
Abstract
Glutamatergic dysfunction is implicated in schizophrenia pathoaetiology, but this may vary in extent between patients. It is unclear whether inter-individual variability in glutamate is greater in schizophrenia than the general population. We conducted meta-analyses to assess (1) variability of glutamate measures in patients relative to controls (log coefficient of variation ratio: CVR); (2) standardised mean differences (SMD) using Hedges g; (3) modal distribution of individual-level glutamate data (Hartigan’s unimodality dip test). MEDLINE and EMBASE databases were searched from inception to September 2022 for proton magnetic resonance spectroscopy (1H-MRS) studies reporting glutamate, glutamine or Glx in schizophrenia. 123 studies reporting on 8256 patients and 7532 controls were included. Compared with controls, patients demonstrated greater variability in glutamatergic metabolites in the medial frontal cortex (MFC, glutamate: CVR = 0.15, p < 0.001; glutamine: CVR = 0.15, p = 0.003; Glx: CVR = 0.11, p = 0.002), dorsolateral prefrontal cortex (glutamine: CVR = 0.14, p = 0.05; Glx: CVR = 0.25, p < 0.001) and thalamus (glutamate: CVR = 0.16, p = 0.008; Glx: CVR = 0.19, p = 0.008). Studies in younger, more symptomatic patients were associated with greater variability in the basal ganglia (BG glutamate with age: z = −0.03, p = 0.003, symptoms: z = 0.007, p = 0.02) and temporal lobe (glutamate with age: z = −0.03, p = 0.02), while studies with older, more symptomatic patients associated with greater variability in MFC (glutamate with age: z = 0.01, p = 0.02, glutamine with symptoms: z = 0.01, p = 0.02). For individual patient data, most studies showed a unimodal distribution of glutamatergic metabolites. Meta-analysis of mean differences found lower MFC glutamate (g = −0.15, p = 0.03), higher thalamic glutamine (g = 0.53, p < 0.001) and higher BG Glx in patients relative to controls (g = 0.28, p < 0.001). Proportion of males was negatively associated with MFC glutamate (z = −0.02, p < 0.001) and frontal white matter Glx (z = −0.03, p = 0.02) in patients relative to controls. Patient PANSS total score was positively associated with glutamate SMD in BG (z = 0.01, p = 0.01) and temporal lobe (z = 0.05, p = 0.008). Further research into the mechanisms underlying greater glutamatergic metabolite variability in schizophrenia and their clinical consequences may inform the identification of patient subgroups for future treatment strategies.
Similar content being viewed by others

Introduction
Several lines of evidence implicate glutamatergic dysfunction in the pathoaetiology of schizophrenia [1]. It is not clear, however, whether the degree of glutamatergic dysfunction is similar across individuals with schizophrenia or whether there is significant interindividual variability over and above the variability observed in the general population. Meta-analyses of 1H-MRS studies report higher glutamate and combined glutamate and glutamine (Glx) in the basal ganglia [2, 3], higher glutamine in the thalamus [2, 3] and lower glutamate in the medial frontal cortex (MFC) [3,4,5,6] in schizophrenia in comparison to controls. Two meta-analyses do not report lower glutamate levels in the medial frontal cortex [2, 3] but find lower levels in non treatment-resistant patients [3]. Glutamate levels in schizophrenia show heritability [7], are associated with glutamatergic genetic risk [8] and may also be altered by environmental factors [9]. There is some evidence that glutamate levels are positively associated with the severity of symptoms of schizophrenia [10,11,12,13] and may be reduced by treatment with antipsychotic medication [12, 14]. It is unknown, however, whether these associations are similar across all patients or if they vary between individuals, for example due to differences in underlying neurobiology or illness stage. This could be important if heterogeneity in glutamate measures is related to treatment outcomes in schizophrenia. For example, there is already some evidence that elevated glutamate levels may be most apparent in patients whose symptoms do not respond well to antipsychotic medication [15,16,17,18,19,20,21,22,23,24], and that glutamate-acting compounds could have selective efficacy in some patient subgroups [25]. If greater variability is present, it is of interest as to whether this manifests in the form of a spectrum (following a unimodal distribution), or whether there is evidence of a bimodal distribution, consistent with discrete subtypes of schizophrenia with different brain glutamate levels [15].
The hypothesis of greater glutamate variability in patients can be formally tested by conducting a meta-analysis of variability, as previously employed to examine the variability of glutathione [26], antipsychotic treatment response [27] and brain structure in schizophrenia [28]. One meta-analysis examined the variability of glutamate in schizophrenia compared to controls, but this was limited to glutamate in the dorsolateral prefrontal cortex (DLPFC) [29]. In addition, the hypothesis of discrete subgroups can be tested by examining the distribution of individual patient data [30].
In the current meta-analysis, we hypothesised that patients with schizophrenia would exhibit greater variability of brain glutamate, glutamine and Glx levels than controls. We complemented this with analysis of the distribution of individual-level data, as a bimodal distribution of glutamatergic metabolites in patients would support the existence of discrete glutamate subgroups. Additionally, we present an updated meta-analysis of case-control differences in glutamate metabolites to include recently published data that has not been previously summarised. In accordance with recent meta-analyses, we hypothesised that glutamine levels in thalamus and glutamate and Glx levels in the basal ganglia will be higher in schizophrenia patients compared to controls, and that MFC glutamate will be lower. Sensitivity analyses examined whether variability or standardised mean differences (SMD) in glutamatergic metabolites were associated with antipsychotic medication exposure, and meta-regressions tested for potential effects of age, sex, symptom severity and antipsychotic medication dose. On the basis of results from a recent mega-analysis [12], we hypothesised that age will not be associated with SMD, whereas medication exposure will be associated with negative effect sizes and symptom severity with positive effect size differences between patients and controls. Meta-regressions of the same variables were performed to investigate potential sources of patient-control differences in variability.
Methods
Search strategy and study selection
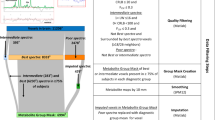
We followed PRISMA guidelines and registered the study on PROSPERO (CRD42021251798). MEDLINE and EMBASE databases were searched to identify articles published from inception to September 23, 2022, using the search terms: (1) MRS or magnetic resonance spectroscopy AND (2) schizophrenia or psychosis or UHR or ARMS or schizoaffective or “Psychosis risk” OR “at risk mental state” or “psychotic experience” or “psychosis spectrum” OR (“genetic risk” and (psychosis or schizophrenia)) OR (“high risk” and (psychosis or schizophrenia)). Screening and selection of studies was performed independently by three authors (KM, KB, CB). 1H-MRS studies reporting glutamate, glutamine, or Glx values for a schizophrenia patient group in comparison with a healthy volunteer group were included in the analysis. Studies in clinical high risk or genetic high risk cohorts have been summarised elsewhere [31] and were excluded from the current analysis on individuals meeting diagnostic criteria. In the case of longitudinal studies, only the values for the first time point were included. If the same sample or partially overlapping samples were included in more than one report, data from the study with the largest sample were included. Where the mean or standard deviations for glutamate measures were unavailable in the published manuscript the authors were contacted and values requested. We also requested individual patient level datasets from authors as part of a previous mega-analysis (for further details see 12).
