
Abstract
Background
Excess abdominal visceral adipose tissue (VAT) is associated with metabolic diseases and poor survival in colon cancer (CC). We assessed the impact of different types of CC surgery on changes in abdominal fat depots.
Material and methods
Computed tomography (CT)-scans performed preoperative and 3 years after CC surgery were analyzed at L3-level for VAT, subcutaneous adipose tissue (SAT) and total adipose tissue (TAT) areas. We assessed changes in VAT, SAT, TAT and VAT/SAT ratio after 3 years and compared the changes between patients who had undergone left-sided and right-sided colonic resection in the total population and in men and women separately.
Results
A total of 134 patients with stage I-III CC undergoing cancer surgery were included. Patients who had undergone left-sided colonic resection had after 3 years follow-up a 5% (95% CI: 2–9%, p < 0.01) increase in abdominal VAT, a 4% (95% CI: 2–6%, p < 0.001) increase in SAT and a 5% increase (95% CI: 2–7%, p < 0.01) in TAT. Patients who had undergone right-sided colonic resection had no change in VAT, but a 6% (95% CI: 4–9%, p < 0.001) increase in SAT and a 4% (95% CI: 1–7%, p < 0.01) increase in TAT after 3 years. Stratified by sex, only males undergoing left-sided colonic resection had a significant VAT increase of 6% (95% CI: 2–10%, p < 0.01) after 3 years.
Conclusion
After 3 years follow-up survivors of CC accumulated abdominal adipose tissue. Notably, those who underwent left-sided colonic resection had increased VAT and SAT, whereas those who underwent right-sided colonic resection demonstrated solely increased SAT.

Similar content being viewed by others
Introduction
Colon cancer (CC) is the fourth most common cancer worldwide [1] and it has a still increasing incidence rate [1, 2]. Survival after a CC diagnosis is steadily improving due to early detection, diagnostic precision and more advanced cancer treatment, and today more than 70% of patients with non-metastatic CC are alive after 5 years [3]. Unfortunately, the risk of developing metabolic comorbidities such as obesity, type 2 diabetes (T2D) and cardiovascular disease (CVD) after a CC diagnosis is also increasing [4, 5] with worsening of overall and cancer-specific prognosis in these patients [6].
Obesity and especially excess abdominal fat are factors increasing morbidity [7] and mortality [8] in survivors of CC. The total amount of abdominal adipose tissue (TAT) consists of the visceral adipose tissue (VAT) and the subcutaneous adipose tissue (SAT) [9]. Distribution of body fat varies between men and women [10]. Men typically have a higher amount of VAT [10]. The structure and functions of the two tissues are very different [11] with VAT being highly pro-inflammatory and a major risk factor of developing several diseases including T2D [12], CVD [13] and various cancer types [14, 15]. Excess VAT is associated with CC development [16] and a meta-analysis from 2014 showed a linear association between CT-assessed VAT area and adenomas, a CC precursor [17]. Moreover, excess VAT may increase CC relapse [18]. In contrast excess SAT hasn’t been associated with worse outcomes of CC [19].
The ratio of VAT/SAT (V/S) can be used as a prognostic marker, and a high V/S ratio has been associated with an increased risk of metabolic disturbances in a general population and with cancer recurrence in patients with CC [20, 21]. In contrast, weight loss, reducing VAT, decrease the risk of developing diseases such as T2D [22], CVD [23] in obese populations and improve the prognosis of CC [24]. We and others have shown that exercise training effectively reduces abdominal VAT in subject with overweight [25], which supports the importance of exercise training in survivors of cancer.
We recently found a post-treatment increase in VAT in survivors of colorectal cancer who were colonic resected and speculated whether the surgical treatment per se may affect metabolism including fat deposits in the body [26].
Two clinical-epidemiological studies revealed that patients treated with left-sided compared with right-sided colonic resection for CC and other colonic illnesses had an increased risk of developing T2D and CVD respectively [27, 28]. These findings raise the intriguing question whether resection of CC, and especially left-sided colonic resections, contribute to metabolic disturbances in survivors of CC.
Due to the significant impact of excess abdominal fat on CC prognosis, it may be of great clinical relevance to identify survivors of CC with a particular risk of VAT accumulation in order to initiate preventive strategies or treatment. Despite the association between excess VAT and CC prognosis no specific follow up regimes or interventions are offered to overweight survivors of CC.
