
Abstract
Background
Interleukin-1 receptor antagonist (IL1RN) variable number tandem repeats (VNTRs) are not fully understood in Type 1 diabetes mellitus (T1DM). It may affect IL1RN level and modify the disease risk. We aimed to study IL1RN VNTR polymorphism in Egyptian children with T1DM to clarify its potential role as a risk factor for T1DM and its effect on plasma IL1RN level.
Methods
A case-controlled study including 200 children (120 T1DM and 80 controls) was carried on. All children were subjected to genotyping of IL1RN VNTR. Plasma IL1RN was estimated by ELISA.
Results
The A1A2 and LS genotypes and A2 allele were significantly higher among cases compared to controls with increased T1DM risk (OR = 5.35, 2.56 and 3.13, respectively). The S allele was significantly elevated in cases compared to controls with 2.09-fold increased risk of having T1DM. The median plasma IL1RN significantly decreased in cases compared to controls. Within cases, IL1RN was significantly decreased in LS versus LL genotype.
Conclusions
There is a strong relationship between IL1RN VNTR and T1DM in Egyptian children. A1A1 genotype, LL genotype, A1 allele, and L allele were protective. A1A2 and LS genotypes, short (S), and A2 alleles were risk factors. IL1RN was decreased in T1DM, especially in LS genotype.
Impact
-
The relationship between IL1RN gene polymorphism and risk for T1DM among Egyptian children.
-
Plasma IL1RN protein level in T1DM.
-
Low IL1RN protein level in T1DM patients could be therapeutic targets for IL1RN medications in the future.
Similar content being viewed by others


Introduction
Type 1 diabetes mellitus (T1DM) is a chronic disease characterized by the inability of the body to produce insulin due to immune destruction of pancreatic beta cells. Although onset always occurs in children, the disease is possible in adults.1
Expression of interleukin-1 (IL1) and tumor necrosis factor-α (TNFA) has been revealed from islets of pancreas from T1DM, and these cytokines can cause beta cell destruction in vitro.2 IL1 family is a collection of 11 cytokines. IL1A and IL1B are the most studied elements, because they were discovered early and because they have strong pro-inflammatory effect. Interleukin-1 receptor antagonist (IL1RN) is a natural antagonist for them.3
IL1A, IL1B, and IL1RN bind IL1 receptor (IL1R). IL1RN organizes IL1A and IL1B pro-inflammatory action by competing with them for receptor’s binding sites.3 IL1RN is motivated to terminate the acute pro-inflammatory state and prevent chronic inflammation from destroying healthy cells. Functional polymorphism in cytokine genes can influence the levels of cytokine production. Altered levels of IL1RN have been demonstrated in the pathogenesis of several inflammatory or auto-immune diseases.4
IL1RN is expressed from IL1RN gene, which is located in chromosome 2, specifically 2q13-2q21.5 A polymorphism due to the presence of the 86 bp variable number tandem repeat (VNTR) has been demonstrated in intron 2 of the corresponding gene. This polymorphism resulted in the presence of six alleles, each of which corresponds to different number of repeats.6 The IL1RN VNTR is represented by 6 different alleles: the most frequent allele I (A1; 4 repeats, 412 bp), allele II (A2; 2 repeats, 240 bp), allele 3 (A3; 5 repeats, 498 bp), allele 4 (A4; 3 repeats, 326 bp), allele 5 (A5; 6 repeats, 584 bp), and allele 6 (A6; 1 repeat, 154 bp).7 These alleles are categorized by their length into long and short alleles. The long allele has >2 repeats. So A1, A3, A4, and A5 are long alleles (IL1RN*L); however, A2 and A6 are short alleles (IL1RN*S). The LL genotype is a genotype that has two long alleles and the SS genotype contains two short alleles. The LS genotype contains one long and one short allele.7 The biological actions of IL1RN and the accurate molecular effects of the IL1RN polymorphisms are not completely evident. Functional polymorphism may influence the level of IL1RN production.8
This study aims to study IL1RN VNTR polymorphism in Egyptian children with T1DM. We aimed also to clarify the potential role of this polymorphism as a risk factor for T1DM and to know its effect on the plasma level of the encoded protein (IL1RN).
