
Abstract
Objective
To examine associations between maternal mental health and involvement in developmental care in the NICU.
Study design
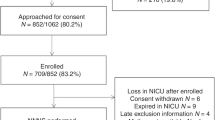
Mothers of infants born <32 weeks gestation (n = 135) were approached to complete mental health screening questionnaires at two weeks after admission. Mothers who completed screening (n = 55) were further classified as with (n = 19) and without (n = 36) elevated scores. Mothers’ frequency, rate, and duration of developmental care activities were documented in the electronic health record.
Results
35% of screened mothers scored above the cutoff for clinical concern on ≥1 measure. No significant differences between the 3 groups were identified for rates, frequency, or amount of all developmental care, kangaroo care, and swaddled holding.
Conclusion
Elevated scores on maternal mental health questionnaires did not relate to developmental care. Maternal developmental care engagement may not indicate mental health status. Universal screening for psychological distress is required to accurately detect symptoms in mothers of hospitalized preterm infants.
Similar content being viewed by others


Introduction
Developmental care, which includes parent involvement in activities such as kangaroo care, positive touch, massage, and auditory exposures, for preterm infants in the neonatal intensive care unit is important to mother-infant attachment [1,2,3,4,5,6] and to infant health outcomes [7]. Mothers of preterm-born infants are at elevated risk for postpartum depression, anxiety disorders, and symptoms of post-traumatic stress [8,9,10,11,12]. These maternal mental health conditions influence mother-infant attachment [13, 14], increasing the risk of maladaptive family dynamics such as vulnerable child syndrome [15]. Maternal mental health is an important factor associated with many childhood outcomes, including physical growth, childhood illness, cognitive development, and academic achievement [3]. Studies have yet to examine potential links between mental health conditions and maternal engagement in developmental care activities.
Developmental care practices in the neonatal intensive care unit have been used to assist parents in developing a healthy attachment with their critically ill infants [16, 17]. Despite comprehensive and well-documented developmental care programs, wide variation exists in the actual parent and infant experience of these developmental care practices [18,19,20]. Institutional, socio-demographic, and infant factors are known to influence developmental care implementation [21,22,23,24]. In this investigation, we ask whether maternal mental health is associated with variation in developmental care practices. We hypothesized that mothers who screened positive for symptoms of psychological distress would participate in fewer developmental care activities overall. We base this hypothesis on research that depressed mothers have a heightened risk of impaired infant bonding [25,26,27,28] and may have altered caregiving behaviors [8, 29,30,31].
Subjects and methods
Participants
Participants in this retrospective study were all mothers and their infants (n = 135) who were born very or extremely preterm (≤31 6/7 weeks gestational age, GA) between 5/1/2018 and 2/9/2020. All infants were cared for at Lucile Packard Children’s Hospital (LPCH) from admission through at least 35 weeks post-menstrual age. We included infants born at other hospitals (n = 19) only if they had been transferred into the LPCH neonatal intensive care unit (NICU) before 7 days of life. We chose this criterion to ensure reliable characterization of their developmental care experience for the duration of hospitalization for preterm birth. LPCH nursing education includes training for developmental care charting. Nurses routinely chart all visitation and developmental care activities (e.g., kangaroo care, swaddled holding, massage) in the electronic medical record (EMR). We excluded infants born after 2/9/2020 because of changes in hospital visitation policies that were instituted on 3/8/2020 due to the SARS-CoV2 pandemic. This cut-off date ensured that all infants experienced at least 1 month of their hospital course during the pre-pandemic period. The Stanford University Institutional Review Board approved the experimental protocol (#IRB-54650). All data were collected in the course of routine clinical care. Participants were not required to give consent for this retrospective analysis. The study was performed in accordance with the Declaration of Helsinki.
Infant and maternal characteristics were extracted from the EMR. Infant characteristics included child sex, gestational age at birth, gestational age at admission, part of a multiple birth, and length of stay. We also tallied the presence/absence of common clinical conditions and treatment that may influence the receipt of developmental care, including bronchopulmonary dysplasia, necrotizing enterocolitis, intraventricular hemorrhage, and sepsis. We calculated a summary health acuity score as the sum of the presence of these four clinical conditions, grouping infants into those with none versus those with one or more of these conditions. Maternal characteristics included maternal age at delivery, delivery type (vaginal or cesarean section), and health insurance type (public vs. private). We previously reported that non-English speaking mothers in our NICU have lower rates of kangaroo care than English-speaking mothers [18], therefore we also collected information on maternal language preference.