Data extraction and processing
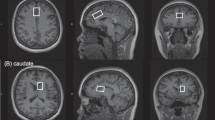
Mean and standard deviation (SD) values of glutamate, glutamine, or Glx concentrations were extracted (K.M.) and verified independently (S.A. and B.K.), and categorized into the following brain regions of interest: (1) medial frontal cortex (MFC), including voxels in the medial prefrontal cortex and in the anterior cingulate cortex since these voxels often spatially overlap; (2) dorsolateral prefrontal cortex (DLPFC); (3) frontal white matter; (4) thalamus; (5) temporal lobe (including superior temporal gyrus and hippocampus); (6) basal ganglia (including caudate, putamen, globus pallidus and substantia nigra). When more than one clinical group was reported in a single study, the values were treated as independent data sets and the number of controls was adjusted by dividing by the number of clinical groups. We also extracted participant age, sex, Positive and Negative Syndrome Scale (PANSS) scores and antipsychotic dose in chlorpromazine equivalents (CPZ), and the SD values for these variables (data available in Supplementary eTable 1. Data and R code also available on github [32]). The quality of included studies was rated using the Newcastle-Ottawa Scale [33] (Supplementary eAppendix 1). Metabolite measures using J-edited and echo-planar spectroscopic imaging (EPSI) acquisition sequences were scaled by 1000 [34,35,36] or 100,000 to obtain comparable values [37].
Meta-analysis outcome measures
The relative variability between patients and controls can be quantified using the log variability ratio (VR), taking into account the standard deviation of mean glutamate values. In many natural systems mean scales with variability, and if this is not accounted for, variability differences can be influenced by mean differences. We therefore used the log coefficient of variation ratio (CVR) for our primary analyses, which adjusts the VR for mean differences between groups:
Where \(\hat \sigma _p\) and \(\hat \sigma _c\) are the unbiased estimates of the population standard deviation for the patient and control groups respectively, \(\bar x_p\) and \(\bar x_c\) are the mean values, Sp and Sc are the reported SDs, while np and nc are the sample sizes.
A CVR above 0 indicates greater variability in patients, and below 0 indicates greater variability in controls. While CVR is used for our primary analysis, VR is presented in the supplementary results.
The standardised mean differences (Hedges’ g) of glutamatergic metabolites between patients and controls were calculated using a random effects model. A Hedges’ g value of 0 indicates no difference between patients and controls, negative values indicate lower glutamatergic metabolite levels in patients than controls, and positive values denote higher metabolite levels in patients than controls. I2 values were calculated to quantify between-study inconsistency. Benjamini-Hochberg false discovery rate (FDR) was used to correct for the number of regions (Q false discovery rate of 10%).
Sensitivity analyses examined CVR and Hedges’ g effect sizes in antipsychotic-naïve and medicated patients separately, which were then compared in a Wald type test to assess significance. Meta-regressions assessed the impact of the combined mean age of sample (patients and controls), proportion of males in combined sample, PANSS total score and CPZ on CVR and Hedges’ g effect sizes. Significant meta-regressions were followed up with meta-regressions to determine if the SD of a demographic/clinical variable was associated with CVR. Significant CVR results were followed up with meta-regressions to determine if CVR was associated with 1H-MRS data quality, namely (1) signal to noise ratio (SNR) (patient mean divided by control mean) and (2) field homogeneity (linewidth as full width half maximum values: FWHM) (patient mean divided by control mean). Analyses were carried out in R (version 4.1.1), using the “metafor” [38] and “weights” packages, while plots were generated using “ggplot2” [39].
Data distribution
The modal distribution of data was investigated in individual-level patient data from 33 studies contributed by the 1H-MRS in Schizophrenia Investigators consortium (for further details see 12). For each study, data was normalized (mean-scaled) and analysed using Hartigan’s Dip Test of Unimodality [30] (R package “dip.test”).
Results
Study selection
The search identified 2527 articles, 123 of which met criteria for the meta-analysis (Supplementary eFig. 1 and eResults 1 for references), including data on 8256 patients with schizophrenia and 7532 controls. The average age was 31 years and males constituted 66% of participants (Supplementary eTable 1 for raw data). Studies examined first episode psychosis patients (57 studies), patients with established schizophrenia (72 studies) and antipsychotic-naïve patients (33 studies).
Variability analyses
Meta-analysis of CVR
There was a positive relationship between mean glutamatergic metabolite level and standard deviation (weighted rp = 0.70, p < 0.001, Supplementary eFig. 2), indicating mean-scaling of variability and the appropriateness of CVR as the primary variability outcome measure.
In the MFC, variability of glutamate, glutamine and Glx were significantly increased in patients compared with controls (CVR = 0.15, 95% CI 0.08–0.22, p < 0.001, 65 studies; CVR = 0.15, 95% CI 0.05–0.25, p = 0.003, 26 studies; CVR = 0.11, 95% CI 0.04–0.18, p = 0.002, 54 studies respectively; Fig. 1). In the DLPFC, variability of glutamine and Glx were significantly increased in patients compared with controls (CVR = 0.14, 95% CI 0.00–0.29, p = 0.05, 8 studies and CVR = 0.24, 95% CI 0.12–0.36, p < 0.001, 22 studies), but the variability of glutamate did not differ (Fig. 1). In the thalamus, variability of glutamate and Glx were significantly increased in patients compared with controls (CVR = 0.16, 95% CI 0.04–0.27, p = 0.008, 14 studies and CVR = 0.19, 95% CI 0.05–0.32, p = 0.008, 13 studies), but the variability of glutamine did not differ (Fig. 1). For the frontal white matter, basal ganglia and temporal lobe, the variability of glutamatergic metabolite measures did not differ between patients and controls (Fig. 1). All findings survived FDR correction.

A CVR in schizophrenia patients compared to healthy volunteers (HV). B CVR in patients treated with antipsychotic medication compared to HV. C CVR in antipsychotic-naïve patients compared to HV. Significant results are shown in blue. Variability was significantly higher in patients relative to HV in the medial frontal cortex (MFC; all glutamatergic metabolites), dorsolateral prefrontal cortex (DLPFC: Glutamine and Glx) and Thalamus (Thal; Glutamate and Glx-). There were no significant differences in glutamatergic metabolite variability in the frontal white matter (fWM), temporal lobe (Temp) and basal ganglia (BG) in patients compared with HV. Reduced Glx variability in the basal ganglia (BG) was found in medicated patients relative to HV. CVR, 95% confidence intervals, P value and I2 presented.
