
Abstract
Lithium is regarded as the first-line treatment for bipolar disorder (BD), a severe and disabling mental health disorder that affects about 1% of the population worldwide. Nevertheless, lithium is not consistently effective, with only 30% of patients showing a favorable response to treatment. To provide personalized treatment options for bipolar patients, it is essential to identify prediction biomarkers such as polygenic scores. In this study, we developed a polygenic score for lithium treatment response (Li+PGS) in patients with BD. To gain further insights into lithium’s possible molecular mechanism of action, we performed a genome-wide gene-based analysis. Using polygenic score modeling, via methods incorporating Bayesian regression and continuous shrinkage priors, Li+PGS was developed in the International Consortium of Lithium Genetics cohort (ConLi+Gen: N = 2367) and replicated in the combined PsyCourse (N = 89) and BipoLife (N = 102) studies. The associations of Li+PGS and lithium treatment response — defined in a continuous ALDA scale and a categorical outcome (good response vs. poor response) were tested using regression models, each adjusted for the covariates: age, sex, and the first four genetic principal components. Statistical significance was determined at P < 0.05. Li+PGS was positively associated with lithium treatment response in the ConLi+Gen cohort, in both the categorical (P = 9.8 × 10−12, R2 = 1.9%) and continuous (P = 6.4 × 10−9, R2 = 2.6%) outcomes. Compared to bipolar patients in the 1st decile of the risk distribution, individuals in the 10th decile had 3.47-fold (95%CI: 2.22–5.47) higher odds of responding favorably to lithium. The results were replicated in the independent cohorts for the categorical treatment outcome (P = 3.9 × 10−4, R2 = 0.9%), but not for the continuous outcome (P = 0.13). Gene-based analyses revealed 36 candidate genes that are enriched in biological pathways controlled by glutamate and acetylcholine. Li+PGS may be useful in the development of pharmacogenomic testing strategies by enabling a classification of bipolar patients according to their response to treatment.
Similar content being viewed by others

Introduction
Bipolar disorder (BD) is a severe and often disabling mental health disorder that affects more than 1% of the population worldwide and is characterized by recurrent episodes of depression and mania [1]. BD accounted for 9.3 million disability-adjusted life years (DALYs) in 2017, and imposes a significant social and economic burden on society and healthcare systems [2, 3]. BD is associated with a significant somatic and psychiatric comorbidity [1] and an increased risk of suicide [4].
Since the discovery of lithium’s mood-stabilizing property in 1949 [5], it has been widely used as a first-line therapy for patients with BD [6, 7]. Lithium is effective in treating acute episodes of illness and reduces the risk of future recurrences of mania and depression [8]. It has also been shown to reduce the risk of suicide [9]. Despite these merits, the efficacy of lithium is highly variable, with about 30% of treated patients showing a favorable response while more than 30% of them have no clinical response at all [8, 10]. Thus far, the causes and predictors of such heterogeneity in treatment response are insufficiently understood.
Genetic factors are thought to contribute, at least in part, to the large interindividual differences in response to lithium [10,11,12,13,14,15]. So far, only a few genetic studies have identified specific single nucleotide polymorphisms (SNPs) and candidate genes associated with patients’ response to lithium or treatment-related side effects [10, 11, 13,14,15,16]. Each employing a genome-wide association study (GWAS) approach, the Taiwan Bipolar Consortium found SNPs in the introns of GADL1 associated with lithium treatment response [17], whereas the International Consortium on Lithium Genetics (ConLi+Gen) identified a locus on chromosome 21 [10], and a follow-up analysis uncovered additional variants within the human leukocyte antigen (HLA) region [14, 16]. Gene expression analysis of ConLi+Gen data also showed overexpression of genes involved in mitochondrial functioning in lithium responder patients, highlighting the electron transport chain as a potential target of lithium [18].
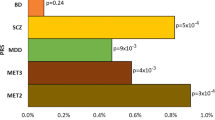
In our recent work, we applied a polygenic score (PGS) modeling approach and demonstrated associations between a poor response to lithium and a high genetic loading for schizophrenia (SCZ) [14], major depression (MD) [13], or a meta-PGS combining both SCZ and MD [15]. Machine-learning models that combined clinical variables with the PGS of SCZ and MD has further improved the prediction of lithium treatment response, explaining 13.7% of the variance [19].
Based on these previous results, translation of PGS testing into clinical practice requires the consideration of three important learnings. First, the PGS of a single phenotype (e.g., SCZ or MD) explains only a small proportion (<2%) of the variability to treatment response in patients with BD [13, 14], providing insufficient power for clinical use. Second, a meta-PGS from multiple related phenotypes has better predictive power than a PGS from a single phenotype [15], suggesting the need to explore additional biological markers, including additional PGSs, that can either independently or together with existing PGSs better predict lithium treatment response. Third, developing polygenic markers with direct pharmacogenomic implications is essential, for example, a PGS for lithium treatment response (Li+PGS), which is perhaps biologically more related to lithium’s pharmacological actions than PGSs built for other clinical phenotypes (i.e., SCZ or MD; that may indirectly influence treatment response or symptom severity, but do not index pharmacogenetic signatures per se).
Here, we developed a novel Li+PGS for lithium treatment response and applied gene-based pathway analyses to identify molecular mechanisms impacted by genetic variation in response phenotypes. Findings may assist in optimizing and personalizing the selection of mood stabilizers in patients with BD, and may point to novel molecular targets for future drug development.
Methods and materials
Study samples
For this study, we obtained genetic and clinical data from the International Consortium on Lithium Genetics (ConLi+Gen: N = 2367), Pathomechanisms and Signature in the Longitudinal Course of Psychosis study (PsyCourse: N = 89), and BipoLife cohort (N = 102). Figure 1 shows the detailed steps of data analysis.

ConLi+Gen = The International Consortium on Lithium Genetics, ALDA = Retrospective Criteria of Long-Term Treatment Response in Research Subjects with Bipolar Disorder scale, HRC = Haplotype Reference Consortium, SNPs = Single Nucleotide Polymorphisms, MAF=Minor Allele Frequency, GWAS = Genome Wide Association analysis, Li+PGS = Polygenic score for lithium treatment response, LOG = Leave-one-group out procedure; PsyCourse = Pathomechanisms and Signature in the Longitudinal Course of Psychosis study and BipoLife = German research consortium for the study of bipolar disorder.
