
Abstract
Objective
Coronavirus disease 2019 (COVID-19) has disproportionally affected communities of color. We aimed to determine what factors are associated with COVID-19 testing and test positivity in an underrepresented, understudied, and underreported (U3) population of mothers.
Methods
This study included 2996 middle-aged mothers of the Boston Birth Cohort (a sample of predominantly urban, low-income, Black and Hispanic mothers) who were enrolled shortly after they gave birth and followed onward at the Boston Medical Center. COVID-19 testing and test positivity were defined by the SARS-CoV-2 nucleic acid test. Two-probit Heckman selection models were performed to identify factors associated with test positivity while accounting for potential selection associated with COVID testing.
Results
The mean (SD) age of study mothers was 41.9 (±7.7) years. In the sample, 1741 (58.1%) and 667 (22.3%) mothers were self-identified as Black and Hispanic, respectively. A total of 396 mothers had COVID-19 testing and of those, 95 mothers tested positive from March 2020 to February 2021. Among a multitude of factors examined, factors associated with the probability of being tested were obesity (RR = 1.27; 95% confidence interval (CI): 1.08–1.49); and presence of preexisting chronic medical conditions including hypertension, asthma, stroke, and other comorbidities (coronary heart disease, chronic kidney disease, and sickle cell disease) with a corresponding RR = 1.40 (95% CI: 1.23–1.60); 1.29 (95% CI: 1.11–1.50); 1.44 (95% CI: 1.23–1.68); and 1.37 (95% CI: 1.12–1.67), respectively. Factors associated with higher incident risk of a positive COVID-19 test were body mass index, birthplace outside of the USA, and being without a college-level education.
Conclusions
This study demonstrated the intersectionality of obesity and social factors in modulating incident risk of COVID-19 in this sample of US Black and Hispanic middle-aged mothers. Methodologically, our findings underscore the importance of accounting for potential selection bias in COVID-19 testing in order to obtain unbiased estimates of COVID-19 infection.
Similar content being viewed by others
Introduction
Coronavirus disease 2019 (COVID-19), a novel infectious disease with devastating health implications, was declared a global pandemic by the World Health Organization in March 2020. As of July 19, 2021, there have been 33,896,296 total reported cases of COVID-19 and 606,618 associated deaths in the United States (US) [1]. Of particular concern, COVID-19 has disproportionally affected communities of color [2,3,4,5]. Specifically, the number of COVID-19 cases among Black, Hispanic, and Latinx persons is nearly three times that of White non-Hispanic persons, while hospitalizations are nearly five times that of Whites [6]. These disparities extend beyond hospitalizations, as rates of COVID-19-related deaths among Black populations are triple or more than that of Whites [6]. However, to better understand the root cause of these disparities, the urgent but unsettled question for individual- and population-based risk assessment and prevention of COVID-19 is: what factors are associated with increased risk of COVID-19 in these high-risk minority populations?
Many studies have reported associations between obesity and other preexisting chronic medical conditions and COVID-19 infection and severity [3, 5, 7, 8], in addition to lower socioeconomic status, overcrowded living environments, poverty, and employment in essential frontline jobs where social distancing is challenging. (https://read.oecd-ilibrary.org/view/?ref=137_137245-8saheqv0k3&title=What-is-the-impact-of-the-COVID-19-pandemic-on-immigrants-and-their-children%3F) [4, 5]. Importantly, the obesity epidemic and its associated morbidities such as diabetes and hypertension have persisted in the US and disproportionally affected low-income minority populations [9, 10]. Although some studies have examined race and ethnicity disparities in testing, incidence, and outcomes of COVID-19 [3, 4, 11], data are limited about what factors are associated with excess COVID-19 infection rate in communities of color, especially, among those understudied and underrepresented, including urban, low-income, minority, mothers. Further limiting our understanding of associated factors, most studies have performed analyses on individuals who received COVID-19 testing [4, 5, 7, 8, 12] or in general cohort population [13, 14], but did not take into account selection in COVID-19 testing. Given COVID-19 testing was not performed at random due to limited testing availability and prioritization, particularly in the early phases of the pandemic, such analyses may have led to selection bias [3]. To obtain unbiased estimates, appropriate data analysis approach that takes into account sample selection is needed.
