
Abstract
Background
Executive function (EF) develops throughout childhood and adolescence; however, little is known about whether and how early life factors are associated with EF during these two stages. This secondary analysis examined the associations between maternal psychological characteristics at 2 years after childbirth and offspring EF at 6 and 18 years.
Methods
Data were from the 18-year New Mothers’ Study in Memphis, TN. Women who self-identified as African-American were included (mother–child dyads: N = 414). Maternal psychological characteristics (e.g., depressive symptoms, self-esteem) were assessed using standardized questionnaires; offspring EF at 6 (i.e., working memory, response inhibition) and 18 years (e.g., working memory, sustained attention) were assessed using age-appropriate cognitive tasks. Statistical analyses included principal component analysis (PCA) and regression models.
Results
PCA reduced the correlated psychological characteristics to two factors: emotionality (depressive symptoms, emotional instability) and psychological resources (self-esteem, mastery, active coping). After controlling for maternal IQ, maternal emotionality was associated with worse working memory and response inhibition (marginally significant) at 6 years. Maternal psychological resources were marginally associated with better working memory at 6 years.
Conclusions
Maternal psychological characteristics may be associated with later EF in offspring. Future studies are needed to replicate these findings and to explore potential mediators.
Impact
-
African-American mothers’ depressive symptoms and emotional instability at 2 years after childbirth were associated with offspring executive function at 6 and 18 years.
-
African-American mothers’ psychological resources at 2 years after childbirth were marginally associated with offspring working memory at 6 years.
-
Maternal IQ attenuated all of the associations observed between maternal psychological status and offspring executive function.
Similar content being viewed by others

Introduction
Executive function (EF) plays a fundamental role in every aspect of life: it supports a set of higher-order cognitive processes such as reasoning, planning, and problem-solving, regulates thoughts and emotions, assists with goal-directed behaviors, and enables an individual to successfully perform complex tasks.1 EF initially manifests as a unidimensional component, but it gradually dissociates into several related but separate sets of cognitive abilities as children transition into school age and adolescence.2 Although there is no consensus about what specific cognitive abilities should be included in EF, it is well accepted that working memory, inhibition, and decision making are three important ones.1
Working memory refers to the storage and manipulation of verbal or visual–spatial information over a short period of time, and the stored information interacts with long-term memory to facilitate ongoing cognitive tasks.3 Inhibition includes two distinguishable components—response inhibition and attentional inhibition, which describe the suppression of goal-irrelevant behavioral responses and distracting stimuli, respectively.4 Attentional inhibition is, by definition, close to sustained attention, which conceptualizes the ability to maintain focus on a task that is non-arousing. Decision-making is considered a higher-order EF underpinned by working memory and inhibition, and one of its specific types is risky decision-making. Individuals who have deficits in risky decision-making are likely to choose the option that may generate positive outcomes in the short term but carry uncertain or negative long-term consequences.5
Compelling evidence supports childhood and adolescence as critical developmental stages of EF.2,6 During these two stages, the prefrontal cortex, the key brain region associated with EF, grows rapidly and does not mature until early adulthood. Along with the anatomical brain development, functional studies have consistently shown that working memory (verbal, visual–spatial),7,8 response inhibition,9,10 and sustained attention9,10 dramatically improve during early childhood (birth to year 8) and continue to develop, although at a much slower rate, throughout adolescence into the early 20s. The developmental trajectory tends to be distinct for risky decision-making, as adolescents often make more risky decisions than younger children.11,12 Meanwhile, despite the ongoing development of EF, children and adolescents often have an increasing demand for EF to support growing independence, autonomy, and new sets of responsibilities. These challenges further contribute to vulnerability to EF deficits during childhood and adolescence.
Deficits in working memory, inhibition, and risky decision-making individually increase the risk for a broad spectrum of neurocognitive (e.g., attention deficit hyperactivity disorder13), mental (e.g., substance use,14 eating disorders15), and behavioral (e.g., self-harm16) disorders. Therefore, to optimize children’s and adolescents’ well-being, it is critical to understand the factors that may contribute to EF development.
EF development is sensitive to early caregiving environments, especially early parenting behaviors: longitudinal studies have shown that positive parenting behaviors (e.g., involvement, autonomy support) were associated with developmental gains in child EF, while negative behaviors (e.g., insensitivity) predicted lower performance in EF in offspring during later life stages.17,18,19,20 Parenting behaviors are strongly influenced by caregivers’ psychological characteristics, such as depressive symptoms, emotional instability (the tendency to lose emotional balance), self-esteem (the overall evaluation of one’s worth), mastery (the degree of one’s perceived control over life), and coping style. For instance, caregivers with more depressive symptoms tend to display insensitive parenting behavior,21 while those with higher levels of self-esteem, mastery, or active coping report less parenting stress, thus better parenting outcomes.22 In addition to influencing parenting behaviors, caregivers’ psychological status also impacts offspring stress responses (e.g., disrupted hypothalamic–pituitary–adrenal axis) and results in structural and functional brain changes,23 all of which have implications in EF development.