Maternal Mental Health Assessment
All mothers of infants were offered mental health services approximately 2 weeks after admission. Mothers who accepted met with a NICU clinical psychologist or social worker and completed three validated mental health screening measures of psychological distress. The Patient Health Questionnaire (PHQ-9) screens for depression and consists of nine prompts asking about the frequency of symptoms over the past two weeks (e.g., “Little interest or pleasure in doing things”) to which patients responded from “not at all” to “nearly every day” [32]. The possible score range is 0-27; scores >15 were considered clinically elevated. The Neuro-QoL Short Form v1.0-Anxiety (NQOL – www.neuroqol.org) consists of eight prompts about unpleasant thoughts and/or feelings related to fear, helplessness, worry and hyperarousal (e.g., “I felt uneasy”) scored from 1-5 (“never” to “always”) [33]. The possible range is 8-40, with > 26 considered clinically elevated. The Perinatal Post Traumatic Stress Disorder Questionnaire (PPQ) consists of 14 questions asking about reactions to their infant’s birth (e.g., “Did you have bad dreams of giving birth or of your baby’s hospital stay?”), scored from 0-4 (“not at all” to “often, for more than a month”) [34]. The possible range is 0-56, with scores > 19 considered clinically elevated. Mothers who scored in the clinically elevated range on any of the questionnaires were counseled by the clinical psychologist and referred to hospital or community resources for further assessment and symptom management.
Of the 135 infant-mother dyads, 55 (41%) completed the mental health screening questionnaires. For analyses, we grouped mothers who participated in the screening into two cohorts based on whether they scored in the clinically elevated range on one or more of the assessments: clinically elevated (n = 19) and not-clinically elevated (n = 36). All mothers who participated in the screening completed all three questionnaires. Non-screened mothers were those mothers who did not complete the screening (n = 80). Ten (18%) scored above the cutoff of the PHQ-9 depression screener, 17 (31%) scored above the cutoff on the NQOL anxiety screener, and 11 (20%) scored above the cutoff on the PTSD screener. Of the 19 scoring above the cutoff, 8 scored in the range of concern on one screen, 3 on 2 screeners, and 8 on all three screeners.
Developmental Care
As part of routine charting, nurses documented each instance of any developmental care activities including the type (Kangaroo Care, Swaddled Holding, Touch, Massage, Music, Talking, and Singing), the approximate duration, and who was involved (mother, father, other family members, nurse, other staff members, or any combination of these). For the purposes of these analyses, we restricted our computation to only those developmental care instances when the mother participated, either alone or with staff or other family members. A summary measure of all developmental care was generated by summing all instances of any type in which the mother was reported to be present. We secondarily assessed two individual developmental care practices, kangaroo care, and swaddled holding. Kangaroo care, also referred to as skin-to-skin holding, has been used as a therapeutic intervention for mood disorders in the NICU [35,36,37]. As infants grow and are better able to maintain body temperature and physiologic stability outside an isolette, kangaroo care may be replaced by swaddled holding. For these individual care practices, we again only count those instances in which the mother was present either alone or together with staff or other family member(s).
Three measures were calculated for each developmental care type:
-
(a)
Frequency = total number of instances of developmental care/total length of stay (instances/day)
-
(b)
Rate = total time performing developmental care activity/total length of stay (minutes/day)
-
(c)
Duration = total time performing developmental care activity/total number of instances of developmental care (minutes/instance). Note: Duration values were missing for those mothers who had no developmental care instances overall and for that activity.
Statistical approach
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS version 28.0, IBM Corp., 2021). Two-sided statistical significance was set at p < 0.05. Based on normality, we used parametric t-tests or ANOVAs for assessing group differences in continuous variables and Chi-square tests for group differences in dichotomous variables. Post-hoc tests evaluated sub-group differences by applying Tukey correction.
