
Abstract
Background
The level and lactonase activity of paraoxonase 1 (PON1) and their association with PON1 genetic variants and oxidative stress are unclear in neonates of women with gestational diabetes mellitus (GDM).
Methods
This study included 362 neonates of women with GDM and 302 control neonates. The level, lactonase activity, normalized lactonase activity (NLA), and genetic polymorphisms of PON1, serum total oxidant status (TOS), total antioxidant capacity (TAC), and malondialdehyde (MDA) were analyzed.
Results
The neonates of the women with GDM had significantly higher levels, lactonase activity, and NLA of PON1, higher TOS, TAC, and MDA concentrations, and relatively higher oxidative stress index than those of the control neonates. The PON1 −108C → T variation decreased the lactonase activity, level, and NLA of PON1, while the PON1 192Q → R variation decreased the PON1 NLA in a genotype-dependent manner in the two groups. Multivariable regression analysis revealed the PON1 −108C/T or 192Q/R variation, apolipoprotein (apo)A1, or apoB as significant predictors of the level, lactonase activity, and NLA of PON1.
Conclusions
The lactonase activity, level, and NLA of PON1 were increased in the neonates of women with GDM. The PON1 genetic variants, abnormalities in lipoproteins, and increased oxidative stress may be associated with these changes.
Impact
-
This is the first study to report the elevated level, lactonase activity, and NLA of PON1 in the neonates of women with GDM.
-
These neonates also exhibited increased oxidative stress and an adverse glycolipid metabolic profile.
-
We further established that the −108C/T and/or 192Q/R genetic variants of the PON1 gene, abnormalities in lipoprotein metabolism, and/or increased oxidative stress had noticeable influences on the level and activities of PON1.
-
Whether these changes potentially cause metabolic disorders later in life remains to be determined. Therefore, the neonates born to women with GDM require further clinical follow-ups.
Similar content being viewed by others

Introduction
Gestational diabetes mellitus (GDM) is defined as abnormal glucose tolerance with onset or first recognition during pregnancy.1 It is the most common metabolic disorder during pregnancy with a worldwide prevalence of 7–17% in different racial and ethnic groups, depending on the diagnostic criteria used.1,2,3 Gestational diabetes mellitus is not only seriously harmful to both the mother and fetus during pregnancy,1 but it is also associated with long-term health risks in the future, including the metabolic syndrome, type 2 diabetes mellitus (T2DM), and an increased risk of cardiovascular diseases for both the mothers and their offspring.1,4,5 While the pathogenesis of GDM is unclear, its occurrence and development have been linked to genetic variants, increased oxidative stress, and dyslipidemia.6,7,8
Paraoxonase 1 (PON1) is a calcium-dependent multifunctional enzyme anchored on high-density lipoprotein (HDL) molecules that has lactonase, Hcy-thiolactonase (HTase), paraoxonase (POase), and arylesterase (AREase) activities.9,10,11 The enzyme not only hydrolyzes several nerve agents and organophosphorus insecticides to protect against xenobiotic toxicity, but also degrades homocysteine thiolactone and oxidized lipids, inhibits the oxidation of low-density lipoprotein (LDL), reduces macrophage foam cell formation, and thus, has anti-inflammatory, antioxidative, and anti-atherogenic roles.9,10,11 It has been suggested that the physiological functions of PON1 are related to its lactonase and HTase activities,9,11 and the POase and AREase activities of PON1 are promiscuous.11,12 Previous studies have found that PON1 can hydrolyze lipid peroxides through its lactonase activity.11,13 Therefore, the lactonase test of PON1 can better reflect its antioxidative and anti-atherogenic properties compared to the POase and AREase tests.11,14,15
Some PON1 genetic polymorphisms can influence its specific activity or protein expression.10,11,16 The −108C/T polymorphism in the PON1 gene promoter region, a potential binding site for the Sp1 transcription factor, has an evident effect on PON1 gene expression, with the CC genotype expressing more PON1 than the TT genotype.10,16 The 192Q/R polymorphism of the PON1 gene, resulting from an amino acid substitution of glutamine (Q) with arginine (R) at codon 192, has been confirmed to affect PON1 activities in a substrate-dependent manner.10,11 The R isoform hydrolyzes lipid peroxides in vitro less efficiently than the Q isoform.10 The 192Q/R polymorphism has been associated with coronary heart disease,10,11 polycystic ovary syndrome (PCOS),17 and GDM.18
The total amount of antioxidant or oxidant molecules present in serum can be estimated by determining the total antioxidant capacity (TAC) or the total oxidant status (TOS), respectively.19,20 The redox imbalance can be evaluated by the oxidative stress index (OSI, the ratio of TOS to TAC).21
Oxidative stress plays an important role in the pathogenesis of GDM.8,16,22 Neonates of women with GDM demonstrate increased malondialdehyde (MDA) and decreased TAC.22 Decreased POase and AREase activities of PON1 and increased lactonase activity of PON1 in mothers with GDM have also been reported.16,23 However, to date, limited information is available regarding the level, activities, and 192Q/R and −108C/T genetic polymorphisms of PON1, TOS, and OSI in the neonates of women with GDM. In the present study, we investigated the lactonase activity and status of PON1 and their association with the −108C/T and 192Q/R variants of the PON1 gene and oxidative stress parameters in the neonates of women with GDM.
