
Abstract
Background
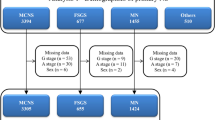
We analyzed the demographic and clinical characteristics of children with immunoglobulin A (IgA) nephropathy using data in the first pages of electronic health records of 22 hospitals from 2016 to 2018.
Methods
Information collected included gender, age, infection site, etiological infection, acute kidney injury (AKI), and chronic kidney disease (CKD) stages 2–5. We analyzed the gender and age distribution of children with IgA nephropathy, the characteristics of children complicated with AKI and CKD, and the influence of geographical distribution and economic status on the incidence of IgA nephropathy.
Results
We included a total of 4006 patients with IgA nephropathy. Incidence in males gradually increased with age. Seventy-nine cases (1.97%) had AKI. We found no significant difference in gender (P = 0.19) or age (P = 0.07) between the AKI and non-AKI groups. Twenty-nine patients had CKD (0.72%), who were significantly older than those in the non-CKD group (P < 0.0001). The incidence of IgA nephropathy in less-developed areas was significantly lower than that in developed areas (P = 0.0002).
Conclusions
The incidence of IgA nephropathy was high mainly in males. Age was an important factor affecting CKD. The disease was related to environment and economic status.
Impact
-
We analyze the demographic and clinical characteristics of children with immunoglobulin A (IgA) nephropathy using data in the first pages of electronic health records.
-
This is a large sample, multi-center study.
-
The incidence of IgA nephropathy in males increased gradually with age.
-
Age was an important factor affecting CKD.
-
The disease was related to environment and economic status.
Similar content being viewed by others

Introduction
Immunoglobulin A (IgA) nephropathy is one of the most common forms of glomerulonephritis. About 20–40% of patients gradually develop end-stage renal disease (ESRD) within 20 years after diagnosis. The incidence of IgA nephropathy varies with the social environment and the status of renal biopsy. In this study, the information in the first pages of electronic health records (EHRs) of children with IgA nephropathy during 2016–2018 was screened and statistically analyzed to explore the demographic and clinical characteristics of such children. We enrolled 22 hospitals affiliated with the Futang Research Center for Pediatric Development (Beijing, China).
Methods
Subjects
Primary and secondary diagnoses of children with IgA nephropathy younger than 18 years old were taken from the first pages of the EHRs of 22 hospitals during 2016–2018. Children were diagnosed by kidney biopsy. Secondary IgA nephropathies such as purpura nephritis and liver disease were excluded. Each patient’s repeat hospitalizations were counted as only one hospitalization. Hospitalization for primary renal disease during the same period was counted according to the International Statistical Classification of Diseases and Related Health Problems (ICD) code (N00.000–N07.901, N17.000–N17.904, N18–N18.8 [excluding N18.801–N18.806], N18.807–N19.03, N39.1–N39.2, and N39.201).
Data collection
The data collected were gender, age, infection site at diagnosis, infection etiology, acute kidney injury (AKI), chronic kidney disease (CKD; stages 2–5), total hospital cost, and average daily hospital cost.
Statistics
We compared differences between the groups. Pearson’s chi-square test was used for comparisons between groups with enumeration data. Measurement data were expressed as the mean ± standard error of the mean. The t test was used for comparisons between groups with normal distribution data with equal variances, and Wilcoxon’s test was used for comparisons between groups with normally distributed data with unequal variances. Results were considered statistically significant at P < 0.05. Analyses were performed using the SPSS 18.0 software.
Results
Subjects
We ultimately included 4006 patients with IgA nephropathy: 1268 patients who were treated in 2016, 1252 who were treated in 2017, and 1486 who were treated in 2018. A total of 33,235 cases of primary kidney disease (10,343, 10,698, and 12,194 cases per year, respectively) were included from 2016 to 2018.