Patients and methods
The study was carried out at the Pediatrics Department, Benha University Hospital in cooperation with the Medical Biochemistry and Molecular Biology Department during the period from April 2018 to June 2020. Informed written consent from parents of the children or health care providers was taken. The study was approved by the Ethical Committee of Benha University conferring to the World Medical Association Declaration of Helsinki.
Patients
This is a case–control study. It included 200 Egyptian children divided into two groups. Group 1 included 120 patients with T1DM whose ages ranged from 2 to 18 years. Group 2 included 80 age- and sex-matched healthy unrelated controls. Patients suffering diabetic complications were excluded.
Methods
Data were collected by physicians on a standard form. Diabetes mellitus was diagnosed according to the American Diabetes Association guidelines.9
All patients were subjected to:
-
Complete history taking, including age, sex, and history of the present illness, which included the onset of the disease, disease duration, manifestations of diabetes, insulin regimen, dose, and metformin use.
-
Full clinical examination with stress on body mass index (BMI), which was calculated by weight in kilogram divided by square of height in meters, BMI interpretation (underweight: BMI is below the 5th percentile, healthy weight: BMI is between 5th and 85th percentiles, overweight: BMI lies between 85th and 95th percentiles, and obese: BMI lies above the 95th percentile.10
-
Investigations that included complete blood count, liver and kidney function, serum electrolytes, albumin/creatinine ratio, thyroid functions, glycosylated hemoglobin (HbA1c), celiac screening, and fundus examination (if needed to exclude diabetic complications).
-
Genotyping of IL1RN VNTR and estimation of IL1RN plasma protein level.
Sampling
A 2-ml venous blood sample was withdrawn from each subject on ethylene diamine tetra-acetic acid (EDTA) and divided into 2 parts. One part (0.5 ml) was added to a sterile vacutainer tube for IL1RN VNTR. The other part (1.5 ml) was centrifuged at 3000 rpm to separate plasma for estimation of IL1RN protein level. Both EDTA blood and plasma were kept in sterile Eppendorf tubes at −80 °C for further assessment.
(A) Genotyping of IL1RN VNTR by DNA amplification and fragment size analysis:
Steps:
-
1.
Genomic DNA extraction: DNA was extracted from 100 µl EDTA blood sample by the Quick-DNATM Miniprep Kit (Zymo Research), including proteinase K for US-based manufacturers. Then Nanodrop 2000 (Thermo-Fisher Scientific, Wilmington) was used to detect DNA purity and concentration. Pure DNA preparations had an optical density ratio (260/280) of 1.7–2.11
-
2.
DNA amplification: Sequence-specific primers for IL1RN VNTR polymorphism (rs2234663; also called rs380092) were used; FP: 5′-CTCAGCAACACTCCTAT-3′ and RP: 5′-TCCTGGTCTGCAGGTAA-3′.12 The reaction mix for each sample contained: 3 µl extracted DNA, 1.5 µl FP, 1.5 µl RP, 12.5 µl Dream Taq Hot Start PCR master mix and up to 25 µl distilled water. The master mix and primers were supplied by Thermo Fisher Scientific Incorporation. The PCR conditions were initial denaturation (95 °C for 5 min) then denaturation (95 °C for 20 s), annealing (58 °C for 30 s) and extension (72 °C for 20 s) for 35 cycles and final extension at 72 °C for 10 min. PCR products (10 µl) and 100 base-pair ladder (5 µl) were run in 2.5% agarose gel with 0.3 µg/ml ethidium bromide to check PCR products. Bands were visualized using UV transilluminator (254 nm) and imaged with a digital camera 8 mega pixel and analyzed by the computer software (Alpha InoTech Gel Documentation System). The given bands of the amplified DNA of IL1RN VNTR were shown at 412 bp for A1allele, 240 bp for A2 allele, and 498 bp for A3 allele. The homozygous A1A1 genotype was represented on the gel by one band (412 bp). Other genotypes were represented on the gel by 2 bands; (412 bp and 240 bp for A1A2), (412 bp and 498 bp for A1A3) and (240 bp and 498 bp for A2A3) (Fig. 1).