Materials and methods
Subjects
This case−control study consisted of 362 neonates of women with GDM and 302 neonates of women with uncomplicated pregnancies between 2013 and 2018. The subjects were recruited from the Department of Obstetrics and Gynecology of West China Second University Hospital. Written informed consent was obtained from all of the participants, and this study was approved by the Institutional Review Board of the West China Second University Hospital, Sichuan University.
At 24–28 gestational weeks, all the expectant mothers underwent a routine 75 g oral glucose tolerance test, and GDM was defined by the presence of one or more of the following features based on the guidelines of the International Association of Diabetes Pregnancy Study Groups (IADPSG):24 fasting glucose ≥5.1 mmol/L, 1 h glucose ≥ 10.0 mmol/L, or 2 h glucose ≥ 8.5 mmol/L. The neonates of women with uncomplicated pregnancies were recruited from the aforementioned department of the hospital during the same period.
The neonates were included if their mothers had GDM or uncomplicated pregnancies. Some mothers with GDM required insulin treatment. All the mothers had not taken any other medications except calcium (Caltrate), vitamins, minerals and trace elements for pregnant women (Elevit) regularly during pregnancy. All the neonates included in this study were singleton pregnancies and were delivered by cesarean section.
The neonates for cases and controls were excluded if their mothers met any one of the following exclusion criteria: diabetes mellitus (DM) before pregnancy; chronic hypertension; any other pregnancy complications, including pre-eclampsia and intrahepatic cholestasis of pregnancy, as well as cardiac, renal, and hepatic diseases; infectious, inflammatory, and autoimmune diseases that may affect oxidative stress; emergency cesarean delivery; and twin or multiple pregnancy.
Clinical and anthropometrical variables, including the height and weight of the neonates, systolic and diastolic blood pressures (SBP and DBP), and body mass index (BMI, kg/m2) of the mothers, were measured or assessed.
Fetal cord blood samples were collected from the umbilical vein at the time of cesarean section. The blood samples were placed on ice immediately and centrifuged at 1500 × g for 15 min at 4 °C within 4 h. The serum and plasma aliquots were stored at −80 °C for later analysis.
Analysis of PON1 activity, metabolic, and oxidative stress markers
The level and lactonase activity of PON1 were determined using 7-O-diethylphosphoryl-3-cyano-4-methyl-7-hydroxycoumarin (DEPCyMC) and 5-thiobutyl butyrolactone (TBBL) as substrates, respectively, based on the measurements described in our previous study.25 The following formula was used to establish normalized lactonase activity (NLA):15,25
Serum TOS and TAC were determined by the semi-automatic microplate colorimetric method as previously described.16,21 TOS was measured colorimetrically at 594 nm based on the oxidation of Fe2+ to Fe3+ in the presence of the oxidants contained in serum.19 The TOS level was computerized from the calibration curve for hydrogen peroxide (H2O2) and expressed in nanomolar H2O2 equivalents per milliliter serum (nmol H2O2 Equiv./mL). The measurement of TAC is based on the reaction of 2,2-azino-bis-3-ethylbenzothiazoline-6-sulfonic acid radical cation (ABTS˙+) with antioxidants present in serum.20 The TAC level was calculated from the calibration curve for Trolox (6-hydroxy-2,5,7,8-tetramethylchroman-2-carboxylic acid). The results were expressed in terms of millimolar Trolox equivalent per liter (mmol Trolox Equiv./L). OSI (arbitrary unit) expressed the ratio of TOS to TAC. Serum MDA was measured colorimetrically at 532 nm by the thibabituric acid reactive substance method using MDA kits (NanJing Jiancheng Bioengineering Institute, Nan Jing, China). MDA level was calculated from the calibration for 1,3,3,3-tetraethoxypropane.
The serum triglyceride (TG), total cholesterol (TC), HDL-cholesterol (HDL-C), LDL-cholesterol (LDL-C), apolipoprotein (apo)A1, and apoB levels, plasma insulin (Ins) and glucose (Glu) concentrations, as well as the homeostatic model assessment of insulin resistance (HOMA-IR) were measured or assessed as previously described.25,26
The intra- and inter-assay coefficients of variation for all of the measurements were less than 5% and 10%, respectively.