Sensitivity analyses examined antipsychotic-naïve and medicated patients separately, and produced the same pattern of results for the MFC and DLPFC (Fig. 1), although the variability of glutamate did not differ between antipsychotic-naïve patients and healthy volunteers in the MFC. In the thalamus, when analysis was restricted to antipsychotic-naïve patients the variability of glutamate no longer differed between groups (Fig. 1). In the basal ganglia, Glx variability was reduced in medicated patients compared with controls (CVR = −0.15, 95% CI −0.26 to −0.03, p = 0.02, 15 studies), but this reduction was not apparent in antipsychotic-naïve patients (3 studies) or across the whole sample. Significant differences in CVR were not found between antipsychotic-naïve and medicated patients in the MFC (glutamate), thalamus (glutamate) and basal ganglia (Glx).
Log VR results were largely the same as CVR and are reported in the Supplement (eFig. 3).
Meta-regressions of CVR
PANSS total score was positively associated with glutamine variability (CVR) in the MFC (z = 0.01, p = 0.02, 9 studies, Fig. 2) and glutamate variability in the basal ganglia (z = 0.007, p = 0.02, 11 studies), indicating that studies examining patients with a greater symptom severity showed greater glutamatergic variability in patients compared to controls. Age (of patients and controls combined) was negatively associated with glutamate variability in the temporal lobe (z = −0.03, p = 0.02, 14 studies) and basal ganglia (z = −0.03, p = 0.003, 12 studies), indicating that studies examining younger participants showed greater variability in the patient group relative to controls. Age (of patients and controls combined) was positively associated with glutamate variability in the MFC (z = 0.01, p = 0.02, 65 studies). CPZ and proportion of males were not significantly related with CVR.

A In the temporal lobe and B basal ganglia, higher glutamate variability in patients relative to HV was associated with studies in younger participants. C In the medial frontal cortex (MFC), higher glutamate variability in patients relative to HV was associated with studies in older participants. For glutamine in the D MFC and E glutamate in the basal ganglia, higher variability in patients relative to healthy volunteers (HV) was associated with studies in more symptomatic patients (according to PANSS Total Scores). Bubble size represents total sample of patients and HV.
The SD of PANSS total score for each study was not associated with glutamine variability in the MFC or glutamate variability in the basal ganglia, indicating that the association between PANSS total score and CVR is not explained by increased variability in PANSS total score. Similarly, there was no association between age SD and glutamate CVR in the basal ganglia. In the temporal lobe, greater age SD was associated with reduced CVR in glutamate (z = −0.05, p = 0.05, 14 studies), suggesting that greater glutamate CVR in younger patients is unlikely to be explained by greater variability in age in younger cohorts. 1H-MRS data quality measures (SNR and FWHM) were not associated with CVR in the MFC, DLPFC or thalamus.
Distribution of individual patient glutamate and Glx data
27 studies contributed individual participant-level glutamatergic metabolite data in the MFC. 18 studies were in patients previously or currently treated with antipsychotics, 6 studies were in antipsychotic-naïve or minimally medicated cohorts, and 3 studies included both antipsychotic-naïve and medicated patients. Hartigan’s dip test found unimodality in the distribution of mean-centred Cr-scaled glutamate (D = 0.01, p = 0.99) and Glx in patients (D = 0.01, p = 0.99), and for CSF-corrected glutamate (D = 0.02, p = 0.37) and Glx in patients (D = 0.01, p = 0.68). Hartigan’s dip test for individual studies found unimodality in 26 studies [15, 16, 21, 22, 40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] and bimodality in 1 study [61].
For the temporal lobe, 6 studies contributed individual participant-level glutamatergic metabolite data. 4 studies were in patients previously or currently treated with antipsychotics and 2 studies were in antipsychotic-naïve or minimally medicated cohorts. Hartigan’s dip test found unimodality in the distribution of mean-centred CSF-corrected Glx (D = 0.04, p = 0.581, 3 studies) and Cr-scaled Glx in patients (D = 0.03, p = 0.68, 6 studies). Hartigan’s dip test for individual studies found unimodality in all 6 studies [51, 53, 62,63,64,65].
Standardised mean differences analyses
Meta-analysis of hedges’ g effect sizes
In the MFC, glutamate levels were significantly lower in patients compared with controls (g = −0.15, 95% CI −0.29 to −0.01, p = 0.03, 65 studies, Fig. 3), whereas glutamine and Glx levels did not differ (Fig. 3). In the thalamus, glutamine levels were significantly higher in patients compared with controls (g = 0.53, 95% CI 0.30–0.75, p < 0.001, 6 studies), and glutamate and Glx levels did not differ (Fig. 3). In the basal ganglia, Glx levels were significantly higher in patients compared with controls (g = 0.28, 95% CI 0.12–0.44, p < 0.001, 18 studies) and glutamate and glutamine did not differ (Fig. 3). For the DLPFC, frontal white matter and temporal lobe, glutamatergic metabolite levels did not differ between patients and controls (Fig. 3). All findings survived FDR correction except glutamate in the MFC.

A SMD in schizophrenia patients compared to healthy volunteers (HV). B SMD in patients treated with antipsychotic medication compared to HV. C SMD in antipsychotic-naïve patients compared to HV. Significant results are shown in green. Glutamate levels in the medial frontal cortex (MFC) were significantly lower in patients relative to HV, whereas glutamine levels in the thalamus (Thal) and Glx levels in the basal ganglia (BG) were significantly higher in patients relative to HV. There were no significant differences in glutamatergic metabolite levels in the dorsolateral prefrontal cortex (DLPFC), frontal white matter (fWM) or temporal lobe (Temp) between patients and HV. Significant differences in glutamatergic metabolites were no longer present when antipsychotic-naïve patients were assessed. Hedges’ g, 95% confidence intervals, P value and I2 presented.
The same pattern of results was apparent when analyses were restricted to medicated patients (Fig. 3). When analyses were restricted to antipsychotic-naïve patients there were no significant differences in glutamatergic metabolites. However, there were no significant differences in Hedges’ g effect sizes between antipsychotic-naïve and medicated patients in the MFC (glutamate) or basal ganglia (Glx) and an insufficient number of studies to assess Hedges’ g effect sizes in antipsychotic-naïve patients for glutamine in the thalamus.