Despite the theoretical link between caregivers’ psychological characteristics and subsequent EF development in the offspring, limited research has empirically tested this relationship. Few studies have investigated maternal depressive symptoms and documented a significant, prospective association with impaired EF (a composite of working memory and inhibition) in preschoolers (4–6 years old)21,24,25,26 and impaired inhibition in school-aged children.27 While these studies provide evidence that maternal psychological status is a potential determinant of offspring EF, the disproportional focus on childhood overlooks the important developmental period of adolescence. Furthermore, the narrow scope on depressive symptoms creates a missed opportunity for understanding the effect of a broader range of maternal psychological profiles (e.g., emotional instability, self-esteem, mastery, coping style) on offspring EF. Additional limitations include a lack of control of maternal characteristics that are known to influence child cognitive development (especially maternal intelligence quotient (IQ))24,25,26,27 and an insufficient presentation of mothers of young age and who are racial minorities, especially African-Americans (AAs).
AA mothers are unique in several ways. First, due to economic adversity, social disadvantage, deprived healthcare access, and racial discrimination, AA mothers experience more depressive symptoms and higher perceived stress at postpartum than their white counterparts.28 Second, there is evidence that AAs are less likely to use adaptive coping strategies when facing adverse events.29 Finally, although AAs report comparable or even higher self-esteem and mastery than whites,30,31 they tend to benefit less from these internal resources. In addition to the racial disparities, being a young mother is associated with challenges such as financial uncertainty, unstable partner relationship, and the need for their own development, all of which add psychological burden to motherhood.
Using data from a cohort of young, AA mothers and their firstborn children, the objective of this study was to examine the associations between maternal psychological characteristics at 2 years after the birth of their first child and the child’s EF at 6 and 18 years.
Methods
Study design
This is a secondary analysis using data from the 18-year follow-up New Mothers’ Study in Memphis, TN. The New Mothers’ Study was a randomized controlled trial that tested the effect of prenatal and infancy home visiting by nurses on maternal and child health and well-being. Women <29 weeks’ gestation with no previous live births and at least two sociodemographic risks (unmarried, <12 years of education, or unemployed) enrolled in 1990–1991. Enrolled women were randomly assigned to four treatment groups: (1) free transportation to prenatal care; (2) transportation to prenatal care and developmental screening for the children; (3) transportation to prenatal care, developmental screening, and prenatal home visits by nurses; and (4) transportation to prenatal care, developmental screening, prenatal home visits, and postnatal home visits through age 2 years by nurses. To reduce the cost of study, only mothers and their firstborn child from groups 2 (control) and 4 (intervention) were followed and assessed at 2, 6, 9, 12, and 18 years after the delivery of the child. The major features of the design have been reported earlier.32,33
Informed consent was obtained from all participants and the study was approved by University of Rochester Institutional Review Board. The New Mothers’ Study in Memphis, TN has been registered at www.clinicaltrials.gov (identifier NCT00708695). The consort diagram and consort checklist has been published elsewhere.33
Participants
To avoid the intervention effect, only mothers and their firstborn child from the control group (group 2) were included. Additional inclusion criteria were the following: (1) mothers completed the follow-up assessments at 2 years; (2) mothers’ firstborn child completed the follow-up assessments at 6 or 18 years; and (3) mothers self-identified as AA.
A total of 515 mothers were assigned to the control group, and 467 completed the 2-year assessment. Among these 467 mothers, 439 self-identified as AA. Among children of these 439 AA mothers, 25 did not complete the 6- or 18-year assessment and thus were excluded from analysis, resulting in a final sample size of 414.
Measurements
Maternal and child data were collected by staff masked to treatment assignment at 2, 6, 9, 12, and 18 years after delivery. For this analysis, maternal data at 2 years and child data at 6 and 18 years were used.
Maternal psychological characteristics at 2-year follow-up
Depressive symptoms were measured by the Depression subscale of the 38-item RAND Mental Health Inventory, which is widely used to assess psychological distress in the general population.34 The Depression subscale contains four items that queried the frequency that participants felt depressed, downhearted and blue, moody or brooded about things, and low or very low spirits during the past 30 days. Responses were scored with a Likert scale ranging from 1 to 5. A higher average score represents higher depressive symptoms.
Emotional instability was measured by the Loss of Behavioral or Emotional Control subscale of the RAND Mental Health Inventory. It includes 9 items that assess the frequency that participants felt in control or concerned about losing control of behaviors/emotions during the past 30 days. Responses were scored from 1 to 5, and a higher average score indicates higher emotional instability.