Genotype analysis
The genomic DNA was isolated from the cord blood leukocytes of the subjects and PON1 192Q/R and −108C/T genotypes were assessed by PCR amplification and restriction analysis as previously described.16,17
Statistical analyses
The probability distributions of all continuous variables were checked using the Kolmogorov−Smirnov test. For the normally distributed variables, the data are expressed as the mean ± standard deviation (SD). For the non-normally distributed variables, the data are expressed as the median (25th–75th percentile value). If a variable showed normal distribution before or after logarithmic transformation, the difference in variable between/among the groups/subgroups were evaluated with an independent sample t test or an analysis of variance (ANOVA). If not, the difference was evaluated by a Mann–Whitney U or Kruskal–Wallis H nonparametric test. The chi-squared (x2) test was used to determine the frequencies of macrosomia or genotypes between the two groups and to assess deviations of the genotype distribution from the Hardy–Weinberg equilibrium. Pearson’s correlation was used to evaluate how the level and activities of PON1 were associated with clinical, metabolic, and oxidative stress parameters in the neonates of women with GDM. Multivariate stepwise regression analyses were used to assess the effects of other parameters, including the −108C/T and 192Q/R genotypes of PON1; GDM status of the mothers (GDM = 1, control=0); gestation age, height and weight of the neonates; plasma insulin and glucose levels; and TG, HDL-C, LDL-C, apoAI, apoB, MDA, TOS, and TAC levels, on PON1 lactonase activity, level, or NLA; and the effects of the maternal clinical and metabolic parameters, including age, BMI at delivery, weight gain during pregnancy, the −108C/T and 192Q/R genotypes of PON1, PON1 lactonase activity, PON1 level, fasting insulin and glucose levels, TG, HDL-C, LDL-C, apoAI, apoB, MDA, TOS, and TAC levels,16 on PON1 lactonase activity, level, or NLA of the neonates. A value of P < 0.05 was considered statistically significant. All statistical analyses were conducted using the Statistical Program for Social Sciences (SPSS) 21.0.
PON1 lactonase activity was one of the main indicators in this study. A power calculation based on sample size and PON1 lactonase activity after logarithmic transformation was performed by the Power and Sample Size Calculations (PS) Program Version 3.1.6.
Results
Clinical characteristics of the mothers with and without GDM
As shown in Table 1, mothers with GDM tended to be of higher age, had higher SBP, pre-pregnancy BMI, and tended to have increased DBP, but demonstrated lower weight gain during pregnancy compared with the control mothers. Of the 362 women with GDM, 76 women required insulin treatment, while 286 women received dietary and exercise treatment only.
Clinical and biochemical characteristics of the neonates of mothers with and without GDM
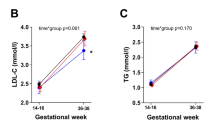
Compared with the neonates of the women with uncomplicated pregnancies, the neonates of the mothers with GDM had significantly higher fasting Glu, TG, TC, LDL-C, apoB, TOS, TAC, MDA, and PON1 levels, PON1 lactonase activity, as well as HOMA-IR, apoB/apoA1 ratios, and NLA, but lower gestational ages, as shown in Tables 1 and 2. They also tended to have increased frequency of macrosomia, fasting Ins, HDL-C levels, and OSI. A statistical power of 0.903 was achieved in the study for PON1 lactonase activity (within-group standard deviation = 0.13009, difference in the case and control means = 0.0331, significance level = 0.05).
PON1 genetic polymorphisms in the neonates of mothers with and without GDM
The genotypic distributions of the PON1 −108C/T and 192Q/R polymorphisms were in Hardy–Weinberg equilibrium in the neonates of mothers with and without GDM (all P > 0.05). No significant differences were observed in the frequencies of the PON1 −108C/T and 192Q/R genotypes between the neonates of the women with GDM and those with uncomplicated pregnancies (Table 2).
Lactonase activity, level, and NLA of PON1 and oxidative stress indexes according to PON1 genetic polymorphisms in the neonates of mothers with and without GDM
As shown in Table 3, the PON1 −108C/T variant decreased the level, lactonase activity, and NLA of PON1 in a genotype-dependent manner (CC > CT > TT) in the neonates of the women with and without GDM. The TAC level was higher in the CC genotype subgroup than the CT subgroup in the neonates of the women with GDM. The control neonates carrying the TT genotype had higher fasting Glu and Ins levels, as well as HOMA-IR than those carrying the CC genotype. They also had higher apoB/apoA1 ratios than the control neonates carrying CC or CT genotypes.