Results
Table 1 shows the demographic and clinical characteristics of the infants and mothers. The distribution of female to male infants was similar across all three groups of infants (χ2 = 0.63, p = 0.73). Infants who were part of a multiple birth were more likely to be in the non-screened group than the screened non-clinically-elevated or clinically-elevated groups (p = 0.05). Critically, there were no differences in the frequency of infants from multiple births in the non-clinically-elevated vs. clinically-elevated groups (p = 0.29). There were no group differences in the age of admission to the NICU, F(2, 132) = 0.30, p = 0.75, however, there was a significant group difference in GA at birth, F(2132) = 6.9, p < 0.001, such that the infants of the non-screened mothers were significantly older at birth than those in the screened non-clinically elevated group (p = 0.03) and the screened clinically-elevated group (p = 0.004). Post-hoc comparisons indicated that infants of mothers in the two screened groups were not significantly different in GA at birth (p = 0.51). In addition, length of stay was significantly different across the three groups, F(2, 132) = 5.6, p = 0.005, with those infants in the screened clinically-elevated group staying in the hospital significantly longer than infants in the non-screened group (p = 0.01). Post-hoc comparisons further indicated that there was no significant difference in length of stay between the screened clinically-elevated and screened not clinically-elevated groups (p = 0.55). While there was a trend for a higher proportion of infants with one or more medical complications in the screened groups, this difference did not achieve significance (p = 0.13). There were no group differences in maternal age (p = 0.29), nor in the frequency of cesarean mode of delivery (p = 0.60), public (vs. private) insurance (p = 0.85), or non-English preferred language (p = 0.99).
Table 2 shows descriptive and inferential statistics in frequency, rate, and duration of developmental care activities by the group. These analyses indicated that mothers in all groups engaged in developmental care activities just over once per day, on average, with no significant group differences in the frequency of developmental care activities. The pattern of similar levels of developmental care activities did not change even when controlling for GA at birth and length of stay, F(2, 130) = 0.34, p = 0.72. Table 2 also shows that infants in all groups engaged in just over 60 minutes/day of developmental care, on average, with each developmental care instance lasting about 51 minutes/instance, with no significant group differences. We also found no evidence for group differences in the frequency F(2,130) = 0.34, p = 0.72, rate, F(2, 130) = 0.23, p = 0.80, or duration, F(2,129) = 0.34, p = 0.71, of all maternal developmental care activities, even when controlling for GA and length of stay. Because we were specifically interested in differences between those mothers who scored as elevated on one or more of the screening measures versus those who did not, comparisons of screened groups showed no significant differences in frequency (p = 0.65), rate (p = 0.68), or duration (p = 0.55) of developmental care activities, even after controlling GA and length of stay (all p > 0.57).
While there were no significant group differences in all developmental care activities, it is possible that maternal mental health status may have moderated participation in specific activities, such as kangaroo care and swaddled holding. Table 2 also reports the descriptive and inferential statistics for these types of developmental care activities. The frequency, rate, and duration of kangaroo care and swaddled holding activities were similar across the groups with no statistically significant group differences in any measure. Again, post-hoc comparisons specifically showed no group differences between those mothers with clinically-elevated scores vs. those screened mothers with non-clinically-elevated scores in frequency (kangaroo care: p = 0.91, holding: p = 0.99), rate (kangaroo care: p = 0.78, holding: p = 0.99) or duration (kangaroo care: p = 0.37, holding: p = 0.86) of care. We also evaluated group differences in rates of these specific developmental care activities, controlling for GA and length of stay, factors that may have affected rates of developmental care. The addition of the covariates did not change the pattern of the results for either kangaroo care (all p > 0.27) or swaddled holding (all p > 0.79).
Finally, it is possible that group differences in developmental care activities would be observed depending on the number or type of screeners on which mothers scored in the clinically-elevated range. Thus, we explored whether measures of developmental care activities were different in those screened mothers who scored in the clinically-elevated range on only one (n = 8) versus on two or more (n = 11) of the screeners. No group differences were observed when considering all developmental care activities (all p > 0.90) or specifically kangaroo care (all p > 0.43) or swaddled holding (all p > 0.66). In addition, no group differences on any measure of developmental care were observed in those screened mothers who scored in the non-clinically-elevated versus clinically-elevated range on depression (n = 10; all p > 0.47), anxiety, (n = 17, all p > 0.31), and PTSD (n = 11; all p > 0.32).