Discovery cohort
ConLi+Gen is a global collaboration of scientists established to study the pharmacogenomics of lithium treatment in patients with BD [10]. In the current study, we analyzed the genome-wide genotype and clinical data of 2367 lithium-treated bipolar patients of European ancestry collected by 22 participating sites in 13 countries, including Australia (n = 122), Austria (n = 43), Czech Republic (n = 45), France (n = 210), Germany (n = 218), Italy (n = 255), Poland (n = 97), Romania (n = 152), Spain (n = 74), Sweden (n = 304), Switzerland (n = 57), Canada (n = 353) and the USA (n = 437) [10, 20].
Replication cohort
To replicate Li+PGS associations found in the discovery ConLi+Gen sample, we utilized datasets from PsyCourse and BipoLife where the study participants were of European ancestry. PsyCourse is a longitudinal multicenter study conducted from 2012 to 2019 in Germany and Austria, with up to four assessments at 6 monthly intervals. The study comprises 1320 patients from psychotic-to-affective spectrum, of which, datasets from 89 patients with BD who received lithium treatment were obtained for this study [21]. BipoLife is a multicenter cohort study, established to investigate the biological basis of BD and patients’ response to treatment and being conducted across ten university hospitals in Germany (Berlin, Bochum, Dresden, Frankfurt, Göttingen, Hamburg, Heidelberg, Marburg, Munich and Tübingen) and the medical informatics section of the University of Göttingen [22].
Target outcome
In both discovery and replication cohorts, patient’s treatment response was assessed using the “Retrospective Criteria of Long-Term Treatment Response in Research Subjects with Bipolar Disorder” scale, also called the ALDA scale [10]. The target outcome “lithium treatment response” was defined in categorical and continuous scales among patients who had received lithium for a minimum of 6 months [10]. In both the discovery ConLi+Gen cohort and the replication cohorts (PsyCourse and BipoLife), a minimum of 6 months of lithium treatment follow-up was implemented as an inclusion criterion. This duration was chosen based on previous analyses of clinical trials, which established that a 6-month follow-up period is appropriate for assessing the minimum efficacy of lithium in patients with bipolar disorder [23]. Furthermore, clinical guidelines highly recommended to regularly monitor lithium levels during the initial six months of treatment, as this period is characterized by potential variability in lithium concentrations and an increased likelihood of side effects. After the six-month mark, stable lithium concentrations are typically achieved, allowing for an evaluation of the risk of toxicity and patients’ adherence to treatment. These factors ultimately influence the effectiveness of the treatment [24,25,26]. The detailed procedures of ALDA scale measurement and its validity are described elsewhere [13, 14, 20]. Briefly, the ALDA scale consists of two subscales: the A scale and the B scale. The A scale measures the response to lithium treatment on a continuum ranging from 0 to 10. Assessors evaluate the change in illness activity while the patient is receiving lithium, and the response is rated accordingly. The anchor points for the A scale range from no change or worsening (score = 0) to complete response, which includes no recurrences during adequate treatment, no residual symptoms, and full functional recovery (score = 10). On the other hand, the B scale describes five factors that could potentially confound the response to lithium treatment or the interpretation of its magnitude. These factors are the number and frequency of episodes before starting lithium (B1 and B2, respectively), the duration of lithium treatment (B3), adherence to the prescribed lithium regimen (B4), and the use of additional medications (B5). Each item on the B scale is rated on a scale of 0 to 2, with a higher B score indicating a lower level of confidence that any observed clinical improvement is solely due to lithium [27]. Once we calculated the total score as ‘A-score minus B-score and setting negative scores to zero’, the categorical (good versus poor) lithium treatment response was defined at a cut-off score of 7, where patients with a total score of 7 or higher were considered as “responders” [10]. The continuous outcome for lithium treatment response was defined on subscale-A, but patients with a total B score greater than 4 or who had missing data on the totals of ALDA subscale-A or B were excluded [10].
Genotyping, quality control and imputation
We obtained the genotype data assayed with different types of commercial SNP arrays across multiple cohorts [10, 21, 22] and applied a series of quality control (QC) procedures before and after imputation using PLINK [28]. First, SNPs that had a poor genotyping rate (<95%), strand ambiguity (A/T and C/G SNPs), a minor allele frequency (MAF) less than 1% or showed deviation from Hardy-Weinberg Equilibrium (P < 10−6) were removed. Then, individuals with low genotype rates (<95%), who had sex inconsistencies (between the documented and genotype-derived sex), and who were genetically related were excluded.
Imputation
The genotype data passing QC were imputed on the Michigan server [24, 29] (https://imputationserver.sph.umich.edu) separately for each genotyping platform, using the Haplotype Reference Consortium (HRC) reference panel that consists of the largest available set (64,976 human haplotypes) of broadly European haplotypes at 39,235,157 SNPs [30]. For each cohort, imputation quality procedures were implemented to exclude SNPs of low-frequency (MAF < 10%) and low-quality (imputation quality score R-square < 0.6). From the imputed dosage score, genotype calls for the filtered SNPs were derived and common sets of 4,652,947 SNPs across the cohorts were merged using PLINK [28].
Statistical analysis
We implemented polygenic score modeling, genome-wide SNP association, gene-based and functional analysis as described below.
Genome-wide SNP association analysis
Genome-wide SNP association analyses were performed on the binary lithium treatment response and continuous ALDA total score using logistic and linear regression models as implemented in PLINK software [28], respectively. Each analysis was adjusted for the covariates: age, sex, chip type and the first four genetic principal components (PCs). After careful examination of the Multidimensional (MD) plot, we observed that the first four PCs successfully captured and delineated any underlying population structure that could potentially influence the genetic association analyses. Consequently, these four PCs were incorporated as covariates in all association analyses. This approach aligns with the methodology employed by previous researchers who utilized the same dataset [10].