Self-esteem was measured by the 10-item Rosenberg’s Self-Esteem Scale, which is a well-known tool that assesses global self-esteem.35 Women were asked to rate how strongly they agree or disagree with the statements of positive and negative feelings about the self on a 4-point scale (1 = strongly disagree to 4 = strongly agree). A higher average score means higher self-esteem.
Mastery was measured by the seven-item Pearlin mastery scale, which is a validated tool to assess a person’s perceived control of their life.36 Responses to all items were rated on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree). A higher average score represents a greater sense of mastery.
Adaptive coping was measured by combining 3 subscales of the 60-item Coping Orientation to Problems Experienced scale, which was designed to measure effective and ineffective ways of coping with stressful life events.37 The three subscales were Use of Instrumental Social Support (four items), Active Coping (four items), and Planning (four items). Women were asked to rate the frequency of using coping strategies on a 4-point scale ranging from 1 (did not do at all) to 4 (did a lot). A higher average score means the more frequent use of adaptive coping.
Offspring EF at 6-year follow-up
Working memory was assessed by the Sequential Processing domain of Kaufman Assessment Battery for Children, which is a validated measure of intelligence and achievement for children aged 2.5–12.5 years.38 The Sequential Processing contains three subtests: Number Recall (the examiner presented a series of numbers, and the child was asked to repeat the numbers in the same sequence), Word Order (the examiner ordered a series of objects, and the child was asked to touch the objects in the same order), and Hand Movements (the examiner performed some hand movements, and the child was asked to imitate the movements). A higher global score of Sequential Processing means better working memory.
Response inhibition was measured by the Color-Word Stroop task.39 In this task, children were presented with several words that describe colors. Furthermore, the color ink of the word was not congruent with the meaning of the word (e.g., the word “red” was printed in green ink). Children were instructed to name the color ink of the presented word and to ignore the meaning of the word as quickly and accurately as possible. A higher number of errors means poorer response inhibition.
Offspring EF at 18-year follow-up
Working memory was measured by the Digital Span subtest of the Wechsler Adult Intelligence Scale, which is one of the most advanced instruments that evaluate the cognitive ability of individuals 16 years of age and older.40 In this test, adolescents were asked to listen to sequences of numbers orally and repeat them in a forward order, backward order, and ascending order. The score comprised the longest number of digits correctly repeated. For analysis, the raw scores were transformed to scaled scores based on chronological age, with higher scores representing better working memory.
Sustained attention was measured by the Attention Sustained subtest of the Leiter International Performance Scale, which has been widely used to examine individuals’ cognitive functioning.41 In the test, children were shown a page with target and non-target figures, and they were asked to mark the target figures and cross out non-target ones within certain time limits. The score was the number of correct responses, and the raw scores were converted to normalized scaled scores based on chronological age. A higher score indicates better sustained attention.
Risky decision-making was measured by a probabilistic gambling task.12 In this task, children were asked to choose one of the two “wheels of fortune” presented on a computer screen, with the aim of maximizing the number of points won. When the child made a choice, an arrow spun around the wheel and then stopped on the number of points won or lost. Based on the difference in expected value and actual outcomes between gambles, a coefficient for risk was generated—a high, positive coefficient indicates a more risky choice.12 For analysis, the proportion of risky and very risky choices were combined to represent risky decision-making.
Analysis
Statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). Continuous variables were described in mean and standard deviation; categorical variables were described in number and percentage. Missing data were assumed as missing at random, and no imputation was performed. A p value of <0.05 was considered statistically significant.
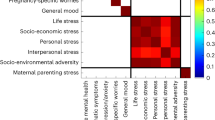
Considering that the five psychological characteristics (depressive symptoms, emotional instability, self-esteem, mastery, and coping styles) were significantly correlated with each other (at least r = 0.14, p < 0.01), a principal component analysis (PCA) was first conducted to minimize the multicollinearity by transforming the characteristics to new sets of linearly uncorrelated factors. The new factors maintain the variability and predictive value of the original characteristics. The PCA was exploratory and was performed with varimax orthogonal rotation. The sampling adequacy and suitability of using PCA were determined by the Kaiser–Meyer–Olkin (KMO) test and Bartlett’s Sphericity test, respectively. The decision on how to transform the five characteristics was based on considering the combination of interpretability, the eigenvalues (>1), and the loading value (≥0.50).42
Following PCA, linear regression models were used to evaluate the effects of the transformed factors with offspring EF at 6 and 18 years. Each EF component was examined separately. Given that maternal IQ has been reported as one of the strongest determinants of offspring cognitive functions,43 two regression models without (model 1) and with (model 2) adjustment for maternal IQ were built. In model 1, covariates considered included gestational age at delivery, pre-pregnancy body mass index (BMI), offspring sex, household income, maternal education, maternal employment, and marital status at 2-year assessment. To reduce the risk of overfitting the regression model, the binary association between each covariate with each EF component was first examined. Then the covariates with a p value <0.10 determined in this univariate analysis were carried into the multiple regression models. Based on the multiple regressions in model 1, model 2 further included maternal IQ as a covariate.