Discussion
In this investigation of mothers of infants born very or extremely preterm, we found that the number of developmental care activities performed by mothers did not differ between mothers with or without clinically elevated self-report of symptoms of depression, anxiety, or PTSD symptoms. No differences were found in the rate (total minutes of developmental care activities per day), nor in the frequency or duration of all developmental care activities and of kangaroo care or holding practices alone. Furthermore, we found no differences in the amounts of developmental care activities performed by mothers who had or had not accepted to participate in mental health screening.
These findings were contrary to our initial hypothesis that mothers with clinically significant mental health concerns would engage in less developmental care. While there is an established relation between maternal mental health and mother-infant interactions and engagement in preterm mother-infant dyads post-discharge [13, 25, 26, 28], maternal mental health may not have the same salience in the NICU environment where parents benefit from a more intensive structure and support for parenting activities. Parenting activities in the NICU may be more tightly guided by unit policies, infant health and support needs, and infant maturity levels. In addition, parents receive daily prompting from the healthcare team to engage in specific practices so may be less able to adjust activity levels depending on mental health. Moreover, all mothers who scored above clinical thresholds were offered mental health services which likely included encouragement to participate in developmental care activities, making these activities a conscious therapeutic act rather than part of routine care. Note that all of these factors are specific to the NICU experience and therefore our results may not be generalizable to other contexts, such as the home environment. Future research should also investigate possible long-term and cumulative sequelae of maternal psychological distress during the neonatal period on maternal engagement after discharge to home.
Kangaroo care specifically has been associated with improved maternal mood [35,36,37] and has been studied as a mental health intervention [38]. In this sample, mothers with clinically elevated symptomatology did no more kangaroo care than those without clinically elevated scores. Finally, other factors may be more powerful drivers of developmental care in the NICU, overwhelming the impact of symptoms of maternal psychological distress. For instance, in our previous research, we found that lower socioeconomic status or being of lower English proficiency was significantly associated with reduced amounts of developmental care activity among parents [18]. Factors such as developmental care policies, psychological support services for parents, and equal access to developmental care education and engagement may provide more important modifiable avenues to improve rates of developmental care.
The present study provides novel evidence that elevated scores on screening measures of maternal psychological distress may not significantly contribute to variation in the total rates, frequency, and duration of developmental care experienced by preterm infants in the NICU. Clinicians and staff caring for preterm infants and their families should take caution - maternal engagement in developmental care activities with their infants is not a marker for maternal mood and well-being. One might imagine that a particularly anxious mother might visit her infant more or that a mother with many depressive symptoms might engage less, but these would be misattributions. Our analysis suggests that maternal participation in developmental care activities does not indicate the presence or absence of significant maternal distress. This analysis contributes to the body of evidence for instituting universal screening for mood disorders among mothers of preterm-born infants with appropriate referral and management supports.
It is worth noting that levels of developmental care involvement in this study are similar to those found in other NICUs in the United States [21] and are relatively low compared with those documented in other countries, particularly those using a more family-integrated care model [39, 40]. While correlations may not exist between maternal mood and developmental care in United States NICUs, future studies should explore associations in NICUs with a higher baseline of parent involvement or a larger range of participation. It is possible that in those settings differences may be detected which may further support social structures which encourage and enforce the parental role as key to NICU infant care.
The current research also points to further research into parent-infant bonding and the impact both participation in developmental care activities and parental mental health status might play in mediating and moderating relations between parent-infant bonding and infant mental health outcomes. Parent-infant bonding at the time of NICU discharge has been shown to positively correlate with long term cognitive outcomes in preterm infants [3]. Targeted interventions to improve the parent-infant relationship have included engagement in developmental care with documented health benefits for infants and parents [41, 42]. These studies indicate that bonding is a core component of NICU family care [20]. Formal screening for bonding is rare outside of the research setting but may be an important additional avenue for future investigation.
The study had limitations. The data were extracted and analyzed from EMRs and clinical psychologists who administered the screening measures and thus may capture inconsistencies in reporting from clinical staff. The sample was not large enough to delve into the timing of developmental care activities or to examine developmental activities before and after the screening. The sample was also not large enough to evaluate the influence of multiple births on developmental care activities or maternal mood. The study did not include information about the quality of interactions which may be an even more important indicator of parent-infant attachment and the quality of caregiving behaviors [43,44,45]. There is no follow-up data on the initial screening tools to identify the trajectory of symptoms of psychological distress and whether improvement in symptoms was associated with developmental care activities. Our measures of maternal mood were self-report questionnaires, and we did not have clinician evaluation with medical diagnoses. Finally, there is limited information on mothers who did not complete screening measures, limiting generalizability of our results. For instance, some non-screened mothers may have declined because they were already receiving mental health services. All of these limitations offer opportunities for further research regarding the interaction between parental mood and infant caregiving in the NICU.