Meta-regressions of hedges’ g effect sizes
Mean PANSS total score was positively associated with effect sizes for elevated glutamate in patients in the temporal lobe (z = 0.05, p = 0.008, 5 studies) and basal ganglia (z = 0.01, p = 0.01, 11 studies), and negatively correlated with glutamate in the DLPFC (z = −0.02, p = 0.03, 12 studies, Fig. 4). Age was negatively associated with the effect size for elevated glutamine in patients compared to controls in the basal ganglia (z = −0.15, p = 0.003, 4 studies, Supplementary eFig. 4). In frontal white matter, age was negatively associated with the effect size for elevated glutamate in patients (z = −0.04, p = 0.03, 7 studies), but positively associated with the effect size for elevated Glx (z = −0.02, p = 0.02, 12 studies). A higher proportion of males was associated with lower MFC glutamate (z = −0.02, p < 0.001, 64 studies) and frontal white matter Glx in patients compared to controls (z = −0.03, p = 0.02, 10 studies) (Fig. 4). Lower CPZ associated with effect sizes for lower Glx in patients in the temporal lobe (z = 0.003, p = 0.03). CPZ did not associate with Hedges’ g effect sizes in other brain regions.

A In the dorsolateral prefrontal cortex (DLPFC), lower glutamate levels in patients relative to healthy volunteers (HV) was associated with studies examining patients with greater symptom severity (according to PANSS Total Scores). In the (B) basal ganglia and (C) temporal lobe, higher glutamate levels were associated with studies examining patients with greater symptom severity (according to PANSS Total Scores). D In the medial frontal cortex (MFC) and (E) frontal white matter, lower glutamate and Glx levels in patients relative to HV was associated with studies including a higher proportion of males. F In the temporal lobe, lower Glx in patients relative to HV was associated with lower CPZ. Bubble size represents total sample of patients and HV.
Discussion
The main findings of this meta-analysis are that schizophrenia is associated with increased variability in the concentrations of glutamatergic metabolites in the brain, together with regional differences in mean glutamatergic metabolite concentrations. The greatest amount of data were available for the MFC (65 studies), where glutamate levels were lower and the variability of all glutamate metabolites (glutamate, glutamine and Glx) were increased in schizophrenia compared to controls (although the finding of lower MFC glutamate in patients compared to controls did not survive FDR correction). While the emphasis has been on glutamate in the MFC in schizophrenia, our results additionally indicate glutamatergic dysregulation in other brain regions, finding increased variability in glutamine and Glx in the DLPFC, higher levels of Glx in the basal ganglia, and higher levels of glutamine alongside increased variability of glutamate and Glx in the thalamus. The increased variability in glutamatergic metabolites tended to be most apparent in studies examining patients who were more symptomatic.
Glutamate is tightly regulated in the brain through complex feedback mechanisms which may be disrupted in schizophrenia [66]. The increased variability in glutamatergic metabolites in schizophrenia indicate a spectrum of disturbances in glutamate homeostatic control between individual patients, resulting in a wide range of concentration values. Regionally, our analysis of the available data in schizophrenia indicates dysfunctional regulation (i.e. increased variability) of glutamatergic metabolite concentrations in the MFC, DLPFC and thalamus, and mean value decreases in the MFC and increases in the thalamus and basal ganglia. Increased glutamatergic variability in schizophrenia, as observed at the macro scale with 1H-MRS, could relate to individual differences in the nature or in the extent of the underlying molecular pathophysiological mechanisms. We did not find evidence for a bimodal distribution within individual participant data, as would be expected if between-subject glutamatergic differences were driven by the presence or absence of a simple, discrete variable. In contrast, the observed unimodal distributions are consistent with the view that glutamatergic pathology in schizophrenia arises secondary to a range of factors that vary amongst patients (e.g polygenic and multiple environmental vulnerability variables) [7,8,9]. Therefore, findings of higher glutamate levels in treatment resistant patients in comparison to treatment responders [15,16,17,18,19,20,21,22,23,24] may represent a continuum, rather than the presence of discrete subtypes.
There was evidence in some regions that the variability of glutamate or glutamine was related to symptom severity and age. In both the basal ganglia and MFC, variability was greater in studies recruiting more symptomatic patients. This could indicate that dysfunction of glutamate regulatory mechanisms is greatest in those patients with highest illness burden. These findings were not explained by increased variance in symptom scores in studies recruiting more unwell patients, or by the absence of antipsychotic medication as variance was similar in medicated compared to unmedicated cohorts. In the basal ganglia and temporal lobe, variability was higher in studies recruiting younger patients. In older patients, our results indicated that glutamate in these regions may be even more homogenous than that seen in controls, which could potentially reflect regulatory over-compensation. Alternatively, this may reflect greater clinical heterogeneity within first episode cohorts, for example in respect to diagnosis. In contrast in the MFC glutamate was more variable in studies including older patients. Potentially, this could relate to heterogeneity in clinical outcomes, as treatment response has been most strongly linked to differential glutamate levels in this region [15, 17,18,19,20,21,22,23]. The relationship between basal ganglia glutamate and symptom severity was largely influenced by a single study. Further studies in highly symptomatic patients are therefore needed to confirm this finding, and to determine whether treatment response contributes to increased variability in the MFC.
As increased variability was of comparable magnitudes in antipsychotic-naive and medicated patient cohorts, this suggests that variability in glutamate does not result from differential effects of antipsychotic medication on glutamate levels between individuals [14, 21]. Although a recent meta-analysis of DLPFC glutamate found higher variability in antipsychotic medicated patients and lower variability in medication-naïve patients [29]. Our analysis, including 12 more recent studies and investigating DLPFC glutamate and Glx separately, did not find any effect of medication status in this region. In fact, in the basal ganglia, it appeared that antipsychotic-treated cohorts displayed reduced variability compared to controls. Potentially this could be due to a regulatory effect of antipsychotics on basal ganglia Glx [67, 68].
The meta-analysis of standardised mean differences found lower MFC glutamate levels and higher thalamic glutamine and basal ganglia Glx in patients compared to controls, although lower MFC glutamate did not survive FDR correction. These results are consistent with recent meta-analyses [2,3,4,5,6], but substantially extend them by including 20 new datasets for MFC glutamate and 2 new datasets for thalamic glutamine. Stratified analyses found that lower MFC glutamate was observed across studies examining medicated patients but not across studies examining antipsychotic-naïve patients. Thus, antipsychotic medication could lower MFC glutamate levels, as indicated by longitudinal studies [14, 21] and a mega-analysis [12], although the meta-regression with CPZ dose was not significant. Our analysis also revealed relationships between the proportion of males in the study and MFC glutamate and frontal white matter Glx effect sizes, such that a higher proportion of males was associated with lower glutamate levels in patients compared to controls. In schizophrenia, males show greater elevation in peripheral d-serine (an NMDA receptor co-agonist) [69], and, in the postmortem ACC, less upregulation of glutamine synthetase [70] and lower expression of GABAergic genes encoding proteins which modulate glutamate neurotransmission [71]. The effect of sex should be further investigated on the individual level through large studies or mega-analyses. Although there was no difference in glutamate metabolite variability in the temporal lobe, higher glutamate levels were found in studies which included more highly symptomatic patients. This is also consistent with our recent mega-analysis [12]. Finally, other than in the basal ganglia and frontal white matter, meta-regressions did not find an accelerated loss of glutamatergic metabolites in patients with age for the majority of brain regions, also consistent with our recent mega-analysis [12].