Results
Description of maternal and offspring characteristics
At randomization, mothers (N = 414) had a mean age of 17.94 ± 3.04 years. The mean pre-pregnancy BMI was 23.07 ± 5.00 kg/m2, and the mean gestational age at delivery was 39.07 ± 2.28 weeks (Table 1). At 2 years after childbirth, approximately one-third of mothers were employed (34.1%), and only a small portion of them were married (5.1%). Offspring sex was equally distributed (female: 50.2%; Table 2).
Principal component analysis
The sample was considered adequate because the KMO value was 0.68, which was higher than the threshold of 0.50. The p value of the Bartlett’s Sphericity test was <0.01, which supports the use of PCA and suggests that the characteristics can be transformed to at least two factors. After PCA, a two-factor solution was revealed (with eigenvalues >1, and loading value ≥0.50), accounting for 76.03% of the variance. Factor 1 comprised two characteristics (depressive symptoms, emotional instability) labeled as emotionality; factor 2 had three characteristics (self-esteem, mastery, active coping) named psychological resources (Table 3).
Associations of maternal emotionality and psychological resources with offspring EF
In model 1 (without adjusting for maternal IQ), maternal emotionality (higher levels of depressive symptoms and emotional instability) was associated with worse 6-year working memory (β = −1.87, 95% confidence interval (CI) −3.15, −0.60) and 6-year response inhibition (β = 0.37, 95% CI 0.02, 0.72) and marginally associated with 18-year working memory (β = −0.26, 95% CI −0.56, 0.03). In model 2 (adjusting for maternal IQ), the association between maternal emotionality and 6-year working memory was attenuated but remained significant (β = −1.79, 95% CI −3.05, −0.52). However, the significant association with 6-year response inhibition became marginally significant (β = 0.33, 95% CI −0.03, 0.68), and the borderline association with 18-year working memory disappeared (β = −0.22, 95% CI −0.52, 0.08).
Maternal psychological resources demonstrated limited association with offspring EF. In model 1, the association between psychological resources and 6-year working memory approached significance (β = 1.26, 95% CI −0.03, 2.56). This borderline association was further weakened by adding maternal IQ (β = 1.11, 95% CI −0.18, 2.41).
Maternal IQ was associated with four of the five examined EF components: working memory (β = 0.16, 95% CI 0.02, 0.29) and response inhibition (marginally significant, β = −0.04, 95% CI −1.94, 0.05) at 6 years, and working memory (β = 0.05, 95% CI 0.01, 0.08) and sustained attention (β = 0.05, 95% CI 0.02, 0.07) at 18 years.
Several covariates were significantly associated with offspring EF after accounting for maternal IQ. For example, children of mothers who were employed at 2 years after childbirth had better working memory (marginally significant, β = 0.65, 95% CI −0.01, 1.31) and sustained attention (β = 0.74, 95% CI 0.18, 1.31) at 18 years. Additionally, compared with female offspring, males had poorer 6-year working memory (marginally significant, β = −2.33, 95% CI −4.83, 0.16) and worse 18-year sustained attention (β = −0.76, 95% CI −1.28, −0.25) (Table 4).
Discussion
In this study, the associations between maternal psychological characteristics at 2 years after childbirth and offspring EF in childhood (6 years) and adolescence (18 years) were examined. Using PCA, the correlated psychological characteristics were transformed into two factors: emotionality (depressive symptoms, emotional instability) and psychological resources (self-esteem, mastery, and active coping). Regression models revealed that, after controlling for maternal IQ, maternal emotionality was associated with working memory and response inhibition (marginally significant) in offspring at 6 years; psychological resources were associated with working memory at 6 years (marginally significant).
The correlations among the psychological characteristics sorted by PCA are well supported by literature. For example, population-based studies and systematic reviews have consistently documented cross-sectional and prospective associations between depression and emotional instability.44,45 Genome-wide association studies and twin studies have revealed that these two constructs share moderate to substantial genetic architecture and environmental risk factors.46,47 Furthermore, Ormel et al.48 reviewed studies that addressed the relationship between emotional instability and common mental disorders (including depression) and found robust evidence in favor of the spectrum model (depression and emotional instability are intrinsically unified constructs but differ in severity levels, with depression reflecting the severe end of emotional instability). Similarly, self-esteem, mastery, and active coping have been acknowledged as personal-level psychological resources, which help people buffer against adverse life events and mental health problems.49
This study found that, before adjusting for maternal IQ, mothers’ emotionality (higher levels of depressive symptoms and emotional instability) at 2 years after childbirth was associated with worse working memory and inhibition control in offspring at 6 years and worse working memory at 18 years (marginally significant). Maternal IQ weakened all these observed associations, but maternal emotionality preserved its significance for 6-year working memory. Although no study has examined the combined effect of depressive symptoms and emotional instability on offspring EF, a few studies have reported a negative association between maternal depression and impaired working memory or inhibition in children of age 4–8 years.21,24,25,26,27 While these studies were conducted in white-dominant samples, focused on preschoolers and school-aged children, and did not consider maternal IQ in analysis, our study expanded previous findings to the AA population, added insight beyond childhood to adolescence, and provided stronger evidence by controlling for important maternal confounders (e.g., IQ).