Fig. 1: Agarose gel electrophoresis of IL1RN VNTR polymorphism. 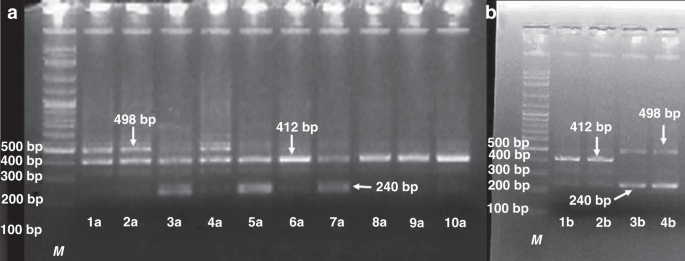
The A1A1 genotype is shown in lanes 6a, 8a, 9a, 10a, 1b, and 2b → 412 bp. The A1A2 genotype is shown in lanes 3a, 5a and 7a → 240 and 412 bp. The A1A3 genotype is shown in lanes 1a, 2a and 4a → 412 and 498 bp. The A2A3 genotype is shown in lanes 3b and 4b → 240 and 498 bp).

(B) Estimation of IL1RN protein by enzyme-linked immunosorbent assay (ELISA):
Quantitative sandwich ELISA estimation of human IL1RN protein in plasma was done using the Human Interleukin 1 Receptor Antagonist ELISA Kit (Wuhan Fine Biotech Co., Ltd., China). The kit sensitivity was 18.75 pg/ml. The detection range was 31.25–2000 pg/ml. The standard concentrations were 0, 31.25, 62.5, 125, 250, 500, 1000, and 2000 pg/ml. Optical density (OD) of the developed color was measured at 450 nm using Infinite F50 Absorbance Microplate Reader with the Magellan Tracker software (Tecan Trading AG, Switzerland). A standard curve was plotted on a graph paper with the OD on the horizontal axis and plasma IL1RN protein level (pg/ml) on the vertical one.13
Statistical methods
Data were collected and analyzed using SPSS vs.25. Numerical data were summarized as mean ± standard deviation (SD) or median and interquartile range. Categorical data were summarized as numbers and percentages. Comparisons between both groups were done using independent t test or Mann–Whitney U test (with z value) for numerical data after performing the normality test. Chi-square test or Fisher’s exact test, if appropriate, were applied for categorical data. Logistic regression analysis was used for calculating odds ratios (ORs) with 95% confidence intervals (CIs) for different genotypes and alleles. P value < 0.05 was considered significant.
Results
The demographic characteristics of the studied children
The present study included 200 Egyptian children: 120 diabetic patients (72 females and 48 males) and 80 healthy controls (42 females and 38 males). The mean age ± SD of patients was 9 ± 2 years. The mean age ± SD of the controls was 9 ± 3 years. There were no significant differences between patients and controls as regards age and sex (P = 0.946 and 0.458, respectively; Table 1).
The clinical characteristics within T1DM cases
Among patients, the mean ± SD of age at onset of diabetes was 9.17 ± 2.12 years. Mean ± SD of the disease duration was 5 ± 6 months. As regards BMI percentile, majority of cases were normal weight 40.0%, 33.3% of cases were underweight, 13.3% were overweight, and 13.3% were obese. As regards the associated disorders, celiac disease and Hashimoto thyroiditis were found in cases (4% for each). Ketoacidosis was seen in 83.3% of cases at the disease onset. The mean ± SD of HBA1c was 8.9 ± 1.4% (Table 2).