As shown in Table 4, the PON1 192Q → R variant decreased PON1 NLA in a genotype-dependent manner (QQ > QR > RR) in the neonates of women with and without GDM (P < 0.08), while PON1 lactonase activity was significantly decreased in the neonates with the RR genotype compared to those with QQ genotypes in both groups. The apoB/apoA1 ratios were increased and the PON1 lactonase activity decreased in the control neonates with the RR genotype than in the QR genotype.
We further compared the differences in variables between the neonates of women with GDM and the control neonates with the same genotype. Fasting Glu and Ins concentrations, HOMA-IR, TG, TAC, and MDA levels were significantly higher in the neonates of women with GDM than the control neonates in the CC genotype. Fasting Glu, TG, LDL-C, apoB, and TOS levels, the PON1 lactonase activity, as well as the apoB/apoA1 ratios were higher in the neonates of women with GDM than the control neonates in the CT genotype. HDL-C, TOS, and MDA levels were higher in the neonates of women with GDM than the control neonates in the TT genotype (Table 3). TG levels were higher in the neonates of women with GDM than the control neonates in the QQ genotype. Fasting Glu and apoB levels, HOMA-IR, and the apoB/apoA1 ratios were higher in the neonates of women with GDM than the control neonates in the QR genotype. Fasting Glu, TG, TC, HDL-C, apoB, TOS, and MDA levels, as well as the PON1 lactonase activity were higher in the neonates of women with GDM than the control neonates in the RR genotype (Table 4).
Relationship of the lactonase activity and status of PON1 with PON1 genetic variants, clinical, metabolic, and oxidative stress parameters in the neonates of mothers with and without GDM
Bivariate analysis in the neonates of women with GDM showed that the PON1 lactonase activity correlated positively with the level, NLA of PON1 (Fig. 1a, b), as well as apoA1, TC, HDL-C, LDL-C, apoB, TAC, and fasting Ins concentrations (r = 0.928, 0.800, 0.285, 0.217, 0.215, 0.184, 0.163, 0.150, and 0.133, respectively; all P < 0.05); the PON1 level correlated positively with the PON1 NLA (Fig. 1c), apoA1, TAC, TC, apoB, HDL-C, LDL-C, MDA, TG, and fasting Ins concentrations (r = 0.558, 0.287, 0.223, 0.214, 0.203, 0.202, 0.191, 0.150, 0.137, and 0.124, respectively; all P < 0.05); the NLA correlated positively with apoA1 and HDL-C (r = 0.193 and 0.136, respectively; all P < 0.05) and negatively with MDA levels (r = −0.132; P = 0.025).

Correlations between the level and lactonase activity (a), NLA and lactonase activity (b), and level and NLA (c) of PON1 in the neonates of women with GDM. PON1 paraoxonase 1, NLA normalized lactonase activity.
The multivariate stepwise regression analysis demonstrated that the PON1 −108C/T genetic variant, apoA1, and apoB levels were significant predictors of the PON1 lactonase activity; the PON1 −108C/T and 192Q/R genetic variants, apoA1, and apoB levels were significant predictors of the PON1 level, while the PON1 −108C/T genetic variant and apoA1 level were significant predictors of the NLA in all neonates (Table 5).
Relationship of clinical, metabolic and oxidative stress parameters, PON1 activities and genetic variants of the mothers with the PON1 lactonase activity and status as well as oxidative stress of the neonates
In the neonates of the women with GDM, bivariate analysis showed that the neonatal PON1 lactonase activity correlated positively with the lactonase activity and level of PON1 (r = 0.281 and 0.258, respectively; all P < 0.001) and negatively with weight gain during pregnancy (r = −0.149; P = 0.013) of the mothers; the neonatal PON1 level correlated positively with the level and lactonase activity of PON1 (r = 0.259 and 0.200, respectively; all P < 0.01) and negatively with weight gain during pregnancy and NLA (r = −0.184 and −0.138, respectively; all P < 0.05) of the mothers; the neonatal NLA correlated positively with the lactonase activity, level, and NLA of PON1 (r = 0.347, 0.225, and 0.274 respectively; all P < 0.001) and negatively with MDA levels (r = −0.150; P = 0.027) of the mothers. Our study also showed that the neonatal TOS, TAC, OSI, and MDA levels correlated positively with the maternal corresponding parameters (r = 0.654, 0.723, 0.818, and 0.367 respectively; all P < 0.001).
The multivariate stepwise regression analysis in all subjects demonstrated that the PON1 lactonase activity, HDL-C, PON1 −108C/T genetic variant, and MDA levels of the mothers were significant predictors of the neonatal PON1 lactonase activity; the PON1 level, apoA1, and PON1 −108C/T genetic variants of the mothers were significant predictors of the neonatal PON1 level, while the PON1 lactonase activity, PON1 level, MDA, HDL-C, and age of the mothers were significant predictors of the neonatal NLA (Supplementary Table 1).