In this study, we sought to address the aforementioned research gaps in a sample of primarily Black and Hispanic, low-income, middle-aged mothers living in Boston, MA, one of the many cities hit hard by the COVID-19 pandemic. It is important to study this sample from a range of research, clinical, public health, and equity perspectives. This is a high-risk yet understudied population due to their socio-demographic disadvantage. Yet, in many ways, these mothers are the backbone of their families and society: they are the primary caregivers for children and older family members, bread winners, and more likely to be frontline workers. Their health and well-being largely affect both their families and society. A unique feature of this study is our ability to integrate baseline socio-demographic and clinical variables with longitudinal follow-up to delineate risk factors of COVID-19 incident risk in a well-defined population. We aimed to identify factors associated with COVID-19 testing and test positivity, including age, race/ethnicity, education, nativity, obesity, and preexisting medical conditions, which may affect an individual’s probability of exposure to COVID-19 and/or personal knowledge and use of protective measures (such as face mask, gloves, alcohol-based hand sanitizer, etc.) as well as susceptibility to COVID-19 infection. Analytically, this study applied two-probit Heckman selection models to identify factors associated with test positivity.
Methods
Study participants
Study participants were mothers enrolled in the Boston Birth Cohort (BBC) [15], a predominantly urban, low-income, minority population in Boston, Massachusetts, one of the large cities seriously affected by COVID-19. As of July 19, 2021, there have been 71,399 cases of COVID-19 and 1395 associated deaths in Boston [16]. Detailed information on participant enrollment has been described previously [15]. Briefly, mother–infant pairs were enrolled 24 to 72 h after delivery. After obtaining written informed consent, trained research staff interviewed mothers using a standardized questionnaire to obtain socio-demographic, lifestyle, diet, and environmental and health variables [17]. This study only focused on mothers. Maternal date of birth was abstracted from medical records. This study included those mothers who continued their medical care at the Boston Medical Center (BMC) and consented to participate in the postnatal follow-up study. A detailed description of the postnatal follow-up was described previously [18]. In brief, to minimize study participants’ burden, we tried to align research study visits with study participant’s clinical appointments. Maternal postnatal clinical data, including weight, height, and chronic clinical diseases were extracted from mothers’ medical records. As shown in the study flowchart (Supplementary Fig. 1), as of October 2020, data were collected from 3394 BBC mother–child pairs who have continued to receive primary care at BMC. Of those, 398 mothers were removed because their written informed consent was expired (n = 98) or because of being enrolled twice due to repeated pregnancies (n = 300). The final sample for this study included 2996 mothers who were enrolled for postnatal follow-up during 2004–2019. Compared to the entire BBC sample, mothers included in the current study were similar to the overall cohort, except that they were more likely to be Black (Supplementary Table 1). The study protocol was approved by the Institutional Review Boards of BMC and Johns Hopkins Bloomberg School of Public Health. Written informed consent was obtained from all study participants.
Socio-demographic variables
At study enrollment, each mother completed a questionnaire to assess race/ethnicity, education, nativity, and smoking during pregnancy, along with their medical and reproductive history. For this study, race/ethnicity was grouped into Black (i.e., Black and not Hispanic), Hispanic, and Other. Educational attainment was grouped into “high school and below” or “college and above.” Nativity was categorized into “US-born” or “foreign-born.”
Adiposity measurements
Weight and height at index prepregnancy were obtained by in-person questionnaire. Weight and height during follow-up measured by medical staff at clinic visits were extracted from the mothers’ electronic medical records (EMRs). Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Overweight and obesity were defined as BMI ≥ 25 kg/m2 but <30 kg/m2 and BMI ≥ 30 kg/m2, respectively [19]. In this report, we used BMI at the last clinical visit before the COVID-19 pandemic. The median (inter-quartile range) timeframe of the last maternal visit before the defined onset of the pandemic was 2.7 (1.6–6.5) years.