In summary, there were no significant relationships between clinically elevated scores on maternal mental health screener and rates, frequency, and duration of developmental care activities. This finding suggests that parental engagement in developmental care activities may not serve as an indicator of mental health. While maternal mental health variables may not contribute significantly to variation in developmental care activities, high rates of parental psychological distress exist in the NICU family population and negative associations have been well documented between poor parental mental health and future neurodevelopmental outcomes in NICU infants [3, 8,9,10]. As such, perinatal maternal mood screeners should be implemented in infant healthcare environments and longitudinally following NICU discharge, to gauge parental mental health in the acute setting and over time. Consideration should be given to serial screening, including after discharge as NICU parent mental health is a dynamic condition. Further research should be conducted to determine how engagement in NICU developmental care practices may affect parenting behaviors, including parent-infant dyad engagement, after hospital discharge.
Data availability
Deidentified Data will be made available upon reasonable request.
References
Feldman R, Weller A, Leckman JF, Kuint J, Eidelman AI. The nature of the mother’s tie to her infant: maternal bonding under conditions of proximity, separation, and potential loss. J Child Psychol Psychiatry. 1999;40:929–39.
Pennestri MH, Gaudreau H, Bouvette-Turcot AA, Moss E, Lecompte V, Atkinson L, et al. Attachment disorganization among children in Neonatal Intensive Care Unit: Preliminary results. Early Hum Dev. 2015;91:601–6.
Breeman LD, Jaekel J, Baumann N, Bartmann P, Wolke D. Neonatal predictors of cognitive ability in adults born very preterm: a prospective cohort study. Dev Med Child Neurol. 2017;59:477–83.
Yui Y, October TW. Parental perspectives on the postpartum bonding experience after neonatal intensive care unit transfer to a referral hospital. Am J Perinatol. 2021;38:1358–65.
Fernández Medina IM, Granero-Molina J, Fernández-Sola C, Hernández-Padilla JM, Camacho Ávila M, López Rodríguez MDM. Bonding in neonatal intensive care units: Experiences of extremely preterm infants’ mothers. Women Birth. 2018;31:325–30.
Fegran L, Helseth S, Fagermoen MS. A comparison of mothers’ and fathers’ experiences of the attachment process in a neonatal intensive care unit. J Clin Nurs. 2008;17:810–6.
Pineda R, Guth R, Herring A, Reynolds L, Oberle S, Smith J. Enhancing sensory experiences for very preterm infants in the NICU: an integrative review. J Perinatol. 2017;37:323–32.
Forcada-Guex M, Borghini A, Pierrehumbert B, Ansermet F, Muller-Nix C. Prematurity, maternal posttraumatic stress and consequences on the mother-infant relationship. Early Hum Dev. 2011;87:21–6.
Helle N, Barkmann C, Ehrhardt S, von der Wense A, Nestoriuc Y, Bindt C. Postpartum anxiety and adjustment disorders in parents of infants with very low birth weight: Cross-sectional results from a controlled multicentre cohort study. J Affect Disord. 2016;194:128–34.
Khoramirad A, Abedini Z, Khalajinia Z. Relationship between mindfulness and maternal stress and mother – Infant bonding in neonatal intensive care unit. J Educ Health Promot. 2021;10:337.
Lee CK, Huang XY. Psychological processes of postpartum mothers with newborns admitted to the intensive care unit. Asian Nurs Res (Korean Soc Nurs Sci). 2022;16:9–17.
Lefkowitz DS, Baxt C, Evans JR. Prevalence and correlates of posttraumatic stress and postpartum depression in parents of infants in the Neonatal Intensive Care Unit (NICU). J Clin Psychol Med Settings. 2010;17:230–7.