A limitation of the meta-analysis is the high between-study inconsistency, as measured by I2, for most brain regions studied. This was highest in the temporal lobe and may relate to the difficulty of obtaining good quality 1H-MRS imaging in this region. There is a possibility that case-control differences in variability result from greater movement artifacts in patient populations [72], however CVR did not correlate with SNR or FWHM values. A recent meta-analysis emphasises the importance of using strict Cramér–Rao lower bound criteria (≤7%) and short echo times (≤20 ms) to improve 1H-MRS consistency [5]. Furthermore, the glutamine signal cannot be accurately resolved from glutamate below 3 T, although the majority of studies reporting glutamine were conducted above 3 T. As voxel placement varied between studies, broad categories of brain regions were used, limiting the regional specificity of our results. Meta-regression analyses of clinical and demographic variables are limited to the study level and are not sensitive to variation within individual studies (although meta-regressions with the SD of clinical and demographic variables were carried out). Lastly, the number of included studies is low for some brain regions, such as the thalamus, and there are a small number of studies examining antipsychotic-naïve patients in all regions except the MFC, and so these sensitivity analyses should be considered preliminary.
In summary, this meta-analysis demonstrates increased regional variability in glutamatergic metabolites in schizophrenia in addition to mean differences compared to controls. Increased inter-individual differences in glutamatergic metabolites in schizophrenia are likely to have a complex mechanistic basis. Further work is also required to determine the clinical consequences along the spectrum of glutamate dysregulation. Both glutamatergic metabolite levels [12] and interindividual variability appear to be greater in more symptomatic patients. Neurobiological heterogeneity may also relate to heterogeneity in antipsychotic response in schizophrenia, and some studies have shown that glutamatergic metabolite levels in the MFC, thalamus, DLPFC and striatum associate with the degree of antipsychotic response [15,16,17,18,19,20,21,22,23,24, 68, 73, 74]. Our findings are relevant to the on-going effort to develop novel drug therapies to target glutamate dysfunction in schizophrenia, as the presence of glutamatergic heterogeneity may indicate the importance of targeting more specific patient subgroups.
References
McCutcheon RA, Krystal JH, Howes OD. Dopamine and glutamate in schizophrenia: biology, symptoms and treatment. World Psychiatry. 2020;19:15–33.
Merritt K, Egerton A, Kempton MJ, Taylor MJ, McGuire PK. Nature of glutamate alterations in schizophrenia a meta-analysis of proton magnetic resonance spectroscopy studies. JAMA Psychiatry. 2016;73:665–74.
Nakahara T, Tsugawa S, Noda Y, Ueno F, Honda S, Kinjo M, et al. Glutamatergic and GABAergic metabolite levels in schizophrenia-spectrum disorders: a meta-analysis of 1H-magnetic resonance spectroscopy studies. Mol Psychiatry. 2021; https://www.nature.com/articles/s41380-021-01297-6.
Sydnor VJ, Roalf DR. Glutamatergic and GABAergic metabolite levels in schizophrenia-spectrum disorders: a meta-analysis of 1H-magnetic resonance spectroscopy studies: Implications for studies of psychosis risk. Schizophr Res. 2020; https://pubmed.ncbi.nlm.nih.gov/32723493/. Accessed 6 Oct 2020.
Smucny J, Carter CS, Maddock RJ. Medial prefrontal cortex glutamate is reduced in schizophrenia and moderated by measurement quality: a meta-analysis of proton magnetic resonance spectroscopy studies. Biol Psychiatry. 2021;90:643–51. https://linkinghub.elsevier.com/retrieve/pii/S0006322321013937.
Marsman A, van den Heuvel MP, Klomp DWJ, Kahn RS, Luijten PR, Hulshoff Pol HE. Glutamate in schizophrenia: a focused review and meta-analysis of 1H-MRS studies. Schizophr Bull. 2013;39:120–9. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3523901&tool=pmcentrez&rendertype=abstract.
Legind CS, Broberg BV, Mandl RCW, Brouwer R, Anhøj SJ, Hilker R, et al. Heritability of cerebral glutamate levels and their association with schizophrenia spectrum disorders: a 1[H]-spectroscopy twin study. Neuropsychopharmacology. 2019;44:581–9. http://www.nature.com/articles/s41386-018-0236-0.
Bustillo JR, Patel V, Jones T, Jung R, Payaknait N, Qualls C, et al. Risk-conferring glutamatergic genes and brain glutamate plus glutamine in schizophrenia. Front Psychiatry. 2017. http://journal.frontiersin.org/article/10.3389/fpsyt.2017.00079/full.
Egerton A, Grace AA, Stone J, Bossong MG, Sand M, McGuire P. Glutamate in schizophrenia: Neurodevelopmental perspectives and drug development. Schizophr Res. 2020;223:59–70. https://linkinghub.elsevier.com/retrieve/pii/S0920996420304710.
Merritt K, Perez-Iglesias R, Sendt K-V, Goozee R, Jauhar S, Pepper F, et al. Remission from antipsychotic treatment in first episode psychosis related to longitudinal changes in brain glutamate. npj Schizophr 2019;5:12 http://www.ncbi.nlm.nih.gov/pubmed/31371817.
Merritt K, McGuire P, Egerton A. Relationship between glutamate dysfunction and symptoms and cognitive function in psychosis. Front Psychiatry. 2013;4.
Merritt K, McGuire PK, Egerton A, Aleman A, Block W, Bloemen OJN, et al. Association of age, antipsychotic medication, and symptom severity in schizophrenia with proton magnetic resonance spectroscopy brain glutamate level. JAMA Psychiatry. 2021;78:667 https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2778479.
Adams RA, Pinotsis D, Tsirlis K, Unruh L, Mahajan A, Horas AM, et al. Computational modeling of electroencephalography and functional magnetic resonance imaging paradigms indicates a consistent loss of pyramidal cell synaptic gain in schizophrenia. Biol Psychiatry. 2021; https://linkinghub.elsevier.com/retrieve/pii/S0006322321014992.
Egerton A, Bhachu A, Merritt K, McQueen G, Szulc A, McGuire P. Effects of antipsychotic administration on brain glutamate in schizophrenia: a systematic review of longitudinal1H-MRS studies. Front Psychiatry. 2017;8:66.
Mouchlianitis E, Bloomfield MAP, Law V, Beck K, Selvaraj S, Rasquinha N, et al. Treatment-resistant schizophrenia patients show elevated anterior cingulate cortex glutamate compared to treatment-responsive. Schizophr Bull. 2016;42:744–52. http://www.ncbi.nlm.nih.gov/pubmed/26683625.