Polygenic score development
Using a polygenic score model constructed via Bayesian regression framework and continuous shrinkage (CS) prior on SNP effect sizes implemented in the PRS-CS software [31], we built Li+PGS for individuals of European descent who participated in the ConLi+Gen study and replicated the findings in the combined PsyCourse and BipoLife datasets. Polygenic scores were computed using PRS-CS to infer posterior SNP effect sizes under continuous shrinkage (CS) using GWAS summary statistics and an external linkage disequilibrium (LD) reference panel. For the current analysis, the precomputed LD pattern of the 1000 Genomes European reference panel [32] and the discovery GWAS summary statistics were used to calculate PGS scores.
For the ConLi+Gen study, Li+PGS was derived only for the European ancestry individuals (n = 2367) using a five-fold leave-one-group out (LOG) procedure [33] to remove discovery-target circularity. In each fold, 80% of the sample (n = 1893) was used to generate GWAS summary statistics that were used as discovery for PGS calculation in the 20% left-out target sample (n = 474). The procedure was repeated five times by selecting a non-overlapping set of 20% left-out samples to calculate PGS for the entire cohort. Finally, Li+PGS was computed for the PsyCourse and BipoLife participants using ConLi+Gen’s GWAS summary statistics (discovery sample) generated from the full European cohort (n = 2367).
Polygenic score association analysis
To assess the association of Li+PGS with lithium treatment response, a binary logistic regression model was applied for the binary outcome (good versus poor response to lithium treatment), and a Tobit analysis model (censored regression) was used for the continuous outcome (ALDA total) [34]. In addition, we divided the ConLi+Gen sample into deciles, ranging from the lowest polygenic load (1st decile, reference group) to the highest polygenic load (10th decile). Then, we compared BD patients in the higher polygenic load deciles (2nd–10th deciles) with patients in the lowest polygenic load decile (1st decile). In both the binary and continuous outcomes, the proportion of phenotypic variance explained by Li+PGS was computed as the difference in R2 of the model fit with Li+PGS plus covariates, compared to the model fit with only covariates. Each modeling analysis was adjusted for the covariates: age, sex, and the first four genetic PCs, and statistical significance was set at p < 0.05.
Gene-based and functional analysis
The gene-based analysis was based on summary statistics generated through genome-wide SNP association analysis of the full European ConLi+Gen sample (n = 2367) and employed MAGMA (Multi-marker Analysis of GenoMic Annotation) [35], a tool that uses a multiple regression approach to incorporate LD between markers and to detect multi-marker effects.
To explore the biological context of the genes discovered from the gene-based analysis, a pathway analysis was implemented using PANTHER (Protein ANalysis THrough Evolutionary Relationships; http://pantherdb.org/) classification system. PANTHER is designed to classify proteins (and their genes) into biological pathways [36]. To prepare the input genes for PANTHER, we selected genes that showed gene-level association with lithium treatment response (either with the categorical or continuous outcome) at MAGMA adjusted p-value < 0.001. This list of genes was entered into PANTHER version-17 which compares the proportion of input genes mapping to a biological pathway to the reference gene list from its databases. Molecular relationships previously experimentally observed in Homo sapiens (human) were included. The significance of the overrepresented PANTHER pathways was determined using Fisher’s exact test and later adjusted for multiple testing using the Bonferroni correction method. Significant associations were defined at p-value < 0.05.
Results
Sample characteristics
The discovery analysis consisted of ConLi+Gen data obtained from 2,367 bipolar patients of European ancestry who had undergone lithium treatment for at least six months. The mean (sd) age of the patients was 47.5(13.9) years and 1,369 (57.8%) were female. In all, 660 (27.9%) of patients had a good response to lithium treatment (ALDA score ≥7). The mean (sd) ALDA score for ConLi+Gen participants was 4.1 (3.1). Among 2362 patients who underwent assessment for the type of bipolar diagnosis, the majority (80.0%) were diagnosed with type 1 bipolar disorder. These patients also presented with comorbid conditions such as psychosis, alcohol dependence, panic disorder, and obsessive-compulsive disorder. Of the 438 patients assessed for possible side effects related to lithium treatment, 153(34.9%) of them reported experiencing at least one of the following: nausea, vertigo, polyuria, diarrhea, hypothyroidism, loss of libido, EEG abnormalities, increased thirst, dermal problems, weight gain, and strangury. The replication analysis was based on a combination of the PsyCourse and BipoLife datasets (N = 191), whose mean (sd) age was 49.1(13.0) years. Of the 191 patients with BD, 48(25.1%) had a good response to lithium. This replication cohort exhibits similar characteristics to the discovery sample in terms of the type of bipolar disorder, comorbidities, and patients’ reports of lithium treatment side effects (Table 1).
Associations of Li+ PGS with lithium treatment response in bipolar patients
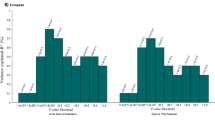
Using ConLi+Gen data, we found statistically significant associations between Li+PGS and lithium treatment response — both in the categorical (P = 9.8 × 10−12, R2 = 1.9%) and continuous (P = 6.4 × 10−9, R2 = 2.6%) outcomes. Li+PGS was positively associated with response to lithium treatment, with an adjusted odds ratio (OR) [95%CI]) of 1.39 [1.26, 1.54]. In other words, BD patients who carry a higher genetic loading for lithium responsive genetic variants, measured using the Li+PGS, have higher odds of favorable lithium treatment response, compared to patients carrying a low Li+PGS load. Table 2 shows the association results of Li+PGS and lithium treatment response in categorical and continuous outcomes. The odds of a favorable treatment response increased as the Li+PGS increased, ranging from 1.59 fold [95%CI: 1.02–2.49] at the 2nd decile to 3.47 fold [95%CI: 2.22–5.47] at 10th decile, compared to the reference Li+PGS at the 1st decile (Table 2). While there was an increasing trend in the odds of lithium treatment response across the deciles, the most significant prediction contrast was found at the ‘extremes’ (1st and 10th decile) which comprised of ~20% of the total cohort (Fig. 2). A replication PGS analysis in the combined PsyCourse and BipoLife samples found a statistically significant association of Li+PGS with the categorical lithium treatment response (P = 3.9 × 10−4, R2 = 0.9%), but not with the continuous outcome (P = 0.13).