The primary aim of this study was to investigate changes in abdominal VAT, SAT, TAT and V/S ratio after 3 years in patients who had undergone left-sided compared with right-sided colonic resection as part of CC treatment. Secondary aim was to examine changes over time in VAT, SAT, TAT and in V/S ratio after both CC resection types. Moreover, we aimed to examine the changes described above when stratifying subjects by sex.
Methods
Study design and population
We conducted a historical prospective study of survivors of stage I-III CC, who had undergone intended curative cancer treatment with right-sided colonic resection (right-sided hemicolectomy) or left-sided colonic resection (left-sided hemicolectomy, sigmoid resection) between 2014–2018 at Department of Surgical Gastroenterology at Copenhagen University Hospital – Herlev and Gentofte, Herlev, Denmark. Following cancer surgery some patients, depending on cancer stage, were treated with 3–6 months of adjuvant chemotherapy (FOLFOX (5-fluorouracil (5-FU), leucovorin, and oxaliplatin), CAPOX (capecitabine and oxaliplatin), monotherapy 5-FU or capecitabine) [29, 30]. As prophylaxis of acute nausea and vomiting, prednisolone was administered for a few days when a new cycle of chemotherapy was initiated [31]. In this study 50 mg/day prednisolone was administered on the day of treatment and 25 mg/day the following 2 days every second or third week, depending on the applied chemotherapy regime. However, this only applies to patients treated with FOLFOX or CAPOX, if patients were treated with monotherapy 5-FU or capecitabin no prednisolone was administered. Thus, some patients treated with adjuvant chemotherapy may have received up to 6 days of prednisolone monthly for up to 6 months.
All patients were included prior to cancer resection in the Danish REBECCA study (“Biomarkers in patients with colorectal cancer – can they provide new information on the diagnosis, treatment efficacy, adverse effects and prognosis?”), an ongoing cohort study initiated in July 2014. The cohort and study design have been described in detail previously [32]. The current study is a subgroup analysis of patients that did not meet the exclusion criteria: UICC-stage IV tumors, rectal cancer (the border between the sigmoid colon and the rectum was defined as 15 cm beyond the anal verge), active cancer at any site during the 3 year postoperative follow-up period, previous colonic resection, a history of diabetes (including current use of diabetes medication), cases where a stoma was performed peri-operatively or recurrence of cancer within the first 3 years after cancer treatment. A total of 134 patients with CC were eligible for the study and were included in the analysis (Fig. 1).

Flowchart.
All patients underwent abdominal CT-scans preoperatively for disease staging, which was repeated after 3 years according to the surveillance program to monitor cancer relapse [33]. Medical records were reviewed for all patients and information on age, sex, height, weight, ECOG performance status, lifestyle comorbidities (chronic obstructive pulmonary disease, hypertension, dyslipidemia or cardiovascular disorders), antihypertensive or steroid medication, tobacco and alcohol consumption were collected preoperatively as well as tumor location in the colon, date of the CT-scans (preoperatively and 3-years postoperatively), date of surgery, potential postoperative adjuvant treatment, peri- or postoperative complications to surgery and development of diabetes during the 3 years of surveillance. Additionally, medication lists were reviewed on a common medication server to make sure that outpatients diagnosed and treated with antidiabetic medication outside of hospitals were revealed. Clinical data were collected blinded to VAT and SAT measurements.
CT-scans
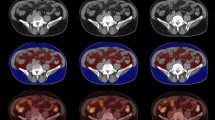
VAT and SAT areas were measured using venous phase axial CT images at the L3-level of the lumbar spine, using the exact axial image where both transversal processes were visible. We used the open-source code software Horos™ (version 3.3.6., Annapolis, MD USA) to define the adipose tissue area, indicated by tissue with Hounsfield units (HU) between −150 and −50 HU (Fig. 2), which is an attenuation value specific for fatty tissues [34]. We defined VAT as the compartment limited anteriorly and laterally by the abdominal musculature and posteriorly by the vertebral column and paraspinal musculature as previously described [35]. SAT was defined as adipose tissue located external to the abdominal and back musculature. Total adipose tissue (TAT) was calculated as the sum of the two areas. The use of CT images to determine abdominal fat depots is widely used [36] and images at L3-level of the lumbar spine has been shown to offer the highest prediction of total SAT and VAT depots in the body compared with CT images at other levels of the lumbar spine [37].

The analysis was performed at L3-level at the point where both transversal processes were visible. Adipose tissue areas were indicated by Hounsfield scale between −150 and −50 HU, which is an attenuation value specific for fatty tissues. Red color marks (A) VAT-area (B) SAT-area. Direction of scanning view: Top-down.