Goldstein ME, Anderson VM, Pillai A, Kydd RR, Russell BR. Glutamatergic neurometabolites in clozapine-responsive and -resistant schizophrenia. Int J Neuropsychopharmacol. 2015;18:pyu117–17. http://www.ncbi.nlm.nih.gov/pubmed/25603859.
Demjaha A, Egerton A, Murray RM, Kapur S, Howes OD, Stone JM, et al. Antipsychotic treatment resistance in schizophrenia associated with elevated glutamate levels but normal dopamine function. Biol Psychiatry. 2014;75:e11–3. http://www.ncbi.nlm.nih.gov/pubmed/23890739.
Iwata Y, Nakajima S, Plitman E, Caravaggio F, Kim J, Shah P, et al. Glutamatergic neurometabolite levels in patients with ultra-treatment-resistant schizophrenia: a cross-sectional 3T proton magnetic resonance spectroscopy study. Biol Psychiatry. 2019;85:596–605. http://www.ncbi.nlm.nih.gov/pubmed/30389132.
Tarumi R, Tsugawa S, Noda Y, Plitman E, Honda S, Matsushita K, et al. Levels of glutamatergic neurometabolites in patients with severe treatment-resistant schizophrenia: a proton magnetic resonance spectroscopy study. Neuropsychopharmacology. 2020;45:632–40. https://pubmed.ncbi.nlm.nih.gov/31842203/.
Szulc A, Konarzewska B, Galinska-Skok B, Lazarczyk J, Waszkiewicz N, Tarasow E, et al. Proton magnetic resonance spectroscopy measures related to short-term symptomatic outcome in chronic schizophrenia. Neurosci Lett. 2013;547:37–41. http://www.ncbi.nlm.nih.gov/pubmed/23665527.
Egerton A, Broberg BV, Van Haren N, Merritt K, Barker GJ, Lythgoe DJ, et al. Response to initial antipsychotic treatment in first episode psychosis is related to anterior cingulate glutamate levels: a multicentre 1 H-MRS study (OPTiMiSE). Mol Psychiatry. 2018;23:2145–55.
Egerton A, Brugger S, Raffin M, Barker GJ, Lythgoe DJ, McGuire PK, et al. Anterior cingulate glutamate levels related to clinical status following treatment in first-episode schizophrenia. Neuropsychopharmacology. 2012;37:2515–21.
Egerton A, Murphy A, Donocik J, Anton A, Barker GJ, Collier T, et al. Dopamine and glutamate in antipsychotic-responsive compared with antipsychotic-nonresponsive psychosis: a multicenter positron emission tomography and magnetic resonance spectroscopy study (STRATA). Schizophr Bull. 2020; https://academic.oup.com/schizophreniabulletin/advance-article/doi/10.1093/schbul/sbaa128/5903699.
Bojesen KB, Ebdrup BH, Jessen K, Sigvard A, Tangmose K, Edden RAE, et al. Treatment response after 6 and 26 weeks is related to baseline glutamate and GABA levels in antipsychotic-naïve patients with psychosis. Psychol Med. 2020;50:2182–93. https://www.cambridge.org/core/product/identifier/S0033291719002277/type/journal_article.
Kinon BJ, Millen BA, Zhang L, McKinzie DL. Exploratory analysis for a targeted patient population responsive to the metabotropic glutamate 2/3 receptor agonist pomaglumetad methionil in schizophrenia. Biol Psychiatry. 2015;78:754–62. https://linkinghub.elsevier.com/retrieve/pii/S0006322315002541.
Palaniyappan L, Sabesan P, Li X, Luo Q. Schizophrenia increases variability of the central antioxidant system: a meta-analysis of variance from MRS studies of glutathione. Front Psychiatry. 2021;12. https://www.frontiersin.org/articles/10.3389/fpsyt.2021.796466/full.
McCutcheon RA, Pillinger T, Mizuno Y, Montgomery A, Pandian H, Vano L, et al. The efficacy and heterogeneity of antipsychotic response in schizophrenia: A meta-analysis. Mol Psychiatry. 2021;26:1310–20. http://www.nature.com/articles/s41380-019-0502-5.
Brugger SP, Howes OD. Heterogeneity and homogeneity of regional brain structure in schizophrenia. JAMA Psychiatry. 2017;74:1104 http://archpsyc.jamanetwork.com/article.aspx?doi=10.1001/jamapsychiatry.2017.2663.
Kaminski J, Mascarell-Maricic L, Fukuda Y, Katthagen T, Heinz A, Schlagenhauf F. Glutamate in the dorsolateral prefrontal cortex in patients with schizophrenia: a meta-analysis of 1H-magnetic resonance spectroscopy studies. Biol Psychiatry. 2020;89:270–7.
Hartigan JA, Hartigan PM. The dip test of unimodality. Ann Stat. 1985;13:70–84. http://www.jstor.org/stable/2241144.
McCutcheon RA, Merritt K, Howes OD. Dopamine and glutamate in individuals at high risk for psychosis: a meta-analysis of in vivo imaging findings and their variability compared to controls. World Psychiatry. 2021;20:405–16. http://www.ncbi.nlm.nih.gov/pubmed/34505389.
Merritt K, McCutcheon R variability. 2023; https://github.com/katemerritt/variability/.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5. http://link.springer.com/10.1007/s10654-010-9491-z.
de la Fuente-Sandoval C, Reyes-Madrigal F, Mao X, León-Ortiz P, Rodríguez-Mayoral O, Jung-Cook H, et al. Prefrontal and striatal gamma-aminobutyric acid levels and the effect of antipsychotic treatment in first-episode psychosis patients. Biol Psychiatry. 2018;83:475–83. http://www.ncbi.nlm.nih.gov/pubmed/29132653.
Bustillo JR, Upston J, Mayer EG, Jones T, Maudsley AA, Gasparovic C, et al. Glutamatergic hypo-function in the left superior and middle temporal gyri in early schizophrenia: a data-driven three-dimensional proton spectroscopic imaging study. Neuropsychopharmacology. 2020;45:1851–9. http://www.nature.com/articles/s41386-020-0707-y.
Bustillo JR, Mayer EG, Upston J, Jones T, Garcia C, Sheriff S, et al. Increased glutamate plus glutamine in the right middle cingulate in early schizophrenia but not in bipolar psychosis: a whole brain 1H-MRS study. Front Psychiatry. 2021;12. https://www.frontiersin.org/articles/10.3389/fpsyt.2021.660850/full.
da Silva Alves F, Boot E, Schmitz N, Nederveen A, Vorstman J, Lavini C, et al. Proton magnetic resonance spectroscopy in 22q11 deletion syndrome. PLoS One. 2011;6:e21685 http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3128078&tool=pmcentrez&rendertype=abstract.