The X mark on the line plot indicates that the association is not statistically significant at that decile. OR Odds ratio, CI Confidence interval, Li+PGS Polygenic score for lithium treatment response.
Genome-wide association, gene-based and functional analysis
After re-imputing the ConLi+Gen data in reference to the latest HRC genomes, we conducted GWASs on lithium response, both in categorical and continuous outcomes. This GWAS analysis identified a single locus with lead SNP rs9396756 located near the stathmin domain containing 1 (STMND1) gene that reached genome-wide significance for association with the categorical outcome (P = 2.7 × 10−8) and showed a suggestive association with the continuous ALDA score (P = 7.6 × 10−8) (Fig. 3). A follow-up gene-based analysis of the newly derived ConLi+Gen GWAS summary statistics found 36 candidate genes likely associated with lithium treatment response — assessed in either continuous or categorical outcomes (P < 0.001). In silico functional analysis of the 36 genes revealed enriched biological pathways including the muscarinic acetylcholine receptors 1 and 3 (P-value corrected for multiple testing = 0.026) and metabotropic glutamate receptor group III pathway (P = 0.043). These genes and pathways may have an impact on clinical response to lithium treatment and be potential molecular targets for lithium (Supplementary Figure 1 and Table 1).

A In the categorical outcome and (B) continuous scale, highlighting the loci that showed genome-wide significance (orange).The −log10 (p-value) is plotted against the physical position of each SNP on each chromosome. The threshold for genome-wide significance (p-value < 5 × 10–8) is indicated by the red dotted horizontal line.
Discussion
This study presents findings from a comprehensive analysis of genetic and clinical data on lithium treatment response that involved the development of a polygenic score for lithium treatment response (Li+PGS), genome-wide SNP association and gene-based and functional analyses.
Since the publication of the first GWAS report by the ConLi+Gen team [10], two landmark studies that independently showed the negative association of PGSs for SCZ and MD with lithium treatment response have been published [13,14,15]. The first study found that 10% of bipolar patients with the lowest polygenic load for SCZ were 3.46 times more responsive to lithium compared to 10% of patients with the highest genetic load for SCZ [14, 15]. Similarly, in the second study, 10% of patients who had the lowest genetic loading for MD were 1.54 times more responsive to lithium than 10% of patients with the highest genetic loading for MD [13, 15]. Nevertheless, each of these PGSs accounts for <2% of the total variance to lithium treatment response [13], suggesting the need to explore additional biological traits that can either independently, or in concert with existing PGSs better predict lithium response. Moreover, the previous PGSs for SCZ and MD are difficult to interpret in a pharmacogenomic context, making the development of a specific lithium response PGS necessary, which is assumed to be more likely to be associated with lithium treatment response and perhaps is biologically more related to lithium’s pharmacological actions.
In this novel study, we constructed a PGS for lithium response-Li+PGS, a biological marker of direct pharmacogenomic relevance, and showed a positive relationship between a high genetic loading for lithium treatment response variants and long-term therapeutic response to lithium in patients with BD. We demonstrated that bipolar patients at the extreme tail end of the distribution have the strongest association, i.e. 10% of patients who carry high genetic loading for lithium responsive variants (10th decile) were 3.47 times more likely to respond to lithium compared to 10% of those with the lowest Li+PGS (1st decile). These results indicated that Li+PGS has the potential to help stratify bipolar patients according to predicted lithium response.
In a GWAS of lithium treatment response, we identified a locus near the STMND1 gene, which encodes for proteins known to be involved in neuron projection development, and active in neuron junctions and cytoplasm. Previous analysis that employed the 1000 Genomes Project reference panel for imputation reported a suggestive association between genetic variants within the STMND1 gene and lithium treatment response [10].
Using our newly derived ConLi+Gen GWASs summary statistics as an input, we then carried out a gene-based analysis where several genetic variations were examined together for their association with lithium treatment response [35]. This approach found 36 potential target genes for lithium treatment that are enriched in the muscarinic acetylcholine receptors (mAChRs) 1 and 3 and the metabotropic glutamate receptor group III signaling pathways — well characterized biological pathways modulated by the most abundant neurotransmitters in the brain (glutamate and acetylcholine).
Acetylcholine is the central regulator of the mAChRs signaling pathways, which are subfamily of G protein-coupled receptor complexes located in the cell membranes of neurons and other cells that regulate fundamental functions of the central and peripheral nervous system including acting as the main end-receptor stimulated by acetylcholine released from postganglionic fibers in the parasympathetic nervous system [37]. The muscarinic antagonist scopolamine has antidepressant activity, while physostigmine, a cholinesterase inhibitor induces depressive symptoms, suggesting muscarinic receptors may play a role, not only in the pathogenesis of mood disorders, but also as therapeutic targets [38]. M1 and 3 receptors are localized in the cortex, hippocampus and substantia nigra and are known to activate protein kinase C (PKC), causing post-synaptic excitation. PKC is thought to be central in the molecular pathogenesis of BD.
Glutamate, the primary excitatory neurotransmitter in the central nervous system (CNS), exerts neuromodulatory actions via the activation of metabotropic glutamate (mGlu), a type of glutamate receptor that modulates synaptic transmission and neuronal excitability throughout the central nervous system [39]. Group III metabotropic glutamate receptors are largely presynaptically localized and downregulate neurotransmitter release from presynaptic terminals directly or indirectly. These receptors have a prominent expression in the brain, especially in the region of the hippocampus, and can lead to the inhibition of the cAMP cascade which is critical for the maintenance of long-term synaptic plasticity [40]. Growing evidence indicates that abnormalities in the glutamatergic system are implicated in the pathogenesis and treatment of mental health disorders [41] including BD [42, 43], SCZ [44], neurodevelopmental disorders [45], Huntington’s disease [46] and Alzheimer’s disease [47]. Studies have reported SNPs of the mGluRs system associated with BD [48], and in animal studies, lithium was found to alter intracellular calcium by modulating the activity of the metabotropic glutamatergic receptor system [49]. To summarise, findings from the genome-wide SNP association, gene-based and functional analysis highlight the possibility that mechanisms involving glutamate and acetylcholine signaling pathways might influence the therapeutic effects of lithium in patients with BD. Modulation of these pathways through genetic variants may disrupt or enhance lithium’s clinical effectiveness.