The VAT/SAT-ratios (V/S ratio) were calculated by dividing the mean VAT-area with the mean SAT-area.
All analyses were performed blinded to type of surgery (right- or left-sided resection) and were performed by two independent investigators, one of them being a radiographer. The intraclass correlation was determined and in case of discordance >5% between the investigators, both investigators re-evaluated their analyses. The average adipose tissue area measured by the two investigators was used in subsequent statistical analyses.
Biomarker analysis
Blood was drawn just prior to planned cancer surgery. C-reactive protein (CRP) was consecutively measured as part of the clinical blood work using high-sensitive CRP ultra-ready-to-use, liquid assay reagent by an immunoturbidimetric method on a fully automated chemistry analyzer (Kit-test SENTINEL CRP Ultra (UD), 11508 UD-2.0/02 2015/09/23) at the Department of Clinical Biochemistry. The blood samples were centrifuged at 2300 g at 4 °C for 10 min, and serum was then aliquoted and stored at −80 °C. Interleukin-6 (IL-6) was measured using a high-sensitive enzyme-linked immunosorbent assay (ELISA) (Quantikine HS600B, R&D Systems, Abingdon, UK) in accordance with the manufacturer’s instructions. IL-6 was measured using the same ELISA batch.
Statistical analyses
The primary analysis compared difference in changes in VAT, SAT, TAT and V/S ratio preoperatively to 3 years after cancer surgery. The primary analysis was based on a mixed effect model using data from all patients and performed with time, group and preoperative values as fixed effects, individual subjects as random effects and the ‘time x group’ interaction was the primary readout. For all study outcomes, the raw means and standard errors of the means (SEMs) were reported for each group for the preoperative and 3 years timepoint, along with the estimated in-group changes and between-group changes with 95% confidence intervals (CI) extracted from the mixed effects model. All variables were log-transformed to improve model compliance, accordingly the estimated in-group changes and between-group difference were analyzed on a log-scale and were reported as back-transformed relative ratios with 95% CIs. As the specified mean changes are based on estimates from the mixed effects models it might not reflect the numerical change. Thus, for example a back-transformed estimate of 0.95 corresponds to a median relative change of −5%. Differences in baseline characteristics between the right-sided and left-sided resected patients preoperatively were analyzed using unpaired t-tests. Results were considered statistically significant if p < 0.05. All the statistical analyses were performed using R-software (version 1.3.1056).
Ethics statement
This study is conducted in accordance with the Declaration of Helsinki. All experimental protocols (The REBECCA study protocol (VEK j.nr. H-2-2013-078) and additional protocol for current project (78485)) were approved by “The ethical committee of the capital region of Denmark” and the Danish Data Protection Agency in Copenhagen, Denmark (j. No. HEH-2014-044, I-suite No. 02771 and PACTIUS P-2019-614). Informed consent was obtained from all subjects included in the REBECCA study.
Results
Baseline characteristics
Preoperative baseline characteristics of the 134 patients with stage I-III CC were similar in the two resection groups (Table 1). Although not statistically significant, patients who had undergone left-sided resection (n = 80) were more likely men, had a better ECOG performance status and had more likely completed chemotherapy than patients who had undergone right-sided resection (n = 54). The cancer stage was similar in the groups except from stage 3b, which was more common in the group of left-sided resections. The higher cancer stage in this group resulted in a significantly more frequent treatment with adjuvant chemotherapy in patients who had undergone left-sided resection compared to patients who had undergone right-sided resection (left-sided: 41,3%; right-sided: 25,9%; p < 0.01).
Postoperatively only around 5% of the patients had major complication with no difference in the incidence between the two resection groups.
On average, the patients were overweight preoperatively defined by a BMI > 25 kg/m2 (left-sided resected patients: BMI 26.8, right-sided resected patients: BMI 25.6).
When stratifying the patients by sex, baseline characteristics were similar across the left-sided and right-sided resected men and women (Supplementary Tables 1 and 2), except that women in the right-sided resection group were older, had a lower cancer stage and received chemotherapy to a lesser extent than the left-sided resected women (Supplementary Table 2).