Discussion
To the best of our knowledge, this is the first study to report the elevated level, lactonase activity, and NLA of PON1 in the neonates of women with GDM, indicating that a compensatory stimulation of PON1 lactonase activity may be present in these neonates. We also showed that the neonates of women with GDM had significantly higher TOS and MDA levels and relatively high OSI compared with the control neonates, suggesting that an increase in oxidative stress and redox imbalance exists in the neonates born to women with GDM. Furthermore, we established that the −108C/T and/or 192Q/R genetic variants of the PON1 gene, abnormalities in lipoprotein metabolism, and increased oxidative stress may be related to the changes of PON1 lactonase activity and status.
Pregnancy stress is related to an atherogenic lipid profile and increased oxidative stress in women.27,28 Compared with healthy pregnant women, mothers with GDM have more severe oxidative stress and display a more unfavorable glycolipid metabolism profile.8,16,22 Similar to mothers with GDM, neonates of women with GDM demonstrated increased fasting Glu and Ins concentrations, 8-isoprostane, xanthine oxidize, and MDA levels, and decreased TAC and levels/activities of antioxidative enzymes, such as superoxide dismutase and glutathione peroxidase when compared with control neonates.22,26 In the present study, we further showed that the neonates of women with GDM had higher serum TG, TC, LDL-C, apoB, TOS, TAC, HOMA-IR, apoB/apoA1 ratio levels, as well as relatively high OSI than the control neonates. These results demonstrate that neonates of women with GDM also exhibit an adverse lipid profile, increased oxidative stress, and tend to have a redox imbalance, suggesting that diabetic pregnancies have adverse implications for the fetal metabolism. ApoB and the apoB/apoA1 ratio have been reported to be reliable parameters in terms of predicting metabolic syndrome and coronary heart disease mortality29,30 and oxidative stress is a crucial mechanism underlying the pathogenesis of atherogenesis.31 It has been proposed that an unfavorable intrauterine environment could result in metabolic imprinting that might eventually cause some adult diseases.32 Therefore, the unfavorable glycolipid metabolism and oxidative stress in the neonates of women with GDM might be related to a higher risk of cardiometabolic diseases later in life.4,32
PON1 plays an antioxidant role by hydrolyzing lipid peroxides depending on its lactonase activity.10,12 Several studies have certified that the active sites of enzymes for the lactonase and promiscuous activities (POase and AREase activities) of PON1 are different.11,13 Impairing the lactonase activity of PON1 through mutations of the H115Q and H134Q catalytic histidine dyad reduces the ability of PON1 to prevent LDL oxidation and stimulate macrophage cholesterol efflux, indicating that the antioxidative and anti-atherogenic functions of PON1 may be mediated by its lactonase activity.13,33 In the present study, we found that the neonates of women with GDM had higher level, lactonase activity, and NLA of PON1 than the control neonates, suggesting that a compensatory increase in the expression and lactonase activity of PON1 observed in the neonates of women with GDM. The results of this study are similar to those of our previous studies demonstrating that the level and lactonase activity of PON1 are elevated in patients with PCOS and mothers with GDM.16,25 In addition, we found that the level and lactonase activity of PON1 remain low at birth, having only one-fourth to one-third of adult PON1 level or activity.16,25 Consistent with our results, Cole et al.34 demonstrated that the AREase activity of PON1 is low at birth, and plateaus between 6 and 15 months of age, with high inter-individual variability and a two- to seven-fold increase in PON1 activity from birth until levels reach a plateau. Maciejczyk et al.35 reported that the antioxidant barrier of saliva and blood is immature and inefficient in children, most effective in adults, and generally decreases with age. These findings suggest that infants and children may be more susceptible to oxidative stress and xenobiotic toxicity than young people and adults.
PON1 is one of the important antioxidant enzymes in blood circulation, and its activities and status are affected by oxidative stress.16,36 In the present study, we found that TAC correlated positively with the level and lactonase activity of PON1, and MDA levels correlated positively with the level of PON1, but negatively correlated with the NLA of PON1 in the neonates of women with GDM, suggesting that the elevated lactonase activity and level of PON1 and TAC might compensate for increased oxidative stress in the neonates of women with GDM. This is conducive to the hydrolysis and clearance of oxidized lipids; therefore, it has a protective role in these neonates. Contrastingly, PON1 is highly sensitive to variations in its milieu. Increased levels of oxidant molecules, such as reactive nitrogen and oxygen species and metals, can cause oxidative modification of PON1 and significantly inhibit the activities of the enzyme.36 Ardalic et al.37 reported that maternal smoking habits before pregnancy are associated with increased oxidative stress and decreased PON1 activity in healthy pregnant women. In brief, PON1 plays an important role in preventing oxidative stress, and the absolute or relative lack of PON1 lactonase activity may contribute to redox imbalance.