IL1RN VNTR genotype and allele distribution
In the current study, only A1, A2, and A3 alleles were obtained but the other alleles were not. Four different genotype categories were identified (A1A1, A1A2, A1A3, and A2A3). The LL genotype in the current study included A1A1 and A1A3 while the LS genotype included A1A2 and A2A3. The homozygous SS genotype (A2A2) was not found in this study (Table 3).
The A1A1 genotype was the commonest in the healthy controls (65.0%) compared to cases (28.3%). The A1A2 genotype was significantly higher among cases (58.3%) compared to controls (25.0%) with increased risk of occurrence of T1DM (OR = 5.35 and 95% CI = 2.11–13.59, P < 0.001). There was no significant difference between the 2 groups as regards A1A3 (P = 0.160) and A2A3 (P = 0.409) (Table 3).
On categorization of the studied groups by short allele carriers, there was significantly increased LS genotypes (A1A2 and A2A3) among cases compared to controls (60.0 versus 25.0%, respectively), with 2.56-fold increased risk of having T1DM and 95% CI of 1.67–3.90 (P < 0.001; Table 3).
The A1 allele was the commonest among controls (82.5%). The A2 allele was significantly elevated in cases (30.0%) compared to controls (12.5%) with higher risk of T1DM (OR = 3.13 and 95% CI = 1.44–6.78, P = 0.004). There was no significant difference between both groups as regards A3 allele (P = 0.402; Table 3).
With respect to the long (*L) and short (*S) alleles, the *S allele significantly increased among cases (30%) versus controls (12.5) with 2.09-fold increased risk of T1DM and 95% CI of 1.39–3.14 (P < 0.001; Table 3).
Plasma IL1RN protein level
The median plasma IL1RN protein level was significantly lower among cases (61.5 pg/ml) compared to controls (101.5 pg/ml) (P < 0.001; Fig. 2).

a T1DM versus controls, b LS versus LL genotype of T1DM. IQR interquartile range, ZMWU z value of Mann–Whitney U test, LL genotype with 2 long alleles, LS genotype with one short and one long allele.
On categorizing the cases by genotypes, IL1RN was significantly decreased in LS versus LL genotype among cases (P < 0.001). The median plasma IL1RN was 41.5 pg/ml in LS genotypes (A1A2 and A2A3) versus 87.0 pg/ml in LL genotypes (A1A1 and A1A3) (Fig. 2).
Discussion
IL1RN is considered a naturally occurring competitive inhibitor of IL1-produced pro-inflammatory action. It is produced by numerous cells that synthesize IL1B, especially pancreatic islets, hepatocytes, adipocytes, neutrophils, and macrophages.2 The number of 86-bp repeats in the IL1RN VNTR polymorphism of intron 2 does not change the IL1RN amino acid sequence but may be of functional importance as the repeated sequences contain putative binding sites for transcription factors.14 Our study revealed that the A1A2 genotype was significantly higher among cases compared to controls with increased risk of occurrence of T1DM by 5.35-fold. Also, the short allele carrier genotypes (LS; A1A2 and A2A3) significantly increased among cases compared to controls with 2.56-fold increased risk of having T1DM. The A2 allele was significantly elevated in cases compared to controls with higher risk of T1DM by 3.13-fold. With respect to long (*L) and short (*S) alleles, the *S allele significantly increased among cases versus controls with 2.09-fold increased risk of T1DM.