Demographic characteristics
The results indicated that the age of children with IgA nephropathy (mean ± standard deviation [SD]) was 9.3 ± 3.0 years, the gender ratio (M/F) was about 2:1, and 93.6% were of Han nationality. IgA nephropathy is supposedly more common in adolescents, mainly in males. Different age groups had significantly different gender ratios (P < 0.0001). The gender ratio of the age group ≤5 years was significantly lower than that of the 6–13-year and 14–18-year age groups, but there was no difference in gender ratio between the latter two groups. Incidence in males increased gradually with age (Table 1). IgA nephropathy accounted for about 12% of all cases of primary kidney disease in 2016–2018. There was no significant difference among these years, and incidence was stable.
Infection in children with IgA nephropathy
Infection is an important cause of IgA nephropathy. Our results showed that, of the total 4006 patients, 1192 (29.8%) had co-infections. There was no significant difference in infection rate among all age groups (P = 0.12) (Supplemental Materials 1). Respiratory tract infection was the most common (1112/1192, 93.3%), followed by urinary tract (70/1192, 5.9%), digestive tract (25/1192, 2.1%), and other system (21/1192,1.8%) infections. Some children had more than two systemic infections. Mycoplasma, Streptococcus, and Tuberculosis were the first three known pathogens. Other pathogens such as Helicobacter pylori and chickenpox were also found.
Patients with IgA nephropathy complicated by AKI/CKD
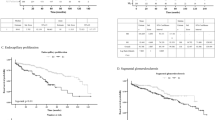
We extracted the information of patients with AKI/CKD stages 2–5 diagnosed during hospitalization from the first pages of their EHRs. Seventy-nine patients (1.97%) had AKI. There was no significant difference in gender (P = 0.19) or age (P = 0.07) between patients with or without AKI. The 29 patients (0.72%) in the CKD group were significantly older than the patients in the non-CKD group (P < 0.0001), but there was no significant difference in gender between these two groups (P = 0.37; Table 2).
Differences in IgA nephropathy among different regions and economic levels
According to the three-step distribution method, China is divided into the eastern, western, and northwestern regions (Fig. 1). Seven of the hospitals in this study serve the west and northwest: Gansu Provincial Maternity and Child Care Hospital, Inner Mongolia Autonomous Region Maternal and Child Health Hospital, Urumqi Children’s Hospital, Women and Children’s Hospital of Qinghai Province, The Children’s Hospital of Xi’an City, Kunming Children’s Hospital, and Guiyang Children’s Hospital. The remaining 15 hospitals are in the east. According to population density and economic level, China is divided into economically developed and underdeveloped regions (Fig. 2). The latter are served by Gansu Provincial Maternity and Child Care Hospital, Inner Mongolia Autonomous Region Maternal and Child Health Hospital, Urumqi Children’s Hospital, and Women and Children’s Hospital of Qinghai Province. The remaining 18 hospitals in this study are located in economically developed areas.

From www.dljs.net.

The purple line is the dividing line. From www.dljs.net.
Our results indicated that the proportion of IgA nephropathy patients to the primary kidney disease spectrum was different in the eastern and western regions (P < 0.0001). And the trend was same in the proportion of IgA nephropathy patients to total patients in the regions (P < 0.0001). There were significant differences in age, hospitalization cost, and length of stay between the two groups (P < 0.0001). Similarly, the proportion of IgA nephropathy patients to the primary kidney disease spectrum in economically underdeveloped areas was significantly lower than that in economically developed areas (P = 0.0002), and the patients were significantly older than those in economically developed areas (P < 0.0001). However, there was no significant difference in cost between the two regions (Tables 3 and 4).
Discussion
IgA nephropathy has attracted extensive attention due to its poor prognosis. In this paper, patients’ demographic and clinical characteristics were obtained from the first pages of their EHRs and analyzed.