Singer LT, Fulton S, Davillier M, Koshy D, Salvator A, Baley JE. Effects of infant risk status and maternal psychological distress on maternal-infant interactions during the first year of life. J Dev Behav Pediatr. 2003;24:233–41.
Korja R, Savonlahti E, Ahlqvist-Björkroth S, Stolt S, Haataja L, Lapinleimu H, et al. Maternal depression is associated with mother–infant interaction in preterm infants. Acta Paediatr. 2008;97:724–30.
Schmitz K. Vulnerable Child Syndrome. Pediatr Rev. 2019;40:313–5.
Cho ES, Kim SJ, Kwon MS, Cho H, Kim EH, Jun EM, et al. The effects of Kangaroo Care in the neonatal intensive care unit on the physiological functions of preterm infants, maternal-infant attachment, and maternal stress. J Pediatr Nurs. 2016;31:430–8.
Conde-Agudelo A, Díaz-Rossello JL. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst Rev. 2014; CD002771.
Brignoni-Pérez E, Scala M, Feldman HM, Marchman VA, Travis KE. Disparities in Kangaroo care for premature infants in the neonatal intensive care unit. J Dev Behav Pediatr. 2021;43:e304–e311.
Scala M, Marchman VA, Brignoni-Pérez E, Morales MC, Dubner SE, Travis KE. Impact of the COVID-19 pandemic on developmental care practices for infants born preterm. Early Hum Dev. 2021;163:105483.
Givrad S, Hartzell G, Scala M. Promoting infant mental health in the neonatal intensive care unit (NICU): A review of nurturing factors and interventions for NICU infant-parent relationships. Early Hum Dev. 2021;154:105281.
Pineda R, Bender J, Hall B, Shabosky L, Annecca A, Smith J. Parent participation in the neonatal intensive care unit: Predictors and relationships to neurobehavior and developmental outcomes. Early Hum Dev. 2018;117:32–8.
Saltzmann AM, Sigurdson K, Scala M. Barriers to Kangaroo Care in the NICU: A qualitative study analyzing parent survey responses. Adv Neonatal Care. 2022;22:261–9.
Fluharty M, Nemeth LS, Logan A, Nichols M. What do neonatal intensive care unit policies tell us about kangaroo care implementation? A realist review. Adv Neonatal Care. 2021;21:E76–85.
Lewis TP, Andrews KG, Shenberger E, Betancourt TS, Fink G, Pereira S, et al. Caregiving can be costly: A qualitative study of barriers and facilitators to conducting kangaroo mother care in a US tertiary hospital neonatal intensive care unit. BMC Pregnancy Childbirth. 2019;19:227.
Dubber S, Reck C, Müller M, Gawlik S. Postpartum bonding: the role of perinatal depression, anxiety and maternal-fetal bonding during pregnancy. Arch Women’s Ment Health. 2015;18:187–95.
Tietz A, Zietlow AL, Reck C. Maternal bonding in mothers with postpartum anxiety disorder: the crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch Women’s Ment Health. 2014;17:433–42.
Reck C, Noe D, Gerstenlauer J, Stehle E. Effects of postpartum anxiety disorders and depression on maternal self-confidence. Infant Behav Dev. 2012;35:264–72.
Moehler E, Brunner R, Wiebel A, Reck C, Resch F. Maternal depressive symptoms in the postnatal period are associated with long-term impairment of mother-child bonding. Arch Women’s Ment Health. 2006;9:273–8.
Beebe B, Lachmann F, Jaffe J, Markese S, Buck KA, Chen H, et al. Maternal postpartum depressive symptoms and 4-month mother–infant interaction. Psychoanal Psychol. 2012;29:383–407.
Herrera E, Reissland N, Shepherd J. Maternal touch and maternal child-directed speech: effects of depressed mood in the postnatal period. J Affect Disord. 2004;81:29–39.
Field T. Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behav Dev. 2010;33:1–6.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16:606–13.
Cella D, Lai JS, Nowinski CJ, Victorson D, Peterman A, Miller D, et al. Neuro-QOL. Neurology 2012;78:1860–7.
Callahan JL, Borja SE, Hynan MT. Modification of the Perinatal PTSD Questionnaire to enhance clinical utility. J Perinatol. 2006;26:533–9.
de Macedo EC, Cruvinel F, Lukasova K, D’Antino MEF. The mood variation in mothers of preterm infants in Kangaroo mother care and conventional incubator care. J Trop Pediatr. 2007;53:344–6.