Changes in VAT, SAT, TAT and V/S after 3 years follow-up within each resection group
After 3 years follow-up, left-sided resected survivors of CC had a 5% (p < 0.01) increase in VAT, a 4% (p < 0.001) increase in SAT and a 5% (p < 0.01) increase in TAT (Table 2 and Fig. 3). After 3 years follow-up, right-sided resected survivors of CC had no change in VAT, but a 6% (p < 0.001) increase in SAT and a 4% (p < 0.01) increase in TAT. Patients who had undergone left-sided resection had no change in V/S ratio, whereas V/S ratio decreased 4% (p = 0.02) after 3 years in the patients who had undergone right-sided resection.

Changes in visceral adipose tissue (VAT), subcutaneous adipose tissue (SAT) and total adipose tissue (TAT) measured in mean cm2 preoperatively (PreOP) to 3 years after cancer surgery with left-sided colonic resection (re) (red bars) and right-sided colonic resection (re) (blue bars). Data represent mean ± SEM. *p < 0.05 determined by a within group analysis from a linear mixed effect model.
Differences in VAT, SAT, TAT and V/S between the resection groups
Preoperatively no difference was found between patients who had undergone left-sided and right-sided resection (Table 2). After 3-years follow-up, we found no difference in the mean changes in SAT, TAT and V/S ratio between left-sided and right-sided resection group. Moreover, when evaluating VAT in the main analysis, the group x time interaction was insignificant (p = 0.24).
Within group changes in VAT, SAT, TAT and V/S in men and women separately
Within group changes in VAT, SAT, TAT and V/S for men and women separately are presented in supplementary Table 1. After 3-years follow up, left-sided resected men had an increased in VAT (6%, p < 0.01), SAT (4%, p < 0.01) and TAT (5%, p < 0.01), whereas women had an increased SAT (5%, p < 0.01) and TAT (5%, p < 0.01), but not VAT.
For both men and women, who had undergone right-sided cancer resection, no changes in VAT were observed after 3 years. In men a 6% (p < 0.01) increase in SAT and no change in TAT was observed after 3 years. In right-sided resected women a 7% (p < 0.001) increase in SAT and a 5% (p = 0.01) increase in TAT was observed after 3 years.
In men, the V/S ratio in the left-sided resected group was unchanged after 3 years follow-up, while it was decreased 4% (p = 0.02) in right-sided resected. In women, the V/S-ratio did not change over time in any of the groups.
Differences in VAT, SAT, TAT and V/S between resection groups in men and women separately
Stratifying by gender did not change the results; preoperative measurement as well as the mean changes after 3 years follow-up in SAT, TAT and V/S ratio were similar in patients who had undergone left-sided and right-sided resection. Between group differences in men and women separately are presented in supplementary Table 1. When comparing changes in SAT, TAT and V/S ratio within the two resection groups preoperatively to 3 years after surgery we found no significant difference between the two resection groups in either men or women. When comparing VAT, SAT, and TAT in patients who had undergone right-sided vs. left-sided resection preoperatively no difference was found in either men or women.
Diabetes development
After reviewing medical records, none of the patients were diagnosed with T2D or were prescribed anti-diabetic medication during 3 years of surveillance. Thus, it was not possible to assess changes in diabetes development across the groups.
Discussion
Our main finding was that patients operated for stage I-III CC increase in abdominal adiposity over the course of 3 years following cancer surgery, but there may be a tendency towards higher VAT accumulation in patients undergoing left-sided colonic resection. This trend was similar for both men and women, but only statistically significant for male survivors of CC.
Due to the potential prognostic significance of increased VAT in left-sided resected survivors of CC may constitute a population at risk of developing metabolic disturbances and having an inferior cancer prognosis.
The overall increase in VAT after surgical cancer treatment is in line with our prior findings [26]. In that study it was speculated whether the type of cancer resection per se has the potential to alter lipid metabolism.
Our data indicate that left-sided colonic resected survivors of CC may constitute a risk population. This is in line with two recent epidemiological studies. In 2018 Jensen and coworkers showed that left-sided colonic resections compared with right-sided colonic resections was associated with an increased risk of T2D in patients with CC and non-cancer patients suffering from inflammatory bowel disease etc. [27]. Later, a study from Taiwan explored the association between resection type and metabolic disturbances in patients without CC and found a higher CVD risk after left-sided resection, and a reduction in T2D after right-sided resection when compared with non-colectomy subjects [38]. However, the most recent epidemiological study found an increased risk of T2D after colectomy compared with small bowel resection, but when stratifying by resection type, no difference in T2D risk was found [39].