These findings agreed with a study performed on Saudi children with T1DM; the study demonstrated that IL1RN A2 allele and A1A2 genotype showed higher frequencies in T1DM than in controls and had nearly twice time risk of T1DM (OR = 1.97 for A1A2 genotype). And the short allele was associated with increased production of IL1RN.15 Moreover, the polymorphisms linked to TNFA and IL1RN genes were considered genetic markers for T1DM among Egyptians with an important impact on family counseling and management.16 Also, A2 allele of IL1RN gene was found to serve as susceptibility indicator for coronary artery disease in T2DM (OR = 2.2).17 In addition, homozygous persons for allele 2 of the IL1RN gene (A2A2) were reported to have more prolonged and severe pro-inflammatory reaction than those genotypes.18
IL1RN A2 allele was also related to the severity (diabetic nephropathy) in both types of diabetes rather than the susceptibility.19 In a study performed on the gene polymorphism of IL1RN and IL4 in Egyptian and other population, IL1RN and IL4 VNTR was found to have highly polymorphic content. Thus, VNTR were considered useful tools in genetic studies in population with different ethnic variations. These tools may help determine disease susceptibility and clinical management of patients.20 Also, many studies were confirming the association of IL1RN gene VNTR polymorphism with the risk of other diseases, such as breast cancer,21 cutaneous melanoma,22 osteoarthritis,23 and vitiligo.24
In contrast, our results disagreed with a previous study that showed non-significant difference in the A2 prevalence between cases and controls and concluded that IL1RN VNTR is not a diabetic marker.25
As regards the plasma IL1RN protein, the present study found significantly lower level in T1DM cases compared to controls. Among cases, IL1RN significantly decreased in the genotypes with short A2 allele (A1A2 and A2A3) compared to genotypes with long alleles. Our results agreed with some researchers who found that the plasma IL1RN levels were decreased among T2DM than non-diabetic controls (median IL1RN = 89 versus 140 pg/ml, respectively).17 In addition, a mild decline in the IL1RN levels was reported, 3 months after the onset of T1DM in patients not undergoing remission.26 Levels of IL1RN were positively associated with insulin resistance.27
Moreover, females with gestational diabetes had lower plasma IL1RN levels that was reported to be a marker for diagnosing and identifying gestational diabetes mellitus and those at risk of developing postpartum T2DM.28 IL1RN was related to the preserved β cell function in T1DM and was suggested to be a new therapeutic line.29
Pancreatic β cell-derived IL1RN is essential for the local defense of β cells to maintain normal function and proliferation.30 Also, administration of IL1RN successfully improved the β cell function in T2DM with enhanced insulin secretion and proper glycemic control pointing to the therapeutic potential of IL1 blockade.31 Intriguingly, a recombinant IL1RN (anakinra) is approved for use in humans as an anti-inflammatory therapy in many diseases, such as rheumatic diseases, ankylosing spondylitis, T2DM, and systemic inflammatory diseases.32 In addition, Dewberry and his colleagues studied IL1RN VNTR polymorphism in atherosclerosis and found that A2 allele was associated with reduced IL1RN.33
In contrast to our results, the anti-inflammatory IL1RN was reported to be the most elevated cytokine in the serum of T2DM patients.34 We disagree also with a former study that found lower IL1RN levels in T1DM (A1/A1) genotype compared with patients carrying (A1/A2) genotype.35 In Saudi children with T1DM, IL1RN levels were increased in A1A2 genotype children.15
This discrepancy concerning findings of the above-mentioned studies could be attributed to the different ethnicity, different experimental designs, and/or the presence of heterogeneity with other polymorphisms in the IL1RN gene.
Conclusion
There is a strong relation between IL1RN VNTR and T1DM in Egyptian children. A1A1 genotype, LL genotype, A1 allele, and long allele (L) were protective. A1A2 and LS genotypes, short (S), and A2 alleles were risk factors. IL1RN was decreased in T1DM, especially in LS genotype.
Recommendations
Further large-scale studies are needed to help other alleles of IL1RN VNTR to be presented. Low protein level in T1DM patients could be therapeutic targets for IL1RN medications in the future. Also, other polymorphisms in IL1RN gene should be studied.
References
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 32, S62–S67 (2009).