Our study has some limitations. First, while our findings were replicated in an independent small size sample, the fact that it was replicated in the binary outcome, but not in the continuous outcome indicates the need for a larger replication cohort. Second, because Li+PGS was developed and evaluated in European-ancestry populations, the findings should be replicated in a multi-ethnic population to gauge generalizability. Furthermore, the risks and benefits of predictive models consisting of Li+PGS should be evaluated in prospective studies. Third, Li+PGS only explains about 2% of response variance in our cohort, and as such is comparable to PGSs from other phenotypes (SCZ, MDD) that have shown an association with treatment outcomes. On their own, these PGSs are not suited to clinical pharmacogenomic testing as they would not predict treatment response prospectively in individual patients. Prediction models combining Li+PGS with other PGSs [13, 14] and clinical characteristics [19] may improve the clinical utility of PGSs. Such models would then need to be tested in prospective studies and clinical trials. Forth, studies have shown that approaches to phenotyping of lithium treatment response can be improved using advanced methods such as machine learning [19]. Employing a more precise phenotype definition may result in the identification of novel candidate genes implicated in lithium treatment response and ultimately the development of more informative Li+PGS. Fifth, the current analysis did not include important covariates such as medication dose, information on lithium blood levels, side effects, and the use of concomitant medications (such as Angiotensin-converting enzyme (ACE) inhibitors, diuretics, Non-steroidal anti-inflammatory drugs (NSAIDs)), which can potentially influence lithium clearance and treatment response [50]. Moreover, maintaining therapeutic blood levels is crucial to achieving treatment response with limited side effects in lithium therapy [50]. Lithium possesses a narrow therapeutic index, meaning that there is a relatively small margin between an effective dose and a potentially toxic one. Typically, lithium levels are initially monitored more frequently (weekly or biweekly) during the initiation or adjustment phase of medication, and then less frequently (every 3 to 6 months) once stable therapeutic levels are achieved. While the duration of lithium treatment and the use of certain psychiatric medications (antidepressants, antipsychotics, mood stabilizers) were assessed as part of the B scale measure of ALDA score, information on the specific dosage, medication blood level and the use of concomitant medications were not available in the ConLi+Gen dataset, and thus, they were not considered in our analyses. The inclusion of these pharmacogenomic covariates could provide stronger evidence and should be considered in future research.
In conclusion, we developed a unique lithium treatment response polygenic score (Li+PGS) that showed a positive association with better lithium treatment response in patients with BD. Our gene-based and functional analyses build upon the findings from existing molecular studies by linking lithium treatment response with muscarinic acetylcholine receptor signaling and metabotropic glutamate receptor pathways. Further pharmacological evaluation of these pathways in the context of BD and mood stabilizing treatments may prove fruitful.
References
Grande I, Berk M, Birmaher B, Vieta E. Bipolar disorder. Lancet. 2016;387:1561–72.
DALYs GBD, Collaborators H. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1859–922.
Walker S, Mackay E, Barnett P, Sheridan Rains L, Leverton M, Dalton-Locke C, et al. Clinical and social factors associated with increased risk for involuntary psychiatric hospitalisation: a systematic review, meta-analysis, and narrative synthesis. Lancet Psychiatry. 2019;6:1039–53.
Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: a meta-review. World Psychiatry. 2014;13:153–60.
Cade JF. Lithium salts in the treatment of psychotic excitement. Med J Aust. 1949;2:349–52.
Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust NZ J Psychiatry. 2021;55:7–117.
Goodwin GM, Haddad PM, Ferrier IN, Aronson JK, Barnes T, Cipriani A, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology. J Psychopharmacol (Oxf, Engl). 2016;30:495–553.
Garnham J, Munro A, Slaney C, Macdougall M, Passmore M, Duffy A, et al. Prophylactic treatment response in bipolar disorder: results of a naturalistic observation study. J Affect Disord. 2007;104:185–90.
Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ (Clin Res ed). 2013;346:f3646.
Hou L, Heilbronner U, Degenhardt F, Adli M, Akiyama K, Akula N, et al. Genetic variants associated with response to lithium treatment in bipolar disorder: a genome-wide association study. Lancet. 2016;387:1085–93.
Amare AT, Schubert KO, Baune BT. Pharmacogenomics in the treatment of mood disorders: Strategies and opportunities for personalized psychiatry. EPMA J. 2017;8:211–27.
Grof P, Duffy A, Cavazzoni P, Grof E, Garnham J, MacDougall M, et al. Is response to prophylactic lithium a familial trait? J Clin psychiatry. 2002;63:942–7.
Amare AT, Schubert KO, Hou L, Clark SR, Papiol S, Cearns M, et al. Association of polygenic score for major depression with response to lithium in patients with bipolar disorder. Mol Psychiatry. 2021;26:2457–70.
International Consortium on Lithium G, Amare AT, Schubert KO, Hou L, Clark SR, Papiol S, et al. Association of polygenic score for schizophrenia and HLA Antigen and inflammation genes with response to lithium in bipolar affective disorder: A genome-wide association study. JAMA Psychiatry. 2018;75:65–74.
Schubert KO, Thalamuthu A, Amare AT, Frank J, Streit F, Adl M, et al. Combining schizophrenia and depression polygenic risk scores improves the genetic prediction of lithium response in bipolar disorder patients. Transl Psychiatry. 2021;11:606.
Le Clerc S, Lombardi L, Baune BT, Amare AT, Schubert KO, Hou L, et al. HLA-DRB1 and HLA-DQB1 genetic diversity modulates response to lithium in bipolar affective disorders. Sci Rep. 2021;11:17823.
Chen CH, Lee CS, Lee MT, Ouyang WC, Chen CC, Chong MY, et al. Variant GADL1 and response to lithium therapy in bipolar I disorder. N. Engl J Med. 2014;370:119–28.