To date, the focus of maternal influences on offspring EF development has been almost exclusively on negative exposures (especially depressive symptoms). Additionally, although there is evidence that maternal psychological resources (especially self-esteem) during postpartum protect offspring from developing mental and behavioral disorders,50,51 EF was not directly assessed in these studies. Our study helped fill these gaps by showing that maternal psychological resources favored offspring working memory at 6 years, although no statistical significance was achieved (before and after controlling for maternal IQ).
The large sample size of this study highlights alternative explanations, such as the unique features of the study population, that may account for the insignificant relationship between maternal psychological resources and offspring EF. First, this study comprised the AA population, and previous research has reported that AA women typically benefit less from internal psychological resources than white women.52,53 In other words, increased levels of self-esteem, mastery, or active coping may not result in large enough changes in maternal mental health54 and parenting behaviors,22,55 which breaks the link between maternal resources and offspring EF. Second, most mothers were in their adolescence when entering this study, thus at the 2-year assessment, many of them were still in their teens or early 20s. Unlike adult mothers, young mothers often reside with their families of origin, particularly with their own mothers.56,57 Consequently, grandmothers may take part in carrying out many of the child-caring responsibilities, weakening the maternal influences on offspring development. Third, young mothers are still striving for mental maturity and have a large potential to further build their self-esteem, gain mastery, and improve coping skills. Therefore, the later growth of these psychological resources may have a stronger impact on offspring EF development. Additionally, it should be noted that maternal psychological resources were measured 4–16 years before the offspring EF assessments. There is a possibility that the psychological resources influenced more proximal rather than distal EF, which were not captured in this study.
Maternal IQ was strongly associated with offspring EF, including working memory and response inhibition at 6 years and working memory and sustained attention at 18 years. This observation is not surprising as maternal IQ determines the genetic potential of offspring cognitive abilities, and previous studies have consistently associated maternal IQ with child neurocognitive development.58 Our study also showed that all the associations observed between maternal psychological characteristics and offspring EF were attenuated after adjusting for maternal IQ, underscoring the importance of including maternal IQ in studies of similar topics.
Surprisingly, maternal education—one of the most prominent socioeconomic factors that predict offspring cognitive development24,59—was not associated with any of the EF components. Instead, maternal employment that has been less studied contributed significantly to offspring EF. Specifically, children of mothers who were employed at 2 years after childbirth had better working memory at 6 years and better sustained attention at 18 years. The relationship between maternal employment and offspring cognitive function has been debated. While maternal employment may impose work–family conflict and decrease the quality of parenting, it can boost mothers’ well-being and may result in increased investments in children. Despite that maternal employment has been negatively linked to cognitive skills in white-dominant, school-aged children,60 our findings with AA participants coincide with one study that reported protective associations between maternal employment in the 2 years after childbearing and AA children’s cognitive function at age 7 years.61
The major strengths of this study include long-term follow-up that spanned a wide age range, a large sample size, the use of PCA that sufficiently considered the correlations between psychological characteristics, the use of performance-based rather than mother-reported cognitive assessments, and the control of maternal IQ in the analysis.
One of the main limitations of this study is the observational study design that did not allow a causal relationship to be established. Additionally, like other studies examining early life exposures and later offspring outcomes, this analysis could not fully adjust for the multitude of confounding variables, including genetic predisposition, postnatal environment, and offspring lifestyle behaviors (e.g., diet, sleep). This residual confounding is likely to cause an overestimation of the reported associations. Future research may benefit from animal studies or well-designed epidemiological studies to provide more accurate findings. An additional limitation is that maternal measurements were limited to the postnatal period. Given the evidence that maternal psychological distress during pregnancy influences fetal brain programming and subsequent neurodevelopment (e.g., attention deficit hyperactivity disorder),62,63 it is possible that the association observed between postnatal maternal psychological characteristics and offspring EF is confounded by the prenatal influences. Furthermore, there is evidence that, compared with single assessment, trajectory-based approaches can better capture child exposure to maternal risk or protective factors.25 However, because the New Mothers’ Study did not have consistent measures of prenatal and postnatal maternal psychological factors over time, trajectory analysis cannot be done. Other limitations of this study include, first, there is a lack of examination of maternal anxiety and stress, which are two well-studied risk factors of offspring cognitive development. Second, this study did not examine possible mediators between maternal psychological factors and offspring EF, such as parenting behaviors and offspring stress response. Third, there was a large time gap between maternal and offspring assessments. Future studies may benefit from including both proximal and distal offspring EF in analysis. Fourth, due to data availability, this study was not able to examine the paternal effects on offspring EF development or adjust for paternal factors in the analysis. An investigation of whether and how maternal and paternal interact to influence offspring EF is warranted in future research.