According to a prior study establishing a cut-off value of pathological obesity in patients with cancer, a VAT of 163.8 cm2 in males (83.6% sensitivity, 62.5% specificity) and 80.1 cm2 in females (96% sensitivity, 73.2% specificity) was strongly correlated with presence of the metabolic syndrome, a precursor of T2D, in Caucasians [40]. Accordingly, based on these cut-off values both males and females independent of resection type had pathological abdominal obesity preoperatively in the present study, which worsened during the follow up period. Based on VAT data it is likely that some of the patients may have developed metabolic syndrome 3 years after cancer surgery, but we didn’t have the relevant variables to detect it post-surgery.
It is well known that excess VAT is accompanied by low-grade inflammatory changes within the fat depot. This contributes to chronic systemic inflammation with enhanced concentrations of circulating cytokines such as CRP and IL-6 and adipokines [41], which is associated with cancer progression and poor survival in patients with CC [42]. In the present study CRP and IL-6 levels were only available preoperatively and values were within the normal range in both resection groups and in men and women respectively.
Our data revealed that SAT was increased independent of resection type and in both sexes after 3 years. In contrast to VAT, the role of abdominal SAT in development of diabetes, CVD and cancer recurrence and death after cancer resection is not fully understood [43, 44]. Nonetheless, an increase in VAT is highly correlated with an increase in SAT [43, 44].
Until recently the impact of adiposity on CC prognosis has been confusing [45]. The divergent results may be due to the various ways to measure adiposity in former studies (eg BMI, waist-circumference, bioelectrical impedance, quantitative CT-scans etc.) [46]. However, since excess adipose tissue is believed to be involved in the underlying pathogenesis of CC [47], it seems plausible that adiposity is associated with more aggressive cancers with increased rates of recurrence. This was confirmed in a recent and the largest metanalysis including 45 studies and 607,266 patients with stage I to IV colorectal cancer as they reported a significant increase in cancer specific (OR = 1.27; 95% CI 1.11–1.45) and overall (OR = 1.20; 95% CI 1.06–1.36) mortality in obese patients compared with patients who were normal-weight [45]. Moreover, increased waist circumference, which is strongly correlated to VAT [48], was associated with increased cancer specific mortality [45].
The distribution of abdominal fat expressed as the V/S ratio has been used as prognostic marker in prior studies. In a study by Hyeong-Gon Moon et al. including 161 patients who had undergone colonic resection for CRC (both men and women) revealed that a preoperative V/S ratio > 0.83 (average V/S-ratio preoperatively was 0.83 in our study) was associated with significantly lower cumulative disease-free survival rate during 8 years of post-operative follow-up [21]. Based on this study survivors of CC who had undergone left-sided colonic resection in the present study may have a worse prognosis. However, this is in contrast to a prospective observational study showing that overall survival was reduced in right-sided compared with left-sided resected patients with CRC [49], and similar studies suggest that tumor location have no impact on overall survival [50].
Due to the strong association between excess VAT and morbidity and mortality in survivors of CC, identifying survivors of CC with increased amounts of VAT may be of great clinical relevance. Our study revealed a tendency towards increased VAT after left-sided CC resection. This is in line with two prior epidemiological studies showing that patients who had undergone left-sided colonic resection may constitute a risk population.
A strength of the present work is that the method used as quantitative computed tomography (CT) to determine VAT, SAT and TAT in CC is well established. CT scans were consistently performed before surgery in relation to cancer staging and later until 3 years postoperatively to detect disease recurrence. Furthermore, all analyses were performed blinded to type of surgery (right or left-sided resection) and were performed by two independent investigators. Another strength of this study is the prospective nature of the study allowing us to detect changes in abdominal fat depots over time.
Our study also has several limitations listed below. First of all, we lack all other variables except for CT-scan results after 3 years. In addition, due to the exploratory nature of the study there is a risk of type 2 statistical errors for some parameters including the lack of difference in the between group comparisons for VAT in opposition to the clear increase in VAT in the left-sided resected but not the right sided resected in the with-in group analysis.
Another limitation is the difference in administration of adjuvant chemotherapy between resection groups. When comparing baseline characteristics, the left-sided tumors were detected at a slightly more advanced cancer stage, and therefore adjuvant chemotherapy was administered more frequent after left-sided resections. However, to the best of our knowledge there is no evidence suggesting that 3–6 months of adjuvant chemotherapy treatment with FOLFOX, CAPOX or monotherapy 5-FU or capecitabine postoperatively affects changes in abdominal adipose tissue after 3 years.