Stacey D, Schubert KO, Clark SR, Amare AT, Milanesi E, Maj C, et al. A gene co-expression module implicating the mitochondrial electron transport chain is associated with long-term response to lithium treatment in bipolar affective disorder. Transl Psychiatry. 2018;8:183.
Cearns M, Amare AT, Schubert KO, Thalamuthu A, Frank J, Streit F, et al. Using polygenic scores and clinical data for bipolar disorder patient stratification and lithium response prediction: machine learning approach. Br J Psychiatry. 2022;220:219–28.
Manchia M, Adli M, Akula N, Ardau R, Aubry JM, Backlund L, et al. Assessment of response to lithium maintenance treatment in bipolar disorder: A consortium on Lithium Genetics (ConLiGen) Report. PLoS One. 2013;8:e65636.
Dwyer DB, Kalman JL, Budde M, Kambeitz J, Ruef A, Antonucci LA, et al. An Investigation of Psychosis Subgroups With Prognostic Validation and Exploration of Genetic Underpinnings: The PsyCourse Study. JAMA Psychiatry. 2020;77:523–33.
Ritter PS, Bermpohl F, Gruber O, Hautzinger M, Jansen A, Juckel G, et al. Aims and structure of the German research consortium bipolife for the study of bipolar disorder. Int J Bipolar Disord. 2016;4:26.
Nierenberg AA, McElroy SL, Friedman ES, Ketter TA, Shelton RC, Deckersbach T, et al. Bipolar CHOICE (Clinical Health Outcomes Initiative in Comparative Effectiveness): a pragmatic 6-month trial of lithium versus quetiapine for bipolar disorder. J Clin Psychiatry. 2016;77:90–9.
McKnight RF, Adida M, Budge K, Stockton S, Goodwin GM, Geddes JR. Lithium toxicity profile: A systematic review and meta-analysis. Lancet. 2012;379:721–8.
Malhi GS, Tanious M, Das P, Berk M. The science and practice of lithium therapy. Aust NZ J Psychiatry. 2012;46:192–211.
Ng F, Mammen OK, Wilting I, Sachs GS, Ferrier IN, Cassidy F, et al. The International Society for Bipolar Disorders (ISBD) consensus guidelines for the safety monitoring of bipolar disorder treatments. Bipolar Disord. 2009;11:559–95.
Scott J, Etain B, Manchia M, Brichant-Petitjean C, Geoffroy PA, Schulze T, et al. An examination of the quality and performance of the Alda scale for classifying lithium response phenotypes. Bipolar Disord. 2020;22:255–65.
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA, Bender D, et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81:559–75.
Das S, Forer L, Schonherr S, Sidore C, Locke AE, Kwong A, et al. Next-generation genotype imputation service and methods. Nat Genet. 2016;48:1284–7.
McCarthy S, Das S, Kretzschmar W, Delaneau O, Wood AR, Teumer A, et al. A reference panel of 64,976 haplotypes for genotype imputation. Nat Genet. 2016;48:1279–83.
Ge T, Chen CY, Ni Y, Feng YA, Smoller JW. Polygenic prediction via Bayesian regression and continuous shrinkage priors. Nat Commun. 2019;10:1776.
Southam L, Gilly A, Suveges D, Farmaki AE, Schwartzentruber J, Tachmazidou I, et al. Whole genome sequencing and imputation in isolated populations identify genetic associations with medically-relevant complex traits. Nat Commun. 2017;8:15606.
Sakaue S, Kanai M, Karjalainen J, Akiyama M, Kurki M, Matoba N, et al. Trans-biobank analysis with 676,000 individuals elucidates the association of polygenic risk scores of complex traits with human lifespan. Nat Med. 2020;26:542–8.
Yee TW. The VGAM package for categorical data analysis. J Stat Softw. 2010;32:1–34.
de Leeuw CA, Mooij JM, Heskes T, Posthuma D. MAGMA: Generalized gene-set analysis of GWAS data. PLoS Comput Biol. 2015;11:e1004219.
Thomas PD, Campbell MJ, Kejariwal A, Mi H, Karlak B, Daverman R, et al. PANTHER: A library of protein families and subfamilies indexed by function. Genome Res. 2003;13:2129–41.
Kruse AC, Kobilka BK, Gautam D, Sexton PM, Christopoulos A, Wess J. Muscarinic acetylcholine receptors: Novel opportunities for drug development. Nat Rev Drug Discov. 2014;13:549–60.
Bymaster FP, Felder CC. Role of the cholinergic muscarinic system in bipolar disorder and related mechanism of action of antipsychotic agents. Mol Psychiatry. 2002;7:S57–63.
Niswender CM, Conn PJ. Metabotropic glutamate receptors: Physiology, pharmacology, and disease. Annu Rev Pharm Toxicol. 2010;50:295–322.
Mercier MS, Lodge D. Group III metabotropic glutamate receptors: Pharmacology, physiology and therapeutic potential. Neurochem Res. 2014;39:1876–94.
Sanacora G, Zarate CA, Krystal JH, Manji HK. Targeting the glutamatergic system to develop novel, improved therapeutics for mood disorders. Nat Rev Drug Discov. 2008;7:426–37.
Matosin N, Fernandez-Enright F, Frank E, Deng C, Wong J, Huang XF, et al. Metabotropic glutamate receptor mGluR2/3 and mGluR5 binding in the anterior cingulate cortex in psychotic and nonpsychotic depression, bipolar disorder and schizophrenia: implications for novel mGluR-based therapeutics. J Psychiatry Neurosci. 2014;39:407–16.
Itokawa M, Yamada K, Iwayama-Shigeno Y, Ishitsuka Y, Detera-Wadleigh S, Yoshikawa T. Genetic analysis of a functional GRIN2A promoter (GT)n repeat in bipolar disorder pedigrees in humans. Neurosci Lett. 2003;345:53–56.
Tang J, Chen X, Xu X, Wu R, Zhao J, Hu Z, et al. Significant linkage and association between a functional (GT)n polymorphism in promoter of the N-methyl-D-aspartate receptor subunit gene (GRIN2A) and schizophrenia. Neurosci Lett. 2006;409:80–2.