The results showed that IgA nephropathy was more common in adolescents and that males were more prone to the disease. Our results were similar to the conclusions of two previous studies.1,2 Interestingly, we found that incidence of IgA nephropathy in males increased gradually with age, which was not mentioned in the previous studies. Adolescent boys are susceptible to IgA nephropathy. The prevalence of IgA nephropathy was stable in 2016–2018, and, annually, cases accounted for about 12% of the total cases of primary kidney disease. Data reported by 33 hospitals 15 years ago showed an increasing incidence of IgA nephropathy. Spectrum analysis of pediatric kidney disease in one hospital from 2014 to 2019 indicated an increasing proportion of IgA nephropathy.3 Another analysis showed that the prevalence of IgA nephropathy in the eastern region has increased over the past 5 years. IgA nephropathy accounts for 50% of renal biopsies and is becoming the most common glomerular disease.4
Mucosal infection is the most important mechanism of IgA nephropathy. In this study, 29.8% of children had infections, most commonly that of the respiratory tract. A variety of pathogens can induce IgA nephropathy.5,6,7 We know that paroxysmal gross hematuria occurs after respiratory tract infection. Acute pharyngopharyngeal infection triggers abnormal activation of the innate immune system in the pharynx. During acute infection, excessive activation of the innate immune system upregulates C-X3-C motif chemokine receptor 1 (CX3CR1)–fractalkine and releases pro-inflammatory factors that damage the renal epithelial cells, which can lead to hematuria. Continuous upregulation of CX3CR1–fractalkine in chronic inflammation might be an important factor in the persistent lack of remission and slow disease progression. Therefore, the pharyngorenal axis mechanism could be the focus of future research,8,9,10,11 and it also provides a theoretical basis for tonsillectomy in the treatment for IgA nephropathy. In addition, respiratory tract infection can cause intestinal–mucosal immune disorder, which induces the occurrence of diseases.12 Therefore, preventing recurrent infection is important.
In our results, patients with CKD (stages 2–5) were significantly older than those without. This suggested that age was an important risk factor for poor prognosis. Some studies have suggested that the prognosis of IgA nephropathy is related to gender and age and that males are more prone to disease progression than females.13 However, we saw no significant gender difference between the two groups. This might have been related to the small sample sizes and short follow-up period. However, we did find that the proportion of males increased with age, which seemed to support that male and age were the risk factors affecting the prognosis of IgA nephropathy. The mechanism needs further study.
The incidence of IgA nephropathy is related to heredity, race, and environment.14 A systematic analysis indicated that the incidence of the disease was higher in Asians than in people of European descent (e.g., 45 cases per million per year in Japan vs. 31 cases per million per year in France).15 There were significant differences in the proportion of IgA nephropathy and in patients’ age among groups from different regions and of different economic statuses. Usually, in our country, the economically underdeveloped areas are mostly located in the western or northwestern regions, so the prevalence of IgA nephropathy in the two areas may have a similar trend. Certainly, the status of renal biopsy in different regions can influence results, because biopsy is the gold standard for diagnosis of IgA nephropathy. Perhaps, renal biopsy is more conservatively ordered due to technical level, cost, and parent’s acceptance in economically underdeveloped areas or western/northwestern regions. Therefore, it is necessary to promote renal biopsy in these areas via technical assistance, education for parents, and economic development so as to improve early diagnosis and long-term prognosis.
In conclusion, we have obtained further understanding of the demographic and clinical characteristics of children with IgA nephropathy through analysis of data from the first pages of EHRs, which provided possible clues for precise treatment in future.
Materials availability
The materials described in the manuscript, including all relevant raw data, will be freely available to any researcher wishing to use them for non-commercial purposes, without breaching participant confidentiality.
References
The Subspecialty Group of Nephrology. The Society Pediatrics, Chinese Medical Association. Clinical and pathological manifestations of Chinese childhood patients with primary IgA nephropathy: a national collaborative study of 33 hospitals. Chin. J. Pediatr. 45, 272–278 (2007).
Working Group for National Survey on Status of Diagnosis and Treatment. Multicenter investigation of therapeutic status of children with IgA nephropathy in China. Chin. J. Pediatr. 51, 486–490 (2013).
Wang, L. et al. The disease spectrum analysis of children’s nephrology department in a hospital from 2014 to 2019. Chin. Med. Rec. 21, 65–68 (2020).
Zhou, Q. et al. Changes in the diagnosis of glomerular diseases in east China: a 15-year renal biopsy study. Ren. Fail. 40, 657–664 (2018).
Pérez, A. et al. IgA-dominant infection-associated glomerulonephritis following SARS-CoV-2 infection. Viruses 13, 587 (2021).