To avoid adverse effects during each cycle of adjuvant chemotherapy some patients receive a few days days of prednisolone treatment [31]. Thus, in this study patients who had undergone left-sided resection may have received larger amounts of prednisolone well known to induce hyperglycemia [51] and central obesity [52]. Unfortunately, we do not have information regarding the amount of prednisolone each patient received during treatment with adjuvant chemotherapy. However, as prednisolone treatment will typically only be administered for a few days each month when a new cycle of chemotherapy is initiated, we do not expect the applied doses of prednisolone to have affected metabolism over a time course of 3 years in this study [53]. Finally, weight loss prior to cancer surgery was not recorded systematically.
.
Conclusion
After 3 years follow-up survivors of CC accumulated abdominal adipose tissue. Notably, those who underwent left-sided colonic resection had increased VAT and SAT, whereas patients who had undergone right-sided colonic resection demonstrated solely increased SAT.
Data availability
The data that support the findings of this study are available from [louise.lang.lehrskov.01@regionh.dk] but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of [louise.lang.lehrskov.01@regionh.dk].
References
Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019;14:89–103.
Rahib L, Wehner MR, Matrisian LM, Nead KT. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw Open. 2021;4:e214708.
(NORDCAN) AoTNCR. 5-year age-standardised relative survival (%), Males and Females, colorectal, Denmark. Available from: https://nordcan.iarc.fr/en/dataviz/survival?cancers=520&set_scale=0&sexes=1_2&populations=208 (2021).
Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, Barzi A, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177–93.
Singh S, Earle CC, Bae SJ, Fischer HD, Yun L, Austin PC, et al. Incidence of diabetes in colorectal cancer survivors. J Natl Cancer Inst. 2016;108:djv402.
Mills KT, Bellows CF, Hoffman AE, Kelly TN, Gagliardi G. Diabetes mellitus and colorectal cancer prognosis: a meta-analysis. Dis Colon Rectum. 2013;56:1304–19.
Park JW, Chang SY, Lim JS, Park SJ, Park JJ, Cheon JH, et al. Impact of visceral fat on survival and metastasis of stage III colorectal Cancer. Gut Liver. 2022;16:53–61.
Brown JC, Caan BJ, Prado CM, Cespedes Feliciano EM, Xiao J, Kroenke CH, et al. The association of abdominal adiposity with mortality in patients with stage I-III colorectal cancer. J Natl Cancer Inst. 2020;112:377–83.
Mittal B. Subcutaneous adipose tissue & visceral adipose tissue. Indian J Med Res. 2019;149:571–3.
Karastergiou K, Smith SR, Greenberg AS, Fried SK. Sex differences in human adipose tissues - the biology of pear shape. Biol Sex Differ. 2012;3:13.
Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11:11–8.
Hanley AJ, Wagenknecht LE, Norris JM, Bryer-Ash M, Chen YI, Anderson AM, et al. Insulin resistance, beta cell dysfunction and visceral adiposity as predictors of incident diabetes: the Insulin Resistance Atherosclerosis Study (IRAS) Family study. Diabetologia. 2009;52:2079–86.
Powell-Wiley TM, Poirier P, Burke LE, Després JP, Gordon-Larsen P, Lavie CJ, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143:e984–e1010.
Steffen A, Schulze MB, Pischon T, Dietrich T, Molina E, Chirlaque MD, et al. Anthropometry and esophageal cancer risk in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. 2009;18:2079–89.
Kim MS, Choi YJ, Lee YH. Visceral fat measured by computed tomography and the risk of breast cancer. Transl Cancer Res. 2019;8:1939–49.
Lee JY, Lee HS, Lee DC, Chu SH, Jeon JY, Kim NK, et al. Visceral fat accumulation is associated with colorectal cancer in postmenopausal women. PLoS One. 2014;9:e110587.
Keum N, Lee DH, Kim R, Greenwood DC, Giovannucci EL. Visceral adiposity and colorectal adenomas: dose-response meta-analysis of observational studies. Ann Oncol. 2015;26:1101–9.
Sørensen TI, Virtue S, Vidal-Puig A. Obesity as a clinical and public health problem: is there a need for a new definition based on lipotoxicity effects? Biochim Biophys Acta. 2010;1801:400–4.
Jung IS, Shin CM, Park SJ, Park YS, Yoon H, Jo HJ, et al. Association of visceral adiposity and insulin resistance with colorectal adenoma and colorectal cancer. Intest Res. 2019;17:404–12.
