupons and stuff just made it possible”: economic constraints and patient experiences of a produce prescription program. Transl. Behav. Med. 9, 875–883 (2019).
Cook, M. et al. Food security and clinical outcomes of the 2017 Georgia fruit and vegetable prescription program. J. Nutr. Educ. Behav. 53, 770–778 (2021).
Bryce, R. et al. A pilot randomized controlled trial of a fruit and vegetable prescription program at a federally qualified health center in low income uncontrolled diabetics. Prev. Med. Rep. 23, 101410 (2021).
Cavanagh, M., Jurkowski, J., Bozlak, C., Hastings, J. & Klein, A. Veggie Rx: an outcome evaluation of a healthy food incentive programme. Public Health Nutr. 20, 2636–2641 (2017).
Johnson, J. K., Vingilis, E. & Terry, A. L. Patients’ experiences with a community fruit and vegetable box program prescribed by their health provider. BMC Public Health 23, 869 (2023).
Engel, K. & Ruder, E. H. Fruit and vegetable incentive programs for supplemental nutrition assistance program (SNAP) participants: a scoping review of program structure. Nutrients 12, 1676 (2020).
Bhat, S. et al. Healthy food prescription programs and their impact on dietary behavior and cardiometabolic risk factors: a systematic review and meta-analysis. Adv. Nutr. 12, 1944–1956 (2021).
Little, M. et al. Promoting healthy food access and nutrition in primary care: a systematic scoping review of food prescription programs. Am. J. Health Promot. 36, 518–536 (2022).
Arksey, H. & O’Malley, L. Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8, 19–32 (2005).
Peters, M. D. J. et al. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 13, 141–146 (2015).
Covidence - Better systematic review management. Covidence https://www.covidence.org/
Tricco, A. C. et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473 (2018).
Hong, Q. N. et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 34, 285–291 (2018).
Saxe-Custack, A., LaChance, J., Jess, J. & Hanna-Attisha, M. Influence of a pediatric fruit and vegetable prescription program on child dietary patterns and food security. Nutrients 13, 2619 (2021).
Saxe-Custack, A., Sadler, R., LaChance, J., Hanna-Attisha, M. & Ceja, T. Participation in a fruit and vegetable prescription program for pediatric patients is positively associated with farmers’ market shopping. Int. J. Environ. Res. Public. Health 17, 4202 (2020).
Saxe-Custack, A., LaChance, J. & Hanna-Attisha, M. Child consumption of whole fruit and fruit juice following six months of exposure to a pediatric fruit and vegetable prescription program. Nutrients 12, 25 (2019).
Saxe-Custack, A. et al. Caregiver perceptions of a fruit and vegetable prescription programme for low-income paediatric patients. Public Health Nutr. 21, 2497–2506 (2018).
Burrington, C. M., Hohensee, T. E., Tallman, N. & Gadomski, A. M. A pilot study of an online produce market combined with a fruit and vegetable prescription program for rural families. Prev. Med. Rep. 17, 101035 (2020).
Esquivel, M. K., Higa, A., Hitchens, M., Shelton, C. & Okihiro, M. Keiki produce prescription (KPRx) program feasibility study to reduce food insecurity and obesity risk. Hawaii J. Health Soc. Welf. 79, 44–49 (2020).
Jones, L. J. et al. Impact of a fruit and vegetable prescription program on health outcomes and behaviors in young Navajo Children. Curr. Dev. Nutr. 4, nzaa109 (2020).
Abel, D. et al. Assessment of a fruit and vegetable prescription program in the Northern Manhattan Community. Am. J. Health Promot. 36, 1014–1018 (2022).
Fischer, L. et al. Feasibility of a home-delivery produce prescription program to address food insecurity and diet quality in adults and children. Nutrients 14, 2006 (2022).
Woo Baidal, J. A. et al. Feasibility of food FARMacia: mobile food pantry to reduce household food insecurity in pediatric primary care. Nutrients 14, 1059 (2022).
Orsega-Smith, E., Slesinger, N. & Cotugna, N. Local pediatricians partner with food bank to provide produce prescription program. J. Hunger Environ. Nutr. 15, 353–359 (2020).
Brown, R. et al. Farm to families: clinic-based produce provision to address food insecurity during the pandemic. Pediatrics 150, e2022057118 (2022).
Hager, K. et al. Impact of produce prescriptions on diet, food security, and cardiometabolic health outcomes: a multisite evaluation of 9 produce prescription programs in the United States. Circ. Cardiovasc. Qual. Outcomes. e009520 https://doi.org/10.1161/CIRCOUTCOMES.122.009520 (2023).
Watt, T. T., Appel, L., Lopez, V., Flores, B. & Lawhon, B. A primary care-based early childhood nutrition intervention: evaluation of a pilot program serving low-income hispanic women. J. Racial Ethn. Health Dispar. 2, 537–547 (2015).
Ridberg, R. A. et al. A pediatric fruit and vegetable prescription program increases food security in low-income households. J. Nutr. Educ. Behav. 51, 224–230.e1 (2019).
Saxe-Custack, A. et al. Caregiver experiences with an innovative farmers’ market incentive program for children in Flint, Michigan. Glob. Pediatr. Health 6, 2333794×1987098 (2019).