Shirai, Y. et al. Rapid progression to end-stage renal disease in a child with IgA-dominant infection-related glomerulonephritis associated with parvovirus B19. CEN Case Rep. 9, 423–430 (2020).
Filippatos, F., Tatsi, E. B. & Michos, A. Immune response to SARS-CoV-2 in children: a review of the current knowledge. Pediatr. Investig. 5, e12283 (2021). Online ahead of print.
Feriozzi, S. & Polci, R. The role of tonsillectomy in IgA nephropathy. J. Nephrol. 29, 13–19 (2016).
Osamu, H. & Takashi, O. The epipharynx-kidney axis triggers glomerular vasculitis in immunoglobulin A nephropathy. Immunol. Res. 67, 304–309 (2019).
Cox, S. N. et al. Activated innate immunity and the involvement of CX3CR1-fractalkine in promoting hematuria in patients with IgA nephropathy. Kidney Int. 82, 548–560 (2012).
Hotta, O., Tanaka, A. & Oda, T. Chronic epipharyngitis: a missing background of IgA nephropathy. Autoimmun. Rev. 18, 835–836 (2019).
Chen, C. J., Wu, G. H., Kuo, R. L. & Shih, S. R. Role of the intestinal microbiota in the immunomodulation of influenza virus infection. Microbes Infect. 19, 570–579 (2017).
Riispere, Ž. et al. IgA nephropathy clinicopathologic study following the Oxford classification: progression peculiarities and gender-related differences. Medicina 52, 340–348 (2016).
Kiryluk, K. et al. Geographic differences in genetic susceptibility to IgA nephropathy: GWAS replication study and geospatial risk analysis. PLoS Genet. 8, e1002765 (2012).
Schena, F. P. & Nistor, I. Epidemiology of IgA nephropathy: a global perspective. Semin. Nephrol. 38, 435–442 (2018).
Acknowledgements
We thank the members of Futang Research Center of Pediatric Development for the information of electronic health records, including Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, China; Dalian Children’s Hospital of Dalian Medical University, Dalian, China; Children’s Hospital of Hebei Province, Shijiazhuang, China; Inner Mongolia Autonomous Region Maternal and Child Health Hospital, Hohhot, China; Shanxi Children’s Hospital, Shanxi Maternal and Child Health Care Hospital, Taiyuan, China; Anhui Children’s Hospital, Hefei, China; Hangzhou Children’s Hospital, Hangzhou, China; Jinan Children’s Hospital, Jinan, China; The Affiliated Children’s Hospital of Nanchang University, Jiangxi Provincial Children’s Hospital, Nanchang, China; Liaocheng Children’s Hospital, Liaocheng, China; Nanjing Children’s Hospital Affiliated to Nanjing Medical University, Nanjing, China; Liuzhou Maternity and Child Healthcare Hospital, Liuzhou, China; Shenzhen Children’s Hospital, Shenzhen, China; Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China; Hunan Children’s Hospital, Changsha, China; Henan Children’s Hospital, Zhengzhou Children’s Hospital, Children’s Hospital Affiliated to Zhengzhou University, Zhengzhou, China; Gansu Provincial Maternity and Child Care Hospital, Lanzhou, Gansu Province, China; Women and Children’s Hospital of Qinghai Province, Xining, Qinghai, China; Urumqi Children’s Hospital, Urumqi, China; The Children’s Hospital of Xi’an City, Xi’an, China; Guiyang Children’s Hospital, Guiyang, China; and Kunming Children’s Hospital, Kunming, China. We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
N.Z., H.W., X.-y.W., and G.-s.F.: conception and design; N.Z., X.-y.W., Y.-p.J., Q.F., and Y.L.: acquisition of data or analysis; N.Z.: interpretation of the data and for drafting the article; H.W. revising the article critically; N.Z.: final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Zhou, N., Wang, H., Wang, Xy. et al. Characteristics of children with IgA nephropathy. Pediatr Res 93, 715–719 (2023). https://doi.org/10.1038/s41390-022-02080-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02080-1