Endele S, Rosenberger G, Geider K, Popp B, Tamer C, Stefanova I, et al. Mutations in GRIN2A and GRIN2B encoding regulatory subunits of NMDA receptors cause variable neurodevelopmental phenotypes. Nat Genet. 2010;42:1021–6.
Arning L, Kraus PH, Valentin S, Saft C, Andrich J, Epplen JT. NR2A and NR2B receptor gene variations modify age at onset in Huntington disease. Neurogenetics. 2005;6:25–8.
Leuba G, Vernay A, Kraftsik R, Tardif E, Riederer BM, Savioz A. Pathological reorganization of NMDA receptors subunits and postsynaptic protein PSD-95 distribution in Alzheimer’s disease. Curr Alzheimer Res. 2014;11:86–96.
Blacker CJ, Lewis CP, Frye MA, Veldic M. Metabotropic glutamate receptors as emerging research targets in bipolar disorder. Psychiatry Res. 2017;257:327–37.
Khayachi A, Ase A, Liao C, Kamesh A, Kuhlmann N, Schorova L, et al. Chronic lithium treatment alters the excitatory/ inhibitory balance of synaptic networks and reduces mGluR5-PKC signalling in mouse cortical neurons. J Psychiatry Neurosci. 2021;46:E402–14.
Malhi GS, Bell E, Outhred T, Berk M. Lithium therapy and its interactions. Aust Prescr. 2020;43:91–3.
Acknowledgements
The authors are grateful to all patients who participated in the study and we appreciate the contributions of clinicians, scientists, research assistants and study staff who helped in the patient recruitment, data collection and biological sample preparation of the studies. We are also indebted to the members of the ConLi+Gen Scientific Advisory Board (http://www.conligen.org/) for critical input over the course of the project. The analysis of this study was carried out using the high-performance computational (HPC) capabilities of the University of Adelaide’s Phoenix Supercomputer https://www.adelaide.edu.au/phoenix/.
Funding
AT Amare received the 2019–2021 National Alliance for Research on Schizophrenia and Depression (NARSAD) Young Investigator Grant from the Brain & Behaviour Research Foundation (BBRF) and is currently supported by National Health and Medical Research Council (NHMRC) Emerging Leadership (EL1) Investigator Grant (APP2008000). The primary sources of funding were the Deutsche Forschungsgemeinschaft (DFG; grant no.RI 908/7-1; grant FOR2107, RI 908/11-1 to Marcella Rietschel, NO 246/10-1 to Markus M. Nöthen) and the Intramural Research Program of the National Institute of Mental Health (ZIA-MH00284311; ClinicalTrials.gov identifier: NCT00001174). The genotyping was in part funded by the German Federal Ministry of Education and Research (BMBF) through the Integrated Network IntegraMent (Integrated Understanding of Causes and Mechanisms in Mental Disorders), under the auspices of the e:Med Programme (grants awarded to Thomas G. Schulze, Marcella Rietschel, and Markus M. Nöthen). Improving Recognition and Care in Critical Areas of Bipolar Disorders (BipoLife) study was funded by Bundesministerium für Bildung und Forschung (BMBF): PIs – Felix Bermpohl, Philipp Ritter, Michael Bauer, Andreas Reif, Sarah Kittel-Schneider, Thomas G. Schulze, Jens Wiltfang, Georg Juckel, Andreas Fallgatter and Martin Lambert. Urs Heilbronner was supported by European Union’s Horizon 2020 Research and Innovation Programme (PSY-PGx, grant agreement No 945151). Some data and biomaterials were collected as part of eleven projects (Study 40) that participated in the National Institute of Mental Health (NIMH) Bipolar Disorder Genetics Initiative. From 2003–2007, the Principal Investigators and Co-Investigators were: Indiana University, Indianapolis, IN, R01 MH59545, John Nurnberger, M.D., Ph.D., Marvin J. Miller, M.D., Elizabeth S. Bowman, M.D., N. Leela Rau, M.D., P.Ryan Moe, M.D., Nalini Samavedy, M.D., Rif El-Mallakh, M.D. (at University of Louisville), Husseini Manji, M.D.(at Johnson and Johnson), Debra A.Glitz, M.D.(at Wayne State University), Eric T.Meyer, Ph.D., M.S.(at Oxford University, UK), Carrie Smiley, R.N., Tatiana Foroud, Ph.D., Leah Flury, M.S., Danielle M.Dick, Ph.D (at Virginia Commonwealth University), Howard Edenberg, Ph.D.; Washington University, St. Louis, MO, R01 MH059534, John Rice, Ph.D, Theodore Reich, M.D., Allison Goate, Ph.D., Laura Bierut, M.D.K02 DA21237; Johns Hopkins University, Baltimore, M.D., R01 MH59533, Melvin McInnis, M.D., J.Raymond DePaulo, Jr., M.D., Dean F. MacKinnon, M.D., Francis M. Mondimore, M.D., James B. Potash, M.D., Peter P. Zandi, Ph.D, Dimitrios Avramopoulos, and Jennifer Payne; University of Pennsylvania, PA, R01 MH59553, Wade Berrettini, M.D., Ph.D.; University of California at San Francisco, CA, R01 MH60068, William Byerley, M.D., and Sophia Vinogradov, M.D.; University of Iowa, IA, R01 MH059548, William Coryell, M.D., and Raymond Crowe, M.D.; University of Chicago, IL, R01 MH59535, Elliot Gershon, M.D., Judith Badner, Ph.D., Francis McMahon, M.D., Chunyu Liu, Ph.D., Alan Sanders, M.D., Maria Caserta, Steven Dinwiddie, M.D., Tu Nguyen, Donna Harakal; University of California at San Diego, CA, R01 MH59567, John Kelsoe, M.D., Rebecca McKinney, B.A.; Rush University, IL, R01 MH059556, William Scheftner, M.D., Howard M. Kravitz, D.O., M.P.H., Diana Marta, B.S., Annette Vaughn-Brown, M.S.N., R.N., and Laurie Bederow, M.A.; NIMH Intramural Research Program, Bethesda, MD, 1Z01MH002810-01, Francis J. McMahon, M.D., Layla Kassem, Psy.D., Sevilla Detera-Wadleigh, Ph.D, Lisa Austin, Ph.D, Dennis L. Murphy, M.D.; Howard University, William B. Lawson, M.D., Ph.D., Evarista Nwulia, M.D., and Maria Hipolito, M.D. This work was supported by the NIH grants P50CA89392 from the National Cancer Institute and 5K02DA021237 from the National