Ascertainment of chronic medical conditions during follow-up
Preexisting chronic medical conditions (diabetes mellitus, hypertension, coronary heart disease (CHD), chronic kidney disease (CKD), stroke, asthma, and sickle cell disease (SCD)) were abstracted from the mothers’ EMRs and identified by the International Classification of Diseases (ICD) ninth revision, Clinical Modification (ICD-9-CM) and tenth revision (ICD-10-CM) codes. Diabetes was diagnosed based on ICD-9-CM: 250 and ICD-10-CM: E10-E11 [20]. Chronic hypertension was diagnosed based on ICD-9-CM: 401–404; ICD-10-CM: I10-I15 [20, 21]. CHD was defined as ICD-9-CM: 410–414 and 429.2; or ICD-10-CM: I20-I25 [20]. Stroke was defined as ICD-9-CM: 430 to 438; and ICD-10-CM: 160 to 169 [20]. CKD was defined based on ICD codes: ICD-9-CM 585.0–585.6, 585.9; and ICD-10-CM: N18.1-N18.5, N18.9. Asthma was defined as ICD-9-CM of 493 and ICD-10-CM of J45 [22]. SCD was defined as ICD-9-CM of 282.60–282.64, 282.68–282.69, 282.41–282.42 and ICD-10-CM of D57.0, D57.1, D57.2, D57.4, and D57.8. Due to a small number of CHD, CKD, and SCD, we combined these three conditions as “Other comorbidity”. Finally, a composite comorbidity score was calculated by counting the number of chronic medical conditions (range from 0–6) and further categorized into 0, 1, and 2+.
COVID-19 testing status and test result
COVID-19 test receipt and result were identified through continuous EMR (including emergency room, inpatient, outpatient, and laboratory data) surveillance of the study mothers at BMC (the medical home for the study mothers) from March 2020 through February 2021. Laboratory result of the nucleic acid test for SARS-CoV-2 (the virus that causes COVID-19) was categorized as “tested” vs. “non-tested;” those tested were further grouped into “tested positive” vs. “tested negative.” For the study period, the majority of COVID-19 tests were conducted at BMC, which served as one of the major COVID-19 testing sites in Boston, MA. In rare cases when testing occurred outside of BMC, EMR surveillance documented COVID testing both at BMC and outside facilities.
Statistical analyses
Demographic and clinical variables are presented as mean (SD) for continuous variables and frequencies (proportions) for categorical variables across COVID-19 testing and test positivity status. Unadjusted P values for group comparisons (i.e., tested vs non-tested or test negative vs test positive) were calculated using the Chi-square test for categorical variables and by t test for continuous variables. Pearson correlation was performed to examine the correlation between BMI at baseline (index prepregnancy) and follow-up. Since BMI at baseline and follow-up were highly correlated (ρ = 0.67, Supplementary Fig. 2), only BMI or obesity status at follow-up were included in subsequent analyses.
First, probit regression was applied to capture the characteristics of COVID-19 testing in univariate and fully adjusted models, respectively. The fully adjusted models included age groups, race/ethnicity, nativity, education, obesity status, diabetes, hypertension, asthma, stroke, and other comorbidities. Risk ratios (RRs) and corresponding 95% confidence intervals (CIs) were reported. Next, we further examined risk factors for COVID-19 test positivity. Since COVID-19 testing was not performed at random due to limited test availability and prioritization, particularly in the early phases of the pandemic, two-probit Heckman (two-step) selection models were applied to obtain unbiased estimates using sampleSelection R package [23]. In step 1, we specified a probit regression for the probability of COVID-19 testing. In step 2, we specified a probit regression for COVID-19 test positivity, conditioned on the probability of testing.
The proportion of COVID-19 test positivity in subgroup was calculated among mothers with testing results. To address the effect of smoking, we performed a sensitivity analysis including maternal smoking status at baseline (during index pregnancy) in the model, because data on smoking at follow-up were not available. In addition, given that this study included data collected from March 2020 to February 2021, a wide timeframe, during which potentially different exposure risks over time across subgroup populations were present, we conducted a sensitivity analysis with additional adjustment for indicators of COVID-19 pandemic time periods specific to Boston, MA (lockdown on March 24; phase 1 reopening on May 18, 2020; phase 2 reopening on June 8, 2020; phase 3 reopening on July 13, 2020; and return to phase 2 on December 16, 2020). All statistical analyses were performed using RStudio (version 3.6.2, R-Tools Technology Inc., ON, CANADA). A two-sided P value <0.05 was considered to be statistically significant.
Results
Characteristics of the study population
The review of EMR data revealed that 13.2% of the study sample (n = 396) received a COVID-19 test from March 1, 2020 to Feb 14, 2021. Nearly 24% of those tested (n = 95) were positive for COVID-19. Table 1 presents the study population’s demographic characteristics at enrollment and clinical variables at the last visit during follow-up. More than half of the sample (n = 1741) were self-identified as Black (58.1%) and 667 (22.3%) as Hispanic. About 51.9% of the mothers had at least one diagnosed chronic medical condition (hypertension, diabetes, asthma, stroke, CHD, CKD, SCD). Compared to non-tested mothers, tested mothers had higher BMI and included a higher proportion with obesity as well as higher rates of hypertension, stroke, asthma, and other chronic medical conditions at follow-up. Participants with a positive COVID-19 test were more likely to be foreign-born compared with participants with a negative COVID-19 test (82.1% vs 44.5%).