Hiuge-Shimizu A, Kishida K, Funahashi T, Ishizaka Y, Oka R, Okada M, et al. Absolute value of visceral fat area measured on computed tomography scans and obesity-related cardiovascular risk factors in large-scale Japanese general population (the VACATION-J study). Ann Med. 2012;44:82–92.
Moon H-G, Ju Y-T, Jeong C-Y, Jung E-J, Lee Y-J, Hong S-C, et al. Visceral obesity may affect oncologic outcome in patients with colorectal cancer. Ann Surg Oncol. 2008;15:1918–22.
Campos R, Masquio DCL, Corgosinho FC, Caranti DA, Ganen AP, Tock L, et al. Effects of magnitude of visceral adipose tissue reduction: Impact on insulin resistance, hyperleptinemia and cardiometabolic risk in adolescents with obesity after long-term weight-loss therapy. Diab Vasc Dis Res. 2019;16:196–206.
Brown JD, Buscemi J, Milsom V, Malcolm R, O’Neil PM. Effects on cardiovascular risk factors of weight losses limited to 5-10. Transl Behav Med. 2016;6:339–46.
Xiao J, Mazurak VC, Olobatuyi TA, Caan BJ, Prado CM. Visceral adiposity and cancer survival: a review of imaging studies. Eur J Cancer Care (Engl). 2018;27:e12611.
Wedell-Neergaard AS, Lang Lehrskov L, Christensen RH, Legaard GE, Dorph E, Larsen MK, et al. Exercise-induced changes in visceral adipose tissue mass are regulated by IL-6 signaling: a randomized controlled trial. Cell Metab. 2019;29:844–55.e3.
Christensen JF, Sundberg A, Osterkamp J, Thorsen-Streit S, Nielsen AB, Olsen CK, et al. Interval walking improves glycemic control and body composition after cancer treatment: a randomized controlled trial. J Clin Endocrinol Metab. 2019;104:3701–12.
Jensen AB, Sørensen TI, Pedersen O, Jess T, Brunak S, Allin KH. Increase in clinically recorded type 2 diabetes after colectomy. Elife. 2018;7:e37420.
Wu CC, Lee CH, Hsu TW, Yeh CC, Lin MC, Chang CM, et al. Is colectomy associated with the risk of type 2 diabetes in patients without colorectal cancer? A population-based cohort study. J Clin Med. 2021;10:5313.
Grothey A, Sobrero AF, Shields AF, Yoshino T, Paul J, Taieb J, et al. Duration of adjuvant chemotherapy for stage III colon cancer. N Engl J Med. 2018;378:1177–88.
DCCG. Adjuverende kemoterapi ved koloncancer stadium III. 2021.Available from: https://www.dmcg.dk/siteassets/forside/kliniske-retningslinjer/godkendte-kr/kolorektal/dccg_adjkemocolon-stadiumiii_v2.1_admgodk030122.pdf.
Roila F, Molassiotis A, Herrstedt J, Aapro M, Gralla RJ, Bruera E, et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann Oncol. 2016;27:v119–v33.
Dolin TG, Christensen IJ, Johansen AZ, Nielsen HJ, Jakobsen HL, Klein MF, et al. Pre- and perioperative inflammatory biomarkers in older patients resected for localized colorectal cancer: associations with complications and prognosis. Cancers. 2021;14:161.
Authority DHaM. Opfølgningsprogram for tyk- og endetarmskræft. 2015.
Kim S, Lee GH, Lee S, Park SH, Pyo HB, Cho JS. Body fat measurement in computed tomography image. Biomed Sci Instrum. 1999;35:303–8.
Choe EK, Park KJ, Ryoo SB, Moon SH, Oh HK, Han EC. Prognostic impact of changes in adipose tissue areas after colectomy in colorectal cancer patients. J Korean Med Sci. 2016;31:1571–8.
Pop R, Raluca P. Using abdominal CT data for visceral fat evaluation. Acta Medica Marisiensis. 2013;59:254–6.
Cheng X, Zhang Y, Wang C, Deng W, Wang L, Duanmu Y, et al. The optimal anatomic site for a single slice to estimate the total volume of visceral adipose tissue by using the quantitative computed tomography (QCT) in Chinese population. Eur J Clin Nutr. 2018;72:1567–75.
Wu CC, Hsu TW, Yeh CC, Lee CH, Lin MC, Chang CM. The impact of colectomy on the risk of cardiovascular disease among patients without colorectal cancer. Sci Rep. 2020;10:2925.