In conclusion, using a cohort of AA mothers and their firstborn child, this study found that maternal emotionality (depressive symptoms, emotional instability) and psychological resources (self-esteem, mastery, coping styles) were associated with working memory and/or response inhibition in offspring at 6 years, after adjusting for maternal IQ. Additionally, maternal IQ, maternal employment, and offspring sex demonstrated association with one or more of the offspring EF.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Diamond, A. Executive functions. Annu. Rev. Psychol. 64, 135–168 (2013).
Lee, K., Bull, R. & Ho, R. M. Developmental changes in executive functioning. Child Dev. 84, 1933–1953 (2013).
Baddeley, A. Working memory. Science 255, 556 (1992).
Sarter, M., Givens, B. & Bruno, J. P. The cognitive neuroscience of sustained attention: where top-down meets bottom-up. Brain Res. Brain Res. Rev. 35, 146–160 (2001).
Defoe, I. N., Dubas, J. S., Figner, B. & van Aken, M. A. A meta-analysis on age differences in risky decision making: adolescents versus children and adults. Psychol. Bull. 141, 48–84 (2015).
Xu, F. et al. Developmental differences in the structure of executive function in middle childhood and adolescence. PLoS ONE 8, e77770 (2013).
Swanson, H. L. Verbal and visual-spatial working memory: what develops over a life span? Dev. Psychol. 53, 971–995 (2017).
Brockmole, J. R. & Logie, R. H. Age-related change in visual working memory: a study of 55,753 participants aged 8-75. Front. Psychol. 4, 12 (2013).
Troller-Renfree, S. V. et al. Development of inhibitory control during childhood and its relations to early temperament and later social anxiety: unique insights provided by latent growth modeling and signal detection theory. J. Child Psychol. Psychiatry 60, 622–629 (2019).
Poon, K. Hot and cool executive functions in adolescence: development and contributions to important developmental outcomes. Front. Psychol. 8, 2311 (2017).
Dahl, R. E. Adolescent brain development: a period of vulnerabilities and opportunities. Keynote address. Ann. NY Acad. Sci. 1021, 1–22 (2004).
Burnett, S., Bault, N., Coricelli, G. & Blakemore, S. J. Adolescents’ heightened risk-seeking in a probabilistic gambling task. Cogn. Dev. 25, 183–196 (2010).
Ramos, A. A., Hamdan, A. C. & Machado, L. A meta-analysis on verbal working memory in children and adolescents with ADHD. Clin. Neuropsychol. 34, 873–898 (2020).
Ortal, S. et al. The role of different aspects of impulsivity as independent risk factors for substance use disorders in patients with ADHD: a review. Curr. Drug Abus. Rev. 8, 119–133 (2015).
Pearson, C. M., Zapolski, T. C. & Smith, G. T. A longitudinal test of impulsivity and depression pathways to early binge eating onset. Int. J. Eat. Disord. 48, 230–237 (2015).
Fikke, L. T., Melinder, A. & Landrø, N. I. Executive functions are impaired in adolescents engaging in non-suicidal self-injury. Psychol. Med. 41, 601–610 (2011).
Devine, R. T., Bignardi, G. & Hughes, C. Executive function mediates the relations between parental behaviors and children’s early academic ability. Front. Psychol. 7, 1902 (2016).
Bernier, A., Carlson, S. M. & Whipple, N. From external regulation to self-regulation: early parenting precursors of young children’s executive functioning. Child Dev. 81, 326–339 (2010).
Hughes, C. & Devine, R. T. For better or for worse? Positive and negative parental influences on young children’s executive function. Child Dev. 90, 593–609 (2019).
Bindman, S. W., Pomerantz, E. M. & Roisman, G. I. Do children’s executive functions account for associations between early autonomy-supportive parenting and achievement through high school? J. Educ. Psychol. 107, 756–770 (2015).
Wang, Y. & Dix, T. Mothers’ depressive symptoms in infancy and children’s adjustment in grade school: the role of children’s sustained attention and executive function. Dev. Psychol. 53, 1666–1679 (2017).
Hess, C. R., Papas, M. A. & Black, M. M. Resilience among African American adolescent mothers: predictors of positive parenting in early infancy. J. Pediatr. Psychol. 27, 619–629 (2002).
Anand, K. J. S. et al. Demographic and psychosocial factors associated with hair cortisol concentrations in preschool children. Pediatr. Res. 87, 1119–1127 (2020).