Burke, S. J. et al. Pancreatic deletion of interleukin 1 receptor disrupt whole body glucose hemostasis and promotes islet beta cell differentiation. Mol. Metab. 14, 95–107 (2018).
Dinarello, C. A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 117, 3720–3732 (2011).
Arend, W. P. The balance between IL-1 and IL-1Ra in disease. Cytokine Growth Factor Rev. 13, 323–340 (2002).
Nicklin, M. J., Weith, A. & Duff, G. W. A physical map of the region encompassing the human interleukin-1 alpha, interleukin-1 beta, and interleukin-1 receptor antagonist genes. Genomics 19, 382–384 (1994).
Kornman, K. S. et al. The interleukin-1 genotype as a severity factor in adult periodontal disease. J. Clin. Periodontol. 24, 72–77 (1997).
BorilovaLinhartova, P. et al. Interleukin-1 gene variability and plasma levels in Czech patients with chronic periodontitis and diabetes mellitus. Int. J. Dent. 2019, 6802349 (2019).
Rafiq, S. et al. Common genetic variation in the gene encoding interleukin-1-receptor antagonist (IL-1RA) is associated with altered circulating IL-1RA levels. Genes Immun. 8, 344–351 (2007).
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 33, S62–S69 (2010).
Kuczmarski, R. J. et al. CDC growth charts: United States. Adv. Data 8, 1–27 (2000).
Wilfinger, W. W., Mackey, K. & Chomczynski, P. Effect of pH and ionic strength on the spectrophotometric assessment of nucleic acid purity. Biotechniques 22, 478–481 (1997).
Hsu, M. J., Lu, Y. C., Hsu, Y. C., Liu, W. S. & Wu, W. T. Interleukin-1 receptor antagonist gene polymorphism in patients with multidrug-resistant Acinetobacter baumannii-associated pneumonia. Ann. Thorac. Med. 7, 74–77 (2012).
Deshpande, S. S. In Enzyme Immunoassays from Concept to Product Development 1st edn. Ch. 2 (International Thomson Publishing, 1996).
Clay, F. E. et al. Novel interleukin-1 receptor antagonist exon polymorphisms and their use in allele-specific mRNA assessment. Hum. Genet. 97, 723–726 (1996).
Ali, R. A., Sabe, L. M. & Al-harbi, A. M. A novel association between IL1-Ra (receptor antagonist) gene polymorphism and T1DM in Al-Madina Al-Mounawra. Eur. Rev. Med. Pharmacol. Sci. 19, 3701–3708 (2015).
Settin, A., Ismail, A., El-Magd, M. A., El-Baz, R. & Kazamel, A. Gene polymorphisms of TNF-alpha-308 (G/A), IL-10(-1082) (G/A), IL-6(-174) (G/C) and IL-1Ra (VNTR) in Egyptian cases with type 1 diabetes mellitus. Autoimmunity 42, 50–55 (2009).
Marculescu, R. et al. Interleukin-1 receptor antagonist genotype is associated with coronary atherosclerosis in patients with type 2 diabetes. Diabetes 51, 3582–3585 (2002).
Witkin, S., Gerber, S. & Ledger, W. J. Influence of interleukin-1 receptor antagonist gene polymorphism on disease. Clin. Infect. Dis. 34, 204–209 (2002).
Blakemore, A. I. et al. Interleukin-1 receptor antagonist allele (IL1RN*2) associated with nephropathy in diabetes mellitus. Hum. Genet. 97, 369–374 (1996).
El-Said, A. M., Abdel-Aziz, A. F., Settin, A. A. & El-Sharabasy, M. M. Incidence of genetic polymorphism of IL1-Ra and IL-4 in Egyptian and other populations. J. Am. Sci. 7, 806–814 (2011).
Al-Eitan, L. N., Al-Ahmad, B. H. & Almomani, F. A. The association of IL-1 and HRAS gene polymorphisms with breast cancer susceptibility in a Jordanian population of Arab descent: a genotype-phenotype study. Cancers 12, 283 (2020).