PON1 is anchored on HDL molecules in circulation, and its activities are influenced by plasma lipoproteins and apolipoproteins.38,39,40 ApoA1 or apoE combined with PON1 in HDL can markedly enhance the stability of PON1 and stimulate its lactonase activity.38,39 The dissociation of PON1 from HDL to the lipoprotein-deficient serum fraction is accompanied by a loss of PON1 lactonase activities and anti-atherogenic properties.41 TBBL, a synthetic chromogenic lactone, is similar to the natural lactone substrates of PON1 and can specifically evaluate PON1 lactonase activity.15,25 The DEPCyMCase activity of PON1 has been demonstrated to be a good marker of PON1 protein concentration because it is not influenced by the degree of catalytic stimulation by HDL and can provide information similar to the direct PON1 quantification by ELISA.15 The NLA of PON1, which is the ratio of TBBL to DEPCyMC activity, may reflect the level of PON1 lactonase catalytic stimulation by HDL.15,16 Thus NLA can estimate the status of PON1 very well. Small and dense proatherogenic LDLs have been associated with increased PON1 activity.40 In the present study, we showed that the level and lactonase activity of PON1 correlate positively with TC, HDL-C, LDL-C, apoA1, and apoB levels in the neonates of women with GDM. Multivariable regression analysis demonstrated that serum apoA1 and apoB levels are significant predictors of the level, lactonase activity, and NLA of PON1 in the neonates of women with and without GDM. Our findings support that the abnormalities in lipoprotein metabolism might be related to the complementary stimulation of PON1 lactonase activity in the neonates of women with GDM.
Several polymorphisms of the PON1 gene have been found to significantly influence the protein expression and/or activity of PON1 and account for more than 60% of the variation in enzyme concentrations and activity among individuals.10,25,38 Similar to previous findings,10,16 we demonstrated that PON1 −108C/T variant decreased the level and lactonase activity of PON1 in a genotype-dependent manner (CC > CT > TT); the 192R allele of the PON1 gene decreased the lactonase activity and NLA of PON1 in the neonates of women with and without GDM. We also showed that the PON1 −108C/T genetic variant was negatively correlated with the level, lactonase activity, and NLA of PON1; the 192Q/R genetic variant was a crucial predictor of the PON1 level in the neonates of women with and without GDM in the multivariate regression models. Besides the enzyme level and activities, the −108C/T and 192Q/R variants of the PON1 gene also have an evident effect on oxidative stress and glycolipid metabolism in the two neonate groups (Tables 3 and 4).
In addition, we further showed that neonatal TOS, TAC, OSI, and MDA correlated strongly and positively with the maternal corresponding parameters; the neonatal PON1 level and lactonase activity correlated negatively with the maternal weight gain during pregnancy. We also observed that the maternal PON1 level or lactonase activity, HDL-C, apoA1, MDA, PON1 −108C/T genetic variant or age are significant predictors of the neonatal PON1 level, lactonase activity or NLA in the multivariate regression models. Our findings suggest that −108C/T genetic variant, lactonase activity, and status of PON1; abnormalities in lipoprotein metabolism, increased oxidative stress, weight gain during pregnancy, aging of the mothers may have a significant effect on the PON1 lactonase activity, and status of their neonates. Whether the mothers’ influence on the neonates after birth would gradually disappear remains to be determined further.
The limitation of this study is that we measured the level and activities of PON1 and oxidative stress indexes in the neonates at birth only. Further studies that track and analyze the differences in enzyme activity and oxidative stress between the neonates of mothers with GDM and the age and sex-matched control neonates from birth to childhood might be needed to provide further insights.
In summary, the present study demonstrates increased level, lactonase activity, and NLA of PON1 in neonates born to women with GDM compared with the control neonates. These findings suggest that a compensatory stimulation of PON1 lactonase activity is present in neonates of women with GDM. We further proved that the −108C/T and/or 192Q/R variants of the PON1 gene, abnormalities in lipoprotein metabolism, and increased oxidative stress may be related to these changes. We also showed that the neonates of women with GDM exhibited an adverse glycolipid metabolism profile and an increase in oxidative stress compared with the control neonates. These findings suggest that the offspring exposed to a perturbed uterine environment may develop an aberrant metabolic status. Whether these changes potentially cause metabolic disorders later in life remains to be determined. Therefore, the neonates born to women with GDM require further clinical follow-ups.