Institute of Drug Abuse. The Canadian part of the study was supported by the Canadian Institutes of Health Research grant (#166098), as well as Genome Canada and Research Nova Scotia grants to MA. Collection and phenotyping of the Australian UNSW sample, by Philip B. Mitchell, Peter R. Schofield, Janice M. Fullerton and Adam Wright, was funded by an Australian NHMRC Program Grant (No.1037196). The collection of the Barcelona sample was supported by the Centro de Investigación en Red de Salud Mental (CIBERSAM), IDIBAPS, and the CERCA Programme / Generalitat de Catalunya (grant numbers PI080247, PI1200906, PI12/00018, 2014SGR1636, and 2014SGR398). The Swedish Research Council, the Stockholm County Council, Karolinska Institutet and the Söderström-Königska Foundation supported this research through grants awarded to Lena Backlund, Louise Frise’n, Catharina Lavebratt and Martin Schalling. The collection of the Geneva sample was supported by the Swiss National Foundation (grants Synapsy 51NF40-158776 and 32003B-125469). The collection of the Romanian sample was supported by U.E.F.I.S.C.D.I., Romania, grant awarded to Maria Grigoroiu-Serbanescu. Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
AT Amare conceived and designed the study hypothesis, as well as secured a fellowship to lead the study. AT Amare and A Thalamuthu conducted the statistical analysis and interpreted the findings. AT Amare, A Thalamuthu, and KO Schubert drafted the manuscript. BT Baune and SR Clark provided supervision for the study. All authors contributed genetic and clinical data, and critically revised the manuscript for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
Eduard Vieta has received grants and served as consultant, advisor or CME speaker for the following entities: AB-Biotics, Allergan, Angelini, AstraZeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, Farmindustria, Ferrer, Forest Research Institute, Gedeon Richter, GlaxoSmith-Kline, Janssen, Lundbeck, Otsuka, Pfizer, Roche, Sanofi-Aventis, Servier, Shire, Sunovion, Takeda, the Brain and Behaviour Foundation, the Spanish Ministry of Science and Innovation (CIBERSAM), and the Stanley Medical Research Institute. Michael Bauer has received grants from the Deutsche Forschungsgemeinschaft (DFG), and Bundesministeriums für Bildung und Forschung (BMBF), and served as consultant, advisor or CME speaker for the following entities: Allergan, Aristo, Janssen, Lilly, Lundbeck, neuraxpharm, Otsuka, Sandoz, Servier and Sunovion outside the submitted work. Sarah Kittel-Schneider has received grants and served as consultant, advisor or speaker for the following entities: Medice Arzneimittel Pütter GmbH and Shire/Takeda. Bernhard Baune has received grants and served as consultant, advisor or CME speaker for the following entities: AstraZeneca, Bristol-Myers Squibb, Janssen, Lundbeck, Otsuka, Servier, the National Health and Medical Research Council, the Fay Fuller Foundation, the James and Diana Ramsay Foundation. Scott Clark has received grants and served as consultant, advisor or CME speaker for the following entities: Otsuka Austalia, Lundbeck Australia, Janssen-Cilag Australia, Servier Australia. Tadafumi Kato received honoraria for lectures, manuscripts, and/or consultancy, from Kyowa Hakko Kirin Co, Ltd, Eli Lilly Japan K.K., Otsuka Pharmaceutical Co, Ltd, GlaxoSmithKline K.K., Taisho Toyama Pharmaceutical Co, Ltd, Dainippon Sumitomo Pharma Co, Ltd, Meiji Seika Pharma Co, Ltd, Pfizer Japan Inc., Mochida Pharmaceutical Co, Ltd, Shionogi & Co, Ltd, Janssen Pharmaceutical K.K., Janssen Asia Pacific, Yoshitomiyakuhin, Astellas Pharma Inc, Wako Pure Chemical Industries, Ltd, Wiley Publishing Japan, Nippon Boehringer Ingelheim Co Ltd, Kanae Foundation for the Promotion of Medical Science, MSD K.K., Kyowa Pharmaceutical Industry Co, Ltd and Takeda Pharmaceutical Co, Ltd. Tadafumi Kato also received a research grant from Takeda Pharmaceutical Co, Ltd. Peter Falkai has received grants and served as consultant, advisor or CME speaker for the following entities Abbott, GlaxoSmithKline, Janssen, Essex, Lundbeck, Otsuka, Gedeon Richter, Servier and Takeda as well as the German Ministry of Science and the German Ministry of Health. Eva Reininghaus has received grants and served as consultant, advisor or CME speaker for the following entities: Janssen and Institut Allergosan. Mikael Landén declares that, over the past 36 months, he has received lecture honoraria from Lundbeck and served as a scientific consultant for EPID Research Oy; no other equity ownership, profit-sharing agreements, royalties or patent. Kazufumi Akiyama has received consulting honoraria from Taisho Toyama Pharmaceutical Co, Ltd. In 2021, Jörg Zimmermann served as an advisor for Biogen concerning Aducanumab (Alzheimer’s Disease).The other authors have no other conflict of interest to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Amare, A.T., Thalamuthu, A., Schubert, K.O. et al. Association of polygenic score and the involvement of cholinergic and glutamatergic pathways with lithium treatment response in patients with bipolar disorder. Mol Psychiatry 28, 5251–5261 (2023). https://doi.org/10.1038/s41380-023-02149-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41380-023-02149-1
This article is cited by
-
Effectiveness of ultra-long-term lithium treatment: relevant factors and case series
International Journal of Bipolar Disorders (2024)
-
Lithium response in bipolar disorder is associated with focal adhesion and PI3K-Akt networks: a multi-omics replication study
Translational Psychiatry (2024)