Viechtbauer W. Conducting meta-analyses in R with the metafor Package. J Stat Softw. 2010;36:1–48. https://www.jstatsoft.org/index.php/jss/article/view/v036i03.
Wickham H. ggplot2: elegant graphics for data analysis. Springer-Verlag New York; 2009. http://ggplot2.org.
Goto N, Yoshimura R, Kakeda S, Nishimura J, Moriya J, Hayashi K, et al. Six-month treatment with atypical antipsychotic drugs decreased frontal-lobe levels of glutamate plus glutamine in early-stage first-episode schizophrenia. Neuropsychiatr Dis Treat. 2012;8:119–22.
Natsubori T, Inoue H, Abe O, Takano Y, Iwashiro N, Aoki Y, et al. Reduced frontal glutamate + glutamine and N-acetylaspartate levels in patients with chronic schizophrenia but not in those at clinical high risk for psychosis or with first-episode schizophrenia. Schizophr Bull. 2014;40:1128–39. http://www.ncbi.nlm.nih.gov/pubmed/24023251.
Theberge J, Bartha R, Drost DJ, Menon RS, Malla A, Takhar J, et al. Glutamate and glutamine measured with 4.0 T proton MRS in never-treated patients with schizophrenia and healthy volunteers. Am J Psychiatry. 2002;159:1944–6.
Théberge J, Al-Semaan Y, Williamson PC, Menon RS, Neufeld RWJ, Rajakumar N, et al. Glutamate and glutamine in the anterior cingulate and thalamus of medicated patients with chronic schizophrenia and healthy comparison subjects measured. Am J Psychiatry. 2003;160:2231–3. http://journals.psychiatryonline.org/article.aspx?articleid=176549.
Wood SJ, Yücel M, Wellard RM, Harrison BJ, Clarke K, Fornito A, et al. Evidence for neuronal dysfunction in the anterior cingulate of patients with schizophrenia: a proton magnetic resonance spectroscopy study at 3 T. Schizophr Res. 2007;94:328–31. http://www.ncbi.nlm.nih.gov/pubmed/17574388.
Tibbo PG, Bernier D, Hanstock CC, Seres P, Lakusta B, Purdon SE. 3-T proton magnetic spectroscopy in unmedicated first episode psychosis: a focus on creatine. Magn Reson Med. 2013;69:613–20. http://www.ncbi.nlm.nih.gov/pubmed/22511463.
Bustillo JR, Rowland LM, Mullins P, Jung R, Chen H, Qualls C, et al. 1H-MRS at 4 tesla in minimally treated early schizophrenia. Mol Psychiatry. 2010;15:629–36. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2892215&tool=pmcentrez&rendertype=abstract.
Bustillo JR, Chen H, Jones T, Lemke N, Abbott C, Qualls C, et al. Increased glutamine in patients undergoing long-term treatment for schizophrenia: a proton magnetic resonance spectroscopy study at 3 T. JAMA Psychiatry. 2014;71:265–72. http://www.ncbi.nlm.nih.gov/pubmed/24402128.
Coughlin JM, Tanaka T, Marsman A, Wang H, Bonekamp S, Kim PK, et al. Decoupling of N-acetyl-aspartate and glutamate within the dorsolateral prefrontal cortex in schizophrenia. Curr Mol Med. 2015;15:176–83. http://www.ncbi.nlm.nih.gov/pubmed/25732147.
Taylor R, Schaefer B, Densmore M, Neufeld RWJ, Rajakumar N, Williamson PC, et al. Increased glutamate levels observed upon functional activation in the anterior cingulate cortex using the Stroop Task and functional spectroscopy. Neuroreport. 2015;26:107–12. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00001756-201502010-00002.
Ongür D, Prescot AP, McCarthy J, Cohen BM, Renshaw PF. Elevated gamma-aminobutyric acid levels in chronic schizophrenia. Biol Psychiatry. 2010;68:667–70. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2942977&tool=pmcentrez&rendertype=abstract.
Gallinat J, McMahon K, Kühn S, Schubert F, Schaefer M. Cross-sectional study of glutamate in the anterior cingulate and hippocampus in schizophrenia. Schizophr Bull. 2016;42:425–33. https://academic.oup.com/schizophreniabulletin/article-lookup/doi/10.1093/schbul/sbv124.
Xin L, Mekle R, Fournier M, Baumann PS, Ferrari C, Alameda L, et al. Genetic polymorphism associated prefrontal glutathione and its coupling with brain glutamate and peripheral redox status in early psychosis. Schizophr Bull. 2016;42:1185–96. https://academic.oup.com/schizophreniabulletin/article-lookup/doi/10.1093/schbul/sbw038.
Smesny S, Gussew A, Biesel NJ, Schack S, Walther M, Rzanny R, et al. Glutamatergic dysfunction linked to energy and membrane lipid metabolism in frontal and anterior cingulate cortices of never treated first-episode schizophrenia patients. Schizophr Res. 2015; http://www.ncbi.nlm.nih.gov/pubmed/26255566. Accessed 11 Aug 2015.
Liemburg E, Sibeijn-Kuiper A, Bais L, Pijnenborg G, Knegtering H, van der Velde J, et al. Prefrontal NAA and Glx levels in different stages of psychotic disorders: a 3T 1H-MRS study. Sci Rep. 2016;6:21873 http://www.ncbi.nlm.nih.gov/pubmed/26903078.
Kegeles LS, Mao XL, Stanford AD, Girgis R, Ojeil N, Xu XY, et al. Elevated prefrontal cortex γ-aminobutyric acid and glutamate-glutamine levels in schizophrenia measured in vivo with proton magnetic resonance spectroscopy. Arch Gen Psychiatry. 2012;69:449–59. http://www.ncbi.nlm.nih.gov/pubmed/22213769.
Kim S-Y, Kaufman MJ, Cohen BM, Jensen JE, Coyle JT, Du F, et al. In vivo brain glycine and glutamate concentrations in patients with first-episode psychosis measured by echo time–averaged proton magnetic resonance spectroscopy at 4T. Biol Psychiatry. 2018;83:484–91. http://www.ncbi.nlm.nih.gov/pubmed/29031411.
Ongür D, Jensen JE, Prescot AP, Stork C, Lundy M, Cohen BM, et al. Abnormal glutamatergic neurotransmission and neuronal-glial interactions in acute mania. Biol Psychiatry. 2008;64:718–26. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2577764&tool=pmcentrez&rendertype=abstract.
Borgan FR, Jauhar S, McCutcheon RA, Pepper FS, Rogdaki M, Lythgoe DJ, et al. Glutamate levels in the anterior cingulate cortex in un-medicated first episode psychosis: a proton magnetic resonance spectroscopy study. Sci Rep. 2019;9:8685 http://www.nature.com/articles/s41598-019-45018-0.