Hutchison, S. M., Mâsse, L. C., Brain, U. & Oberlander, T. F. A 6-year longitudinal study: are maternal depressive symptoms and selective serotonin reuptake inhibitor (SSRI) antidepressant treatment during pregnancy associated with everyday measures of executive function in young children? Early Hum. Dev. 128, 21–26 (2019).
Park, M., Brain, U., Grunau, R. E., Diamond, A. & Oberlander, T. F. Maternal depression trajectories from pregnancy to 3 years postpartum are associated with children’s behavior and executive functions at 3 and 6 years. Arch. Womens Ment. Health 21, 353–363 (2018).
Gueron-Sela, N., Camerota, M., Willoughby, M. T., Vernon-Feagans, L. & Cox, M. J. Maternal depressive symptoms, mother-child interactions, and children’s executive function. Dev. Psychol. 54, 71–82 (2018).
Jensen, S. K., Dumontheil, I. & Barker, E. D. Developmental inter-relations between early maternal depression, contextual risks, and interpersonal stress, and their effect on later child cognitive functioning. Depress. Anxiety 31, 599–607 (2014).
Cannon, C. & Nasrallah, H. A. A focus on postpartum depression among African American women: a literature review. Ann. Clin. Psychiatry 31, 138–143 (2019).
Van Gundy, K. T., Howerton-Orcutt, A. & Mills, M. L. Race, coping style, and substance use disorder among non-Hispanic African American and white young adults in south Florida. Subst. Use Misuse 50, 1459–1469 (2015).
Gray-Little, B. & Hafdahl, A. R. Factors influencing racial comparisons of self-esteem: a quantitative review. Psychol. Bull. 126, 26–54 (2000).
Twenge, J. M. & Crocker, J. Race and self-esteem: meta-analyses comparing whites, blacks, Hispanics, Asians, and American Indians and comment on Gray-Little and Hafdahl (2000). Psychol. Bull. 128, 371–408 (2002). Discussion 409–320.
Kitzman, H. et al. Effect of prenatal and infancy home visitation by nurses on pregnancy outcomes, childhood injuries, and repeated childbearing. A randomized controlled trial. JAMA 278, 644–652 (1997).
Olds, D. L. et al. Prenatal and infancy nurse home visiting effects on mothers: 18-year follow-up of a randomized trial. Pediatrics 144, e20183889 (2019).
Veit, C. T. & Ware, J. E. Jr The structure of psychological distress and well-being in general populations. J. Consult Clin. Psychol. 51, 730–742 (1983).
Rosenberg, M. Society and the Adolescent Self-Image (Princeton University Press, 1989).
Pearlin, L. I. & Schooler, C. The structure of coping. J. Health Soc. Behav. 19, 2–21 (1978).
Carver, C. S., Scheier, M. F. & Weintraub, J. K. Assessing coping strategies: a theoretically based approach. J. Pers. Soc. Psychol. 56, 267–283 (1989).
Boivin, M. J. et al. Neuropsychological benefits of computerized cognitive rehabilitation training in Ugandan children surviving severe malaria: a randomized controlled trial. Brain Res. Bull. 145, 117–128 (2019).
Stroop, J. R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 18, 643–662 (1935).
Wechsler, D. The Measurement and Appraisal of Adult Intelligence 4th edn (Williams & Witkins, 1958).
Roid, G., Pomplun, M. & Martin, J. Nonverbal Intellectual and Cognitive Assessment with the Leiter International Performance Scale-Revised (Leiter-R) (Wiley, 2009).
Osborne, J. W. Best Practices in Quantitative Methods (Sage Publications, 2008).
Faleschini, S., Rifas-Shiman, S. L., Tiemeier, H., Oken, E. & Hivert, M. F. Associations of prenatal and postnatal maternal depressive symptoms with offspring cognition and behavior in mid-childhood: a prospective cohort study. Int. J. Environ. Res. Public Health 16, 1007 (2019).
Navrady, L. B. et al. Intelligence and neuroticism in relation to depression and psychological distress: evidence from two large population cohorts. Eur. Psychiatry 43, 58–65 (2017).
Hakulinen, C. et al. Personality and depressive symptoms: Individual-participant meta-analysis of 10 cohort studies. Depress. Anxiety 32, 461–470 (2015).
Luciano, M. et al. Association analysis in over 329,000 individuals identifies 116 independent variants influencing neuroticism. Nat. Genet. 50, 6–11 (2018).
Kendler, K. S., Gatz, M., Gardner, C. O. & Pedersen, N. L. Personality and major depression: a Swedish longitudinal, population-based twin study. Arch. Gen. Psychiatry 63, 1113–1120 (2006).
Ormel, J. et al. Neuroticism and common mental disorders: meaning and utility of a complex relationship. Clin. Psychol. Rev. 33, 686–697 (2013).