References
Caughey, A. B. & Turrentine, M. ACOG practice bulletin no. 190: Gestational diabetes mellitus. Obstet. Gynecol. 131, e49–e64 (2018).
Gao, C., Sun, X., Lu, L., Liu, F. & Yuan, J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J. Diabetes Investig. 10, 154–162 (2019).
Lowe, W. L. Jr, Scholtens, D. M., Sandler, V. & Hayes, M. G. Genetics of gestational diabetes mellitus and maternal metabolism. Curr. Diab. Rep. 16, 15 (2016).
Tam, W. H. et al. In utero exposure to maternal hyperglycemia increases childhood cardiometabolic risk in offspring. Diabetes Care 40, 679–686 (2017).
Bellamy, L., Casas, J. P., Hingorani, A. D. & Williams, D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet 373, 1773–1779 (2009).
Ryckman, K. K., Spracklen, C. N., Smith, C. J., Robinson, J. G. & Saftlas, A. F. Maternal lipid levels during pregnancy and gestational diabetes: a systematic review and meta-analysis. Bjog 122, 643–651 (2015).
Zhang, C. et al. Genetic variants and the risk of gestational diabetes mellitus: a systematic review. Hum. Reprod. Update 19, 376–390 (2013).
Lopez-Tinoco, C. et al. Oxidative stress and antioxidant status in patients with late-onset gestational diabetes mellitus. Acta Diabetol. 50, 201–208 (2013).
Perla-Kajan, J. & Jakubowski, H. Paraoxonase 1 and homocysteine metabolism. Amino Acids 43, 1405–1417 (2012).
Precourt, L. P. et al. The three-gene paraoxonase family: physiologic roles, actions and regulation. Atherosclerosis 214, 20–36 (2011).
Camps, J., Marsillach, J. & Joven, J. The paraoxonases: role in human diseases and methodological difficulties in measurement. Crit. Rev. Clin. Lab. Sci. 46, 83–106 (2009).
Draganov, D. I. et al. Human paraoxonases (PON1, PON2, and PON3) are lactonases with overlapping and distinct substrate specificities. J. Lipid Res. 46, 1239–1247 (2005).
Rosenblat, M. et al. The catalytic histidine dyad of high density lipoprotein-associated serum paraoxonase-1 (PON1) is essential for PON1-mediated inhibition of low density lipoprotein oxidation and stimulation of macrophage cholesterol efflux. J. Biol. Chem. 281, 7657–7665 (2006).
Gugliucci, A. et al. Low protective PON1 lactonase activity in an Arab population with high rates of coronary heart disease and diabetes. Clin. Chim. Acta 445, 41–47 (2015).
Gaidukov, L. & Tawfik, D. S. The development of human sera tests for HDL-bound serum PON1 and its lipolactonase activity. J. Lipid Res. 48, 1637–1646 (2007).
Zhou, M. et al. Lactonase activity, status, and genetic variations of paraoxonase 1 in women with gestational diabetes mellitus. J. Diabetes Res. 2020, 3483427 (2020).
Wang, Y. et al. Evidence for association between paraoxonase 1 gene polymorphisms and polycystic ovarian syndrome in southwest Chinese women. Eur. J. Endocrinol. 166, 877–885 (2012).
Pappa, K. I., Gazouli, M., Anastasiou, E., Loutradis, D. & Anagnou, N. P. The Q192R polymorphism of the paraoxonase-1 (PON1) gene is associated with susceptibility to gestational diabetes mellitus in the Greek population. Gynecol. Endocrinol. 33, 617–620 (2017).
Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 38, 1103–1111 (2005).
Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 37, 277–285 (2004).
Zhang, R. et al. Oxidative stress status in Chinese women with different clinical phenotypes of polycystic ovary syndrome. Clin. Endocrinol. 86, 88–96 (2017).
Shang, M., Zhao, J., Yang, L. & Lin, L. Oxidative stress and antioxidant status in women with gestational diabetes mellitus diagnosed by IADPSG criteria. Diabetes Res. Clin. Pr. 109, 404–410 (2015).
Camuzcuoglu, H., Toy, H., Cakir, H., Celik, H. & Erel, O. Decreased paraoxonase and arylesterase activities in the pathogenesis of future atherosclerotic heart disease in women with gestational diabetes mellitus. J. Women’s Health 18, 1435–1439 (2009).
International Association of Diabetes Pregnancy Study Groups Consensus, Panel International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33, 676–682 (2010).
Zhang, Y. et al. Lactonase activity and status of paraoxonase 1 in Chinese women with polycystic ovarian syndrome. Eur. J. Endocrinol. 172, 391–402 (2015).
