
Abstract
Objective
To describe outcomes for infants in the neonatal intensive care unit with septic shock based on the vasopressor administered.
Methods
This is a multicenter cohort study of infants with an episode of septic shock. We evaluated the primary outcomes of mortality and pressor-free days alive in the first week after shock using multivariable logistic and Poisson regressions.
Results
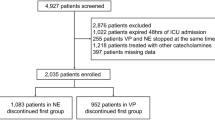
We identified 1592 infants. Mortality was 50%. Dopamine was the most used vasopressor (92% of episodes) and hydrocortisone was co-administered with a vasopressor in 38% of episodes. Compared to infants treated with dopamine alone, adjusted odds of mortality were significantly higher for those treated with epinephrine alone (aOR 4.7 [95% CI: 2.3–9.2]). Adjuvant hydrocortisone was associated with significantly lower adjusted odds of mortality (aOR 0.60 [0.42–0.86])
Conclusions
The use of epinephrine as either a solo agent or in combination therapy was associated with significantly worse outcomes, while adjuvant hydrocortisone was associated with decreased mortality.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
The computer code and Stata do-files used to generate the results of the manuscript are available from the corresponding author on reasonable request.
References
Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA. 2015;314:1039–51.
Cailes B, Kortsalioudaki C, Buttery J, Pattnayak S, Greenough A, Matthes J, et al. Epidemiology of UK neonatal infections: the neonIN infection surveillance network. Arch Dis Child Fetal Neonatal Ed. 2018;103:F547–53.
Wynn JL, Wong HR. Pathophysiology and treatment of septic shock in neonates. Clin Perinatol. 2010;37:439–79.
Burns ML, Stensvold HJ, Risnes K, Guthe HJ, Astrup H, Nordhov SM, et al. Inotropic therapy in newborns, a population-based national registry study. Pediatr Crit Care Med. 2016;17:948–56.
Tsai M-H, Hsu J-F, Chu S-M, Lien R, Huang H-R, Chiang M-C, et al. Incidence, clinical characteristics and risk factors for adverse outcome in neonates with late-onset sepsis. Pediatr Infect Dis J. 2014;33:e7–13.
McGovern M, Giannoni E, Kuester H, Turner MA, van den Hoogen A, Bliss JM, et al. Challenges in developing a consensus definition of neonatal sepsis. Pediatr Res. 2020;88:14–26.
Verstraete E, Boelens J, De Coen K, Claeys G, Vogelaers D, Vanhaesebrouck P, et al. Healthcare-associated bloodstream infections in a neonatal intensive care unit over a 20-year period (1992-2011): trends in incidence, pathogens, and mortality. Infect Control Hosp Epidemiol. 2014;35:511–8.
Fleiss N, Coggins SA, Lewis AN, Zeigler A, Cooksey KE, Walker LA, et al. Evaluation of the neonatal sequential organ failure assessment and mortality risk in preterm infants with late-onset infection. JAMA Netw Open. 2021;4:e2036518.
Baske K, Saini SS, Dutta S, Sundaram V. Epinephrine versus dopamine in neonatal septic shock: a double-blind randomized controlled trial. Eur J Pediatr. 2018;177:1335–42.
Kermorvant-Duchemin E, Laborie S, Rabilloud M, Lapillonne A, Claris O. Outcome and prognostic factors in neonates with septic shock. Pediatr Crit Care Med. 2008;9:186–91.
Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med. 2020;46:10–67.
Ventura AMC, Shieh HH, Bousso A, Goes PF, Fernandes ICFO, de Souza DC, et al. Double-blind prospective randomized controlled trial of dopamine versus epinephrine as first-line vasoactive drugs in pediatric septic shock. Crit Care Med. 2015;43:2292–302.
Ramaswamy KN, Singhi S, Jayashree M, Bansal A, Nallasamy K. Double-blind randomized clinical trial comparing dopamine and epinephrine in pediatric fluid-refractory hypotensive septic shock. Pediatr Crit Care Med. 2016;17:e502–12.
Kharrat A, Jain A. Hemodynamic dysfunction in neonatal sepsis. Pediatr Res. 2022;91:413–24.
Miller LE, Laughon MM, Clark RH, Zimmerman KO, Hornik CP, Aleem S, et al. Vasoactive medications in extremely low gestational age neonates during the first postnatal week. J Perinatol. 2021;41:2330–6.
Spitzer AR, Ellsbury DL, Handler D, Clark RH. The Pediatrix BabySteps Data Warehouse and the Pediatrix QualitySteps improvement project system—tools for “meaningful use” in continuous quality improvement. Clin Perinatol. 2010;37:49–70.
Wynn JL, Polin RA. A neonatal sequential organ failure assessment score predicts mortality to late-onset sepsis in preterm very low birth weight infants. Pediatr Res. 2020;88:85–90.
Sassano-Higgins S, Friedlich P, Seri I. A meta-analysis of dopamine use in hypotensive preterm infants: blood pressure and cerebral hemodynamics. J Perinatol. 2011;31:647–55.
Valverde E, Pellicer A, Madero R, Elorza D, Quero J, Cabañas F. Dopamine versus epinephrine for cardiovascular support in low birth weight infants: analysis of systemic effects and neonatal clinical outcomes. Pediatrics. 2006;117:e1213–22.
Osborn D, Evans N, Kluckow M. Randomized trial of dobutamine versus dopamine in preterm infants with low systemic blood flow. J Pediatr. 2002;140:183–91.
Osborn DA, Paradisis M, Evans N. The effect of inotropes on morbidity and mortality in preterm infants with low systemic or organ blood flow. Cochrane Database Syst Rev. 2007;2007:CD005090.
Zimmerman K, Gonzalez D, Swamy GK, Cohen-Wolkowiez M. Pharmacologic studies in vulnerable populations: using the pediatric experience. Semin Perinatol. 2015;39:532–6.
Ibrahim H, Sinha IP, Subhedar NV. Corticosteroids for treating hypotension in preterm infants. Cochrane Database Syst Rev. 2011;2011:CD003662.
Crouchley JL, Smith PB, Cotton CM, Hornik CD, Goldberg RN, Foreman JW, et al. Effects of low-dose dopamine on urine output in normotensive very low birth weight neonates. J Perinatol. 2013;33:619–21.
Schmatz M, Srinivasan L, Grundmeier RW, Elci OU, Weiss SL, Masino AJ, et al. Surviving sepsis in a referral neonatal intensive care unit: association between time to antibiotic administration and in-hospital outcomes. J Pediatr. 2020;217:59–65.e1.
Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–96.
Acknowledgements
Erin Campbell, MS, provided editorial review and manuscript submission. Erin Campbell did not receive compensation for her assistance, apart from her employment at the institution where this research was conducted. Carol Hill, PhD, provided informatics assistance with data procurement from Pediatrix. The authors would like to thank Duke Pediatric Research Scholars.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data. HPF drafted the work, all authors revised it critically for important intellectual content. All authors approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
RGG received support from the industry for research services (https://dcri.org/about-us/conflict-of-interest/). The authors have no other conflicts of interest relevant to this article to disclose.
Ethics approval and consent to participate
We obtained institutional review board approval from the Duke University Health System IRB with a waiver of informed consent for our study, protocol Pro00112607. The study was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Foote, H.P., Benjamin, D.K., Greenberg, R.G. et al. Use of vasopressors for septic shock in the neonatal intensive care unit. J Perinatol 43, 1274–1280 (2023). https://doi.org/10.1038/s41372-023-01667-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-023-01667-8