Fukasawa, M., Watanabe, K., Nishi, D. & Kawakami, N. Longitudinal association between adolescent work values and mental health and well-being in adulthood: a 23-year prospective cohort study. Sci. Rep. 10, 13547 (2020).
Koutra, K. et al. Maternal depression and personality traits in association with child neuropsychological and behavioral development in preschool years: mother-child cohort (Rhea Study) in Crete, Greece. J. Affect. Disord. 217, 89–98 (2017).
Hetherington, E., McDonald, S., Racine, N. & Tough, S. Risk and protective factors for externalizing behavior at 3 years: results from the all our families pregnancy cohort. J. Dev. Behav. Pediatr. 39, 547–554 (2018).
Gayman, M. D., Cislo, A. M., Goidel, A. R. & Ueno, K. SES and race-ethnic differences in the stress-buffering effects of coping resources among young adults. Ethn. Health 19, 198–216 (2014).
Oates, G. L. & Goode, J. Racial differences in effects of religiosity and mastery on psychological distress: Evidence from national longitudinal data. Soc. Ment. Health 3, 40–58 (2013).
Assari, S. High sense of mastery reduces psychological distress for African American women but not African American men. Arch. Gen. Intern. Med. 3, 5–9 (2019).
Azar, S. T. et al. Maternal social information processing and the frequency and severity of mother-perpetrated physical abuse. Child Maltreat. 21, 308–316 (2016).
Oberlander, S. E., Black, M. M. & Starr, R. H. Jr African American adolescent mothers and grandmothers: a multigenerational approach to parenting. Am. J. Community Psychol. 39, 37–46 (2007).
Sellers, K., Black, M. M., Boris, N. W., Oberlander, S. E. & Myers, L. Adolescent mothers’ relationships with their own mothers: impact on parenting outcomes. J. Fam. Psychol. 25, 117–126 (2011).
Ronfani, L. et al. The complex interaction between home environment, socioeconomic status, maternal IQ and early child neurocognitive development: a multivariate analysis of data collected in a newborn cohort study. PLoS ONE 10, e0127052 (2015).
Madhushanthi, H. J., Wimalasekera, S. W., Goonewardena, C. S. E., Amarasekara, A. & Lenora, J. Socioeconomic status is a predictor of neurocognitive performance of early female adolescents. Int. J. Adolesc. Med. Health 32, 20180024 (2018).
Brooks-Gunn, J., Han, W. J. & Waldfogel, J. First-year maternal employment and child development in the first seven years. Monogr. Soc. Res. Child Dev. 75, 7–9 (2010).
Coley, R. L. & Lombardi, C. M. Does maternal employment following childbirth support or inhibit low-income children’s long-term development? Child Dev. 84, 178–197 (2013).
Manzari, N., Matvienko-Sikar, K., Baldoni, F., O’Keeffe, G. W. & Khashan, A. S. Prenatal maternal stress and risk of neurodevelopmental disorders in the offspring: a systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 54, 1299–1309 (2019).
Van den Bergh, B. R. H. et al. Prenatal developmental origins of behavior and mental health: the influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 117, 26–64 (2020).
Funding
New Mothers’ Study in Memphis, TN was supported with funding from 5 federal agencies: the National Institute of Nursing Research (grant NR01-01691-05); the Bureau of Maternal and Child Health (grant MCJ 360579); the Administration for Children and Families (grant 90PJ0003); the Office of the Assistant Secretary for Planning and Evaluation; and the National Center for Child Abuse and Neglect, through a transfer of funds to the National Institute of Nursing Research. This research was also supported by 4 private foundations: the Robert Wood Johnson Foundation, Princeton, NJ (grants 017934 and 11084); the Carnegie Corporation of New York, New York, NY (grant 5492); the Pew Charitable Trusts, Philadelphia, PA (grants 88-0211-000 and 93-02363-000); and the William T. Grant Foundation, New York, NY (grants 88-1246-88 and 91-1246-88), including a William T. Grant Faculty Scholars Award (86108086) and a Senior Research Scientist Award (1-K05-MH01382-01) to Dr. David L. Olds.
Author information
Authors and Affiliations
Contributions
Y.Y.: conception and design, interpretation of data, drafting and revising the article. Q.M.: analysis and interpretation of data, revising the article. S.W.G.: conception and design, acquisition of data, revising the article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Each participant in New Mothers’ Study in Memphis, TN provided informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yu, Y., Ma, Q. & Groth, S.W. Association between maternal psychological factors and offspring executive function: analysis of African-American mother–child dyads. Pediatr Res 92, 1051–1058 (2022). https://doi.org/10.1038/s41390-022-02084-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02084-x
This article is cited by
-
Imperative to accelerate research aligning real-time clinical demand with mental health supply
Pediatric Research (2022)