Factors associated with COVID-19 testing
Being older than age 45 years was associated with a 21% lower risk ratio (RR = 0.79, 95% CI: 0.66–0.94) for COVID-19 testing, after adjustment for covariates, compared to mothers younger than age 35 years (Table 2). In addition, compared to mothers with normal weight, there was a dose–response association between being overweight (1.18 times (95% CI: 1.00–1.40)) or having obesity (1.27 times (95% CI: 1.08–1.49)) and being tested. Of note, the association between being overweight and being tested was marginal, p = 0.058; but the association between having obesity and being tested was significant, p = 0.004. Chronic medical conditions including diabetes, hypertension, stroke, asthma, and other comorbidities (CHD, CKD, SCD) were each associated with an increased probability of seeking COVID-19 testing, RR (95% CI): 1.28 (1.09–1.51), 1.47 (1.31–1.66), 1.46 (1.27–1.68), 1.54 (1.32–1.79), and 1.56 (1.29–1.89), respectively, compared to mothers without these conditions. These associations remained statistically significant in the fully adjusted model, except for diabetes (Table 2).
Factors associated with COVID-19 test positivity
By applying two-step Heckman selection models to correct for selection for COVID-19 testing, we found that higher educational attainment (college and above) was associated with a 10 percentage point reduction in the probability of COVID-19 test positivity (coefficient = −0.10, se = 0.04, p = 0.024) (Table 3), compared to lower educational attainment (high school and below). In contrast, being foreign-born was associated with a 25 percentage point increase in the probability of COVID-19 test positivity (coefficient = 0.25, se = 0.05, p = 0.000), compared to being US-born. Furthermore, a 3 percentage point increase in the risk of COVID-19 test positivity per 5 kg/m2 increase in BMI at the last study visit was observed (coefficient = 0.03, se = 0.01, p = 0.018). Although having two or higher of comorbidity score had a trend towards higher risk of COVID-19 test positivity (coefficient = 0.18, se = 0.12, p = 0.144), it did not reach significance (Table 3).
COVID-19 test positivity stratified by obesity status, nativity, education, and race/ethnicity
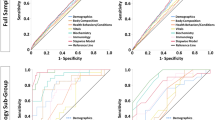
As shown in Fig. 1, mothers with lower educational attainment and obesity (Panel 1A) and mothers with foreign-born status and obesity (Panel 1B) had higher proportion of test positivity for COVID-19. When further stratified by race/ethnicity, foreign-born Black mothers with obesity had the highest proportion (Panel 1C) and foreign-born none-Black or foreign-born Black mothers with lower educational attainment had higher proportion of test positivity for COVID-19 than US-born none-Black mothers with higher education level (Panel 1D).

Plot A displays the proportion of COVID-19 test positivity stratified by education and obesity; plot B displays the proportion of COVID-19 test positivity stratified by nativity and obesity; plot C displays the proportion of COVID-19 test positivity stratified by race/ethnicity, nativity, and obesity; and plot D displays the proportion of COVID-19 test positivity stratified by race/ethnicity, nativity, and education level.
Sensitivity analysis
Since we collected data on maternal smoking status at baseline (i.e., during index pregnancy), but not in follow-up, we included maternal smoking status during pregnancy in the Heckman selection model. We observed a 17 percentage point reduction in COVID-19 test positivity in smoker, but smoking was not associated with COVID-19 testing (Supplementary Table 2). Moreover, the number of COVID-19 testing and test positivity in our study population were parallel with the time period of COVID-19 pandemic in Boston, MA (Supplementary Fig. 3). To adjust for potentially different exposure risks over time, the indicators of COVID-19 pandemic time periods specific to Boston were included in the Heckman model, though similar results were obtained (Supplementary Table 3).