Gao, Q. et al. Activity and distribution of plasma platelet-activating factor acetylhydrolase in women with gestational diabetes mellitus and their neonates. Diabetes Metab. Res. Rev. 32, 634–642 (2016).
Stefanovic, A. et al. Association of the atherogenic index of plasma and oxidative stress status with weight gain during non-complicated pregnancy. Clin. Chem. Lab. Med. 50, 2019–2025 (2012).
Stefanovic, A. et al. Longitudinal changes in PON1 activities, PON1 phenotype distribution and oxidative status throughout normal pregnancy. Reprod. Toxicol. 33, 20–26 (2012).
Lee, Y. H., Choi, S. H., Lee, K. W. & Kim, D. J. Apolipoprotein B/A1 ratio is associated with free androgen index and visceral adiposity and may be an indicator of metabolic syndrome in male children and adolescents. Clin. Endocrinol. 74, 579–586 (2011).
Sierra-Johnson, J. et al. Concentration of apolipoprotein B is comparable with the apolipoprotein B/apolipoprotein A-I ratio and better than routine clinical lipid measurements in predicting coronary heart disease mortality: findings from a multi-ethnic US population. Eur. Heart J. 30, 710–717 (2009).
Navab, M. et al. The oxidation hypothesis of atherogenesis: the role of oxidized phospholipids and HDL. J. Lipid Res. 45, 993–1007 (2004).
Barker, D. J. The Wellcome Foundation Lecture, 1994. The fetal origins of adult disease. Proc. Biol. Sci. 262, 37–43 (1995).
Khersonsky, O. & Tawfik, D. S. The histidine 115-histidine 134 dyad mediates the lactonase activity of mammalian serum paraoxonases. J. Biol. Chem. 281, 7649–7656 (2006).
Cole, T. B. et al. Expression of human paraoxonase (PON1) during development. Pharmacogenetics 13, 357–364 (2003).
Maciejczyk, M., Zalewska, A. & Ladny, J. R. Salivary antioxidant barrier, redox status, and oxidative damage to proteins and lipids in healthy children, adults, and the elderly. Oxid. Med. Cell Longev. 2019, 4393460 (2019).
Aviram, M. & Vaya, J. Paraoxonase 1 activities, regulation, and interactions with atherosclerotic lesion. Curr. Opin. Lipido. 24, 339–344 (2013).
Ardalic, D. et al. The influence of maternal smoking habits before pregnancy and antioxidative supplementation during pregnancy on oxidative stress status in a non-complicated pregnancy. Adv. Clin. Exp. Med. 23, 575–583 (2014).
James, R. W. & Deakin, S. P. The contribution of high density lipoprotein apolipoproteins and derivatives to serum paraoxonase-1 activity and function. Adv. Exp. Med. Biol. 660, 173–181 (2010).
Gaidukov, L. et al. ApoE induces serum paraoxonase PON1 activity and stability similar to ApoA-I. Biochemistry 49, 532–538 (2010).
Vekic, J. et al. Association of oxidative stress and PON1 with LDL and HDL particle size in middle-aged subjects. Eur. J. Clin. Invest. 37, 715–723 (2007).
Rosenblat, M., Karry, R. & Aviram, M. Paraoxonase 1 (PON1) is a more potent antioxidant and stimulant of macrophage cholesterol efflux, when present in HDL than in lipoprotein-deficient serum: relevance to diabetes. Atherosclerosis 187, 74–81 (2006).
Acknowledgements
We thank the women with GDM and the control group women who donated cord blood samples for this study. We also appreciate Qian Gao for participating in the sample collection. This study was supported by the Key Research and Development Project of Sichuan Province (grant no. 2019YFS0401), the National Key Research and Development Program of China (grant no. 2016YFC1000400) and the Program for Changjiang Scholars and Innovative Research Team in University, Ministry of Education (grant no. IRT0935).
Author information
Authors and Affiliations
Contributions
M.Z. collected samples, conducted experiments, and wrote the paper. P.F. designed the experiments, analyzed the data, and revised the paper. X.-H.L. and M.C. were responsible for patient screening and helped with the sample collection. Q.-Q.L., C.-Y.J., and L.-B.G. assisted with the experiments. H.B. helped with the data analysis of the results and revised the paper. All authors read and approved the final manuscript to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical statement
The present study was approved by the Institutional Review Board of the West China Second University Hospital, Sichuan University. All subjects provided their written informed consent in accordance with the Helsinki Declaration of ethical conduct in research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Zhou, M., Liu, XH., Liu, QQ. et al. Lactonase activity and status of paraoxonase 1 and oxidative stress in neonates of women with gestational diabetes mellitus. Pediatr Res 89, 1192–1199 (2021). https://doi.org/10.1038/s41390-020-1023-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-1023-2