George, D. R. et al. Examining feasibility of mentoring families at a farmers’ market and community garden. Am. J. Health Educ. 47, 94–98 (2016).
Aiyer, J. N. et al. A pilot food prescription program promotes produce intake and decreases food insecurity. Transl. Behav. Med. 9, 922–930 (2019).
Forbes, J. M., Forbes, C. R., Lehman, E. & George, D. R. “Prevention Produce”: integrating medical student mentorship into a fruit and vegetable prescription program for at-risk patients. Perm. J. 23, 18–238 (2019).
USDA ERS - Survey Tools. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/survey-tools/#six.
Hager, E. R. et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 126, e26–e32 (2010).
Biden-Harris Administration National Strategy on Hunger, Nutrition, And Health. https://www.whitehouse.gov/wp-content/uploads/2022/09/White-House-National-Strategy-on-Hunger-Nutrition-and-Health-FINAL.pdf (2022).
Maudrie, T. L., Colón-Ramos, U., Harper, K. M., Jock, B. W. & Gittelsohn, J. A scoping review of the use of indigenous food sovereignty principles for intervention and future directions. Curr. Dev. Nutr. 5, nzab093 (2021).
Scaglioni, S. et al. Factors influencing children’s eating behaviours. Nutrients 10, 706 (2018).
DeBoer, M. D. Assessing and managing the metabolic syndrome in children and adolescents. Nutrients 11, 1788 (2019).
True Cost of Food: Measuring What Matters to Transform the U.S. Food System. The Rockefeller Foundation https://www.rockefellerfoundation.org/report/true-cost-of-food-measuring-what-matters-to-transform-the-u-s-food-system/.
De Marchis, E. H. et al. Interventions addressing food insecurity in health care settings: a systematic review. Ann. Fam. Med. 17, 436–447 (2019).
Budd Nugent, N. et al. Accelerating evaluation of financial incentives for fruits and vegetables: a case for shared measures. Int. J. Environ. Res. Public. Health 18, 12140 (2021).
Malbi, J., Ohls, J., Dragoset, L., Castner, L. & Santos, B. Measuring the Effect of Supplemental Nutrition Assistance Program (SNAP) Participation on Food Security. (2013).
Gearing, M., Lewis, M., Wilson, C., Bozzolo, C. & Hansen, D. Barriers that Constrain the Adequacy of Supplemental Nutrition Assistance Program (SNAP) Allotments: In-depth Interview Findings. (2021).
Farson Gray, K., Balch-Crystal, E., Giannarelli, L. & Johnson, P. National- and State-level estimates of WIC eligibility and WIC program reach in 2019. (2022).
Castner, L., Henke, J. & Singh, A. “Benefit Redemption Patterns in the Supplemental Nutrition Assistance Program. (2011).
Kharmats, A. Y. et al. Relation between the supplemental nutritional assistance program cycle and dietary quality in low-income African Americans in Baltimore, Maryland. Am. J. Clin. Nutr. 99, 1006–1014 (2014).
Bowen, S., Elliot, S. & Hardison-Moody, A. The structural roots of food insecurity: How racism is a fundamental cause of food insecurity.
Bottino, C. J., Fleegler, E. W., Cox, J. E. & Rhodes, E. T. The relationship between housing instability and poor diet quality among urban families. Acad. Pediatr. 19, 891–898 (2019).
Auvinen, A., Simock, M. & Moran, A. Integrating produce prescriptions into the healthcare system: perspectives from key stakeholders. Int. J. Environ. Res. Public. Health 19, 11010 (2022).
Johnson, S. et al. “I Felt Like I Had Something I Could Do About It”: Pediatric clinician experiences with a food insecurity-focused produce prescription program. Clin. Pediatr. (Phila.) 000992282211506 https://doi.org/10.1177/00099228221150604 (2023).
Hager, K. et al. Association of national expansion of insurance coverage of medically tailored meals with estimated hospitalizations and health care expenditures in the US. JAMA Netw. Open 5, e2236898 (2022).
Burke, M., Cabili, C., Berman, D., Forrestal, S. & Gleason, P. A randomized controlled trial of three school meals and weekend food backpacks on food security in Virginia. J. Acad. Nutr. Diet. 121, S34–S45 (2021).
Acknowledgements
We would like to acknowledge the technical help and support from Thomas Harrod, MLS, MS, Associate Director Reference, Instruction, and Access, The George Washington University. No funding was secured for this study.
Author information
Authors and Affiliations
Contributions
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data (H.M., L.F., M.C., C.O., K.E.). Drafting the article or revising it critically for important intellectual content (H.M., L.F., M.C., N.K., C.L., C.O., K.E.). Final approval of the version to be published (H.M., L.F., M.C., N.K., C.L., C.O., K.E.).
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent to participate
No patient consent was required for this study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Muleta, H., Fischer, L.K., Chang, M. et al. Pediatric produce prescription initiatives in the U.S.: a scoping review. Pediatr Res 95, 1193–1206 (2024). https://doi.org/10.1038/s41390-023-02920-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-023-02920-8