Discussion
This study is unique in respect to the specific efforts taken to account for selection bias in testing and to apply a closer lens to the intersectionality of obesity, chronic diseases, and social factors to examine COVID-19 testing and test positivity among middle-aged Black and Hispanic mothers. This study fills a research gap in the literature related to advancing our understanding of factors affecting incident risk for COVID-19 in understudied, underrepresented, and underreported (U3) populations. Specifically, in this cohort of primarily Black and Hispanic middle-aged, low-income mothers, we identified factors associated with COVID-19 testing and test positivity, including a joint influence of biomedical and social risk factors. We found that mother who were younger, with obesity, and who had preexisting chronic medical conditions were more likely to obtain a COVID-19 test—findings that are consistent with selective testing based on clinical indications or exposure, in the absence of universal testing. After accounting for potential selection bias regarding testing, we identified risk factors for COVID-19 test positivity: lower educational attainment, foreign-born status, and higher BMI. Mothers with 2+ co-existing chronic medical conditions, such as diabetes, hypertension, CHD, CKD, stroke, asthma, or SCD also had a tendency of higher incidence of COVID-19 test positivity, although the association was not significant.
Consistent with previous studies that revealed detrimental effects of obesity on COVID-19 susceptibility [3, 7, 12], our study found that higher BMI was associated with COVID-19 test positivity, independent of other comorbidities. Given the fact that the prevalence of obesity exceeds 42% in the US [24]. where the total number of COVID-19 cases is one of the highest in the world [25], these data emphasize that obesity and the COVID-19 pandemic converged into a co-epidemic. Although the potential underlying mechanisms related to obesity and COVID test positivity are outside the scope of this study, previous studies have documented that individuals with obesity experience sustained low-grade systemic inflammation [26], and impaired adaptive immune response to infection [27]. In addition, obesity is characterized by increased activation of the systemic and local adipose tissue renin–angiotensin–aldosterone system [28], which may link to SARS-CoV-2 to enter into adipocytes [29]. Therefore, an appropriate and timely multidisciplinary approach is needed to address this evident co-epidemic.
Our study also revealed the important role of social factors. We found that mothers without a college education were at increased risk of COVID-19 test positivity. Although we did not have specific information about their occupations, we speculate that mothers with higher education may be less likely to be employed in service-related jobs and more likely to engage in remote work, which may have reduced their potential for virus exposure. Consistent with previous research that reported a higher risk of COVID-19 infection among immigrants [13, 14], our data demonstrated a significantly increased risk of COVID-19 test positivity among foreign-born mothers independent of the effects of age, education, obesity, and chronic medical conditions. Although the exact mechanism underlying this association is unknown, we hypothesize that this is likely due to a combination of social risk factors of COVID-19 exposure and infection shown to be prevalent in foreign-born populations, such as exposure to overcrowded living environments, higher incidence of poverty, and employment in high exposure/contact jobs (i.e., to provide essential services such as health care, or at essential businesses like grocery stores, etc.) where social distancing is challenging (https://read.oecd-ilibrary.org/view/?ref=137_137245-8saheqv0k3&title=What-is-the-impact-of-the-COVID-19-pandemic-on-immigrants-and-their-children%3F). Notably, both education and nativity were not associated with receipt of COVID-19 testing. This finding is consistent with the testing prioritization that was mainly based on clinical indicators, not socio-demographic factors. This study, by accounting for selection for testing, revealed that socio-demographic factors were associated with increased risk of COVID-19 infection.
Previous observational studies have shown conflicting results about the association between chronic medical conditions and COVID-19 infection, perhaps in part due to selectivity of COVID-19 testing [3, 13, 14]. For example, a study conducted by Gu et al. [3]. documented an important influence of selection bias in association between chronic medical conditions and COVID-19 susceptibility. Consistently, our results showed that these same medical conditions, except for diabetes, were significantly associated with COVID-19 testing, which is consistent with testing prioritization of individuals with chronic medical conditions. In our study, when selection factors for COVID-19 testing were corrected by using Heckman selection models, we found a trend but statistically insignificant association between number of chronic medical conditions and COVID-19 test positivity. Interestingly, our data showed that older mothers were less likely to get tested compared with younger mothers. This may be due to experiencing more COVID-related symptoms as a result of providing more caregiving for children and older family members, or needing to work more (as testing could be required by their employers). However, mother’s age was not associated with COVID-19 test positivity, further suggesting the need to take into account selectivity of testing sampling in these analyses. Notably, our study showed a lower risk of COVID-19 test positivity in smokers. Although similar findings have been found in previous studies [3, 8, 13], this result should be considered carefully due to the smoking status in our study reflecting the status during index pregnancy, not current.
Considered together, our findings have important public health implication: First, our study contributes to an understanding of the risk factors for COVID-19 incident risk among a population of low-income middle-age Black and Hispanic mothers. While most COVID-19 studies