Allin KH, Agrawal M, Iversen AT, Antonsen J, Villumsen M, Jess T. The risk of type 2 diabetes in patients with inflammatory bowel disease after bowel resections: a nationwide cohort study. Gastro Hep Adv. 2022;1:777–84.
Doyle SL, Bennett AM, Donohoe CL, Mongan AM, Howard JM, Lithander FE, et al. Establishing computed tomography-defined visceral fat area thresholds for use in obesity-related cancer research. Nutr Res. 2013;33:171–9.
Furuhashi M, Hotamisligil GS. Fatty acid-binding proteins: role in metabolic diseases and potential as drug targets. Nat Rev Drug Discov. 2008;7:489–503.
Rasic I, Rebic V, Rasic A, Aksamija G, Radovic S. The association of simultaneous increase in interleukin-6, C reactive protein, and matrix metalloproteinase-9 serum levels with increasing stages of colorectal cancer. J Oncol. 2018;2018:2830503.
Liu J, Fox CS, Hickson DA, May WD, Hairston KG, Carr JJ, et al. Impact of abdominal visceral and subcutaneous adipose tissue on cardiometabolic risk factors: the Jackson Heart Study. J Clin Endocrinol Metab. 2010;95:5419–26.
Fox CS, Massaro JM, Hoffmann U, Pou KM, Maurovich-Horvat P, Liu CY, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation. 2007;116:39–48.
Jaspan V, Lin K, Popov V. The impact of anthropometric parameters on colorectal cancer prognosis: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2021;159:103232.
Fang H, Berg E, Cheng X, Shen W. How to best assess abdominal obesity. Curr Opin Clin Nutr Metab Care. 2018;21:360–5.
Ma Y, Yang Y, Wang F, Zhang P, Shi C, Zou Y, et al. Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLOS One. 2013;8:e53916.
Gadekar T, Dudeja P, Basu I, Vashisht S, Mukherji S. Correlation of visceral body fat with waist–hip ratio, waist circumference and body mass index in healthy adults: a cross sectional study. Med J Armed Forces India. 2020;76:41–6.
Kalantzis I, Nonni A, Pavlakis K, Delicha EM, Miltiadou K, Kosmas C, et al. Clinicopathological differences and correlations between right and left colon cancer. World J Clin Cases. 2020;8:1424–43.
Livingston AJ, Bailey CE. Invited editorial: does side really matter? Survival analysis among patients with right- versus left-sided colon cancer: a propensity score-adjusted analysis. Ann Surg Oncol. 2022;29:9–10.
Jeong Y, Han HS, Lee HD, Yang J, Jeong J, Choi MK, et al. A Pilot study evaluating steroid-induced diabetes after antiemetic dexamethasone therapy in chemotherapy-treated cancer patients. Cancer Res Treat. 2016;48:1429–37.
Lee MJ, Pramyothin P, Karastergiou K, Fried SK. Deconstructing the roles of glucocorticoids in adipose tissue biology and the development of central obesity. Biochim Biophys Acta. 2014;1842:473–81.
Azam F, Latif MF, Farooq A, Tirmazy SH, AlShahrani S, Bashir S, et al. Performance status assessment by using ECOG (Eastern Cooperative Oncology Group) score for cancer patients by oncology healthcare professionals. Case Rep Oncol. 2019;12:728–36.
Acknowledgements
This work was supported by the Danish Diabetes Association and the Danish Diabetes Academy, which is funded by the Novo Nordisk Foundation under grant number NNF17SA0031406. The Centre for Physical Activity Research (CFAS) is supported by TrygFonden (grants ID 101390, ID 20045, and ID 125132). The VELUX foundation (Grant project number 00018310, salary to TGD) is acknowledged. Chief physician Benny Vittrup is acknowledged for his important contribution to the REBECCA study.
Funding
Open access funding provided by National Hospital.
Author information
Authors and Affiliations
Contributions
Conceptualization LLL. Methodology LLL, TIAS, JFC, MSS, YKM and TGD. Access to and verified the raw data and formal analysis LLL, MSS, YKM. Resources LLL and MSS. Writing – original draft LLL and YKM. Writing – review and editing, all authors contributed. All authors approved the final version for publication, and LLL had final responsibility for the decision to submit.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kays Mohammed Ali, Y., Dolin, T.G., Damm Nybing, J. et al. Change in abdominal obesity after colon cancer surgery – effects of left-sided and right-sided colonic resection. Int J Obes 48, 533–541 (2024). https://doi.org/10.1038/s41366-023-01445-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-023-01445-8