Cauci, S. et al. Interleukin 1 receptor antagonist gene variable number of tandem repeats polymorphism and cutaneous melanoma. Oncol. Lett. 18, 5759–5768 (2019).
Xu, B. et al. Meta-analysis of the association of IL1-RN variable number of tandem repeats polymorphism with osteoarthritis risk. Acta Orthop. Traumatol. Turc. 53, 497–501 (2019).
Singh, M., Mansuri, M. S., Jadeja, S. D., Marfatia, Y. S. & Begum, R. Association of interleukin 1 receptor antagonist intron 2 variable number of tandem repeats polymorphism with vitiligo susceptibility in Gujarat population. Indian J. Dermatol. Venereol. Leprol. 84, 285–291 (2018).
Copeman, J. B. et al. Linkage disequilibrium mapping of a type 1 diabetes susceptibility gene (IDDM7) to chromosome 2q31-q33. Nat. Genet. 9, 80–85 (1995).
Schloot, N. C. et al. Association of immune mediators at diagnosis of type 1 diabetes with later clinical remission. Diabetes Med. 24, 512–520 (2007).
Meier, C. A. et al. IL-1 receptor antagonist serum levels are increased in human obesity: a possible link to the resistance to leptin? J. Clin. Endocrinol. Metab. 87, 1184–1188 (2002).
Katra, P., Dereke, J., Nilsson, C. & Hillmnan, M. Plasma levels of the interleukin-1-receptor antagonist are lower in women with gestational diabetes mellitus and are particularly associated with postpartum development of type 2 diabetes. PLoS ONE 11, e0155701 (2016).
Pfleger, C. et al. Association of IL-1ra and adiponectin with C-peptide and remission in patients with type 1 diabetes. Diabetes 57, 929–937 (2008).
Böni-Schnetzler, M. et al. β cell-specific deletion of the IL-1 receptor antagonist impairs β cell proliferation and insulin secretion. Cell Rep. 22, 1774–1786 (2018).
Herder, C., Dalmas, E., Böni-Schnetzler, M. & Donath, M. Y. The IL-1 pathway in type 2 diabetes and cardiovascular complications. Trends Endocrinol. Metabol. 26, 551–563 (2015).
Abbate, A. et al. Anakinra, a recombinant human interleukin-1 receptor antagonist, inhibits apoptosis in experimental acute myocardial infarction. Circulation 117, 2670–2683 (2008).
Dewberry, R., Holden, H., Crossman, D. & Francis, S. Interleukin-1 receptor antagonist expression in human endothelial cells and atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 20, 2394–2400 (2000).
Ybarra, J. et al. Gender-based dimorphic pattern for interleukin-1 receptor antagonist in type 2 diabetes mellitus. Diabetes Metab. 34, 75–81 (2008).
Mandrup-Poulsen, T. et al. Monokine antagonism is reduced in patients with IDDM. Diabetes 43, 1242–1247 (1994).
Acknowledgements
Authors would like to thank all children and their parents who participated in this study. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
N.T.A., S.A.M., and E.M.E.-S.: contributed to the design and implementation of the research, aided in choosing the patients and helped shape the research, supervised the findings of this work, discussed the results, read and approved the final manuscript. I.A.R.: contributed to the design and implementation of the research, aided in choosing the patients, performed the laboratory work and helped shape the research, supervised the findings of this work, discussed the results, read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The current study was approved by the Medical Research Ethical Committee of the Faculty of Medicine, Benha University. All subjects were informed about the procedures and the aim of the study, and informed written consent was obtained from the parents or caregivers of enrolled children. The committee’s reference number is not available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Abed, N.T., Ramadan, I.A., Mohammed, S.A. et al. Genetic polymorphism of interleukin-1 receptor antagonist in Type 1 diabetic children. Pediatr Res 91, 1536–1541 (2022). https://doi.org/10.1038/s41390-021-01569-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01569-5