Jauhar S, McCutcheon R, Borgan F, Veronese M, Nour M, Pepper F, et al. The relationship between cortical glutamate and striatal dopamine in first-episode psychosis: a cross-sectional multimodal PET and magnetic resonance spectroscopy imaging study. Lancet Psychiatry. 2018;5:816–23.
Dempster K, Jeon P, MacKinley M, Williamson P, Théberge J, Palaniyappan L. Early treatment response in first episode psychosis: a 7-T magnetic resonance spectroscopic study of glutathione and glutamate. Mol Psychiatry. 2020;25:1640–50.
Posporelis S, Coughlin JM, Marsman A, Pradhan S, Tanaka T, Wang H, et al. Decoupling of brain temperature and glutamate in recent onset of schizophrenia: a 7T proton magnetic resonance spectroscopy study. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3:248–54. https://linkinghub.elsevier.com/retrieve/pii/S2451902217300873.
Galińska B, Szulc A, Tarasów E, Kubas B, Dzienis W, Czernikiewicz A, et al. Duration of untreated psychosis and proton magnetic resonance spectroscopy (1H-MRS) findings in first-episode schizophrenia. Med Sci Monit. 2009;15:CR82–R88. http://www.medscimonit.com/abstract/index/idArt/869559.
Kegeles LS, Shungu DC, Anjilvel S, Chan S, Ellis SP, Xanthopoulos E, et al. Hippocampal pathology in schizophrenia: magnetic resonance imaging and spectroscopy studies. Psychiatry Res Neuroimaging. 2000;98:163–75. http://linkinghub.elsevier.com/retrieve/pii/S0925492700000445.
Szulc A, Galinska B, Tarasow E, Waszkiewicz N, Konarzewska B, Poplawska R, et al. Proton magnetic resonance spectroscopy study of brain metabolite changes after antipsychotic treatment. Pharmacopsychiatry. 2011;44:148–57. http://www.ncbi.nlm.nih.gov/pubmed/21710405.
Wood SJ, Berger GE, Wellard RM, Proffitt T, McConchie M, Velakoulis D, et al. A 1H-MRS investigation of the medial temporal lobe in antipsychotic-naïve and early-treated first episode psychosis. Schizophr Res. 2008;102:163–70. http://www.ncbi.nlm.nih.gov/pubmed/18456460.
Pillinger T, Rogdaki M, McCutcheon RA, Hathway P, Egerton A, Howes OD. Altered glutamatergic response and functional connectivity in treatment resistant schizophrenia: the effect of riluzole and therapeutic implications. Psychopharmacology. 2019;236:1985–97. http://link.springer.com/10.1007/s00213-019-5188-5.
McQueen G, Sendt K-V, Gillespie A, Avila A, Lally J, Vallianatou K, et al. Changes in brain glutamate on switching to clozapine in treatment-resistant schizophrenia. Schizophr Bull. 2021;47:662–71. https://academic.oup.com/schizophreniabulletin/article/47/3/662/6063097.
de la Fuente-Sandoval C, León-Ortiz P, Azcárraga M, Stephano S, Favila R, Díaz-Galvis L, et al. Glutamate levels in the associative striatum before and after 4 weeks of antipsychotic treatment in first-episode psychosis: a longitudinal proton magnetic resonance spectroscopy study. JAMA Psychiatry. 2013;70:1057–66. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3790718&tool=pmcentrez&rendertype=abstract.
Brouwer A, Luykx JJ, van Boxmeer L, Bakker SC, Kahn RS. NMDA-receptor coagonists in serum, plasma, and cerebrospinal fluid of schizophrenia patients: a meta-analysis of case–control studies. Neurosci Biobehav Rev. 2013;37:1587–96.
Martins-de-Souza D, Schmitt A, Röder R, Lebar M, Schneider-Axmann T, Falkai P, et al. Sex-specific proteome differences in the anterior cingulate cortex of schizophrenia. J Psychiatr Res. 2010;44:989–91.
Bristow GC, Bostrom JA, Haroutunian V, Sodhi MS. Sex differences in GABAergic gene expression occur in the anterior cingulate cortex in schizophrenia. Schizophr Res. 2015;167:57–63.
Weinberger DR, Radulescu E. Structural magnetic resonance imaging all over again. JAMA Psychiatry. 2021;78:11 https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2768031.
Merritt K, Perez-Iglesias R, Sendt K-V, Goozee R, Jauhar S, Pepper F, et al. Remission from antipsychotic treatment in first-episode psychosis related to longitudinal changes in brain glutamate. npj Schizophr. 2019;5:12.
Reyes-Madrigal F, Guma E, León-Ortiz P, Gómez-Cruz G, Mora-Durán R, Graff-Guerrero A, et al. Striatal glutamate, subcortical structure and clinical response to first-line treatment in first-episode psychosis patients. Prog Neuro-Psychopharmacol Biol Psychiatry. 2022;113:110473 https://linkinghub.elsevier.com/retrieve/pii/S0278584621002323.
Funding
This work was supported by MRC Grant Reference MR/S003436/1 (TD) and Medical Research Council grant MR/L003988/1 (AE). RM is funded by an NIHR clinical lectureship. OH is funded by Medical Research Council-UK (no. MC_A656_5QD30_2135), Maudsley Charity (no. 666), and Wellcome Trust (no. 094849/Z/10/Z). This study presents independent research funded in part by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley National Health Service (NHS) Foundation Trust and King’s College London.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
RM has received honoraria for talks from Otsuka and Janssen. OH is a part-time employee and stock holder of Lundbeck A/s. He has received investigator-initiated research funding from and/or participated in advisory/speaker meetings organised by Angellini, Autifony, Biogen, Boehringer-Ingelheim, Eli Lilly, Heptares, Global Medical Education, Invicro, Jansenn, Lundbeck, Neurocrine, Otsuka, Sunovion, Recordati, Roche and Viatris/Mylan. OH has a patent for the use of dopaminergic imaging.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Merritt, K., McCutcheon, R.A., Aleman, A. et al. Variability and magnitude of brain glutamate levels in schizophrenia: a meta and mega-analysis. Mol Psychiatry 28, 2039–2048 (2023). https://doi.org/10.1038/s41380-023-01991-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41380-023-01991-7
This article is cited by
-
Longitudinal trajectories of anterior cingulate glutamate and subclinical psychotic experiences in early adolescence: the impact of bullying victimization
Molecular Psychiatry (2024)
-
Schizophrenia: from neurochemistry to circuits, symptoms and treatments
Nature Reviews Neurology (2024)
-
Psychosis and autism spectrum disorder: a special issue of Molecular Psychiatry
Molecular Psychiatry (2023)