Feldman R, Eidelman AI, Sirota L, Weller A. Comparison of Skin-to-Skin (Kangaroo) and traditional care: Parenting outcomes and preterm infant development. Pediatrics 2002;110:16–26.
Tallandini MA, Scalembra C. Kangaroo mother care and mother-premature infant dyadic interaction. Infant Ment Health J 2006;27:251–75.
Kirca N, Adibelli D. Effects of mother-infant skin-to-skin contact on postpartum depression: A systematic review. Perspect Psychiatr Care. 2021;57:2014–23.
Raiskila S, Axelin A, Toome L, Caballero S, Tandberg BS, Montirosso R, et al. Parents’ presence and parent-infant closeness in 11 neonatal intensive care units in six European countries vary between and within the countries. Acta Paediatr. 2017;106:878–88.
Blomqvist YT, Ewald U, Gradin M, Nyqvist KH, Rubertsson C. Initiation and extent of skin-to-skin care at two Swedish neonatal intensive care units. Acta Paediatr. 2013;102:22–8.
Welch MG, Halperin MS, Austin J, Stark RI, Hofer MA, Hane AA, et al. Depression and anxiety symptoms of mothers of preterm infants are decreased at 4 months corrected age with Family Nurture Intervention in the NICU. Arch Women’s Ment Health. 2016;19:51–61.
Welch MG, Firestein MR, Austin J, Hane AA, Stark RI, Hofer MA, et al. Family Nurture Intervention in the Neonatal Intensive Care Unit improves social-relatedness, attention, and neurodevelopment of preterm infants at 18 months in a randomized controlled trial. J Child Psychol Psychiatry. 2015;56:1202–11.
Poehlmann J, Fiese BH. Parent-infant interaction as a mediator of the relation between neonatal risk status and 12-month cognitive development1 1The first edition of the Bayley was used because the initial wave of data collection was initiated just prior to distribution of the second edition. Infant Behav Dev. 2001;24:171–88.
Gerstein ED, Poehlmann-Tynan J, Clark R. Mother–Child Interactions in the NICU: Relevance and Implications for Later Parenting. J Pediatr Psychol. 2015;40:33–44.
Treyvaud K, Anderson VA, Howard K, Bear M, Hunt RW, Doyle LW, et al. Parenting behavior is associated with the early neurobehavioral development of very preterm children. Pediatrics 2009;123:555–61.
Acknowledgements
The authors would like to thank the NICU nurses, clinical psychologists, and clinical research coordinator, Molly Fradin Lazarus, for their contributions to data collection. We thank the parents and families of the LPCH NICU for their generous participation in this study.
Funding
All phases of this study were supported by the Stanford University 2019 Department of Psychiatry & Behavioral Sciences Innovator Grants (R. J. Shaw, PI) and the National Institutes of Health- Eunice Kennedy Shriver National Institute of Child Health and Human Development (K.E. Travis, PI; 5R00HD8474904; H.M. Feldman, PI; 2RO1- HD069150).
Author information
Authors and Affiliations
Contributions
SED contributed to data acquisition and data interpretation and drafted the manuscript. MCM performed initial data analyses and drafted the manuscript. VAM performed data analysis and data interpretation and revised the manuscript for important intellectual content. RS contributed to the conception and design of the study, data acquisition, and reviewed the manuscript critically for important intellectual content. KET contributed to study design, data acquisition, and data interpretation, and reviewed the manuscript for critically important intellectual content. MS conceptualized the study, contributed to interpretation of the data, and reviewed the manuscript for critically important intellectual content. All authors approve the final version of the manuscript and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The Stanford University Institutional Review Board approved the experimental protocol (#IRB-54650). All data were collected in the course of routine clinical care. Participants were not required to give consent for this retrospective analysis. The study was performed in accordance with the Declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dubner, S.E., Morales, M.C., Marchman, V.A. et al. Maternal mental health and engagement in developmental care activities with preterm infants in the NICU. J Perinatol 43, 871–876 (2023). https://doi.org/10.1038/s41372-023-01661-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-023-01661-0
This article is cited by
-
Outcomes assessments should reflect the dynamic and contextual nature of early childhood development
Pediatric Research (2023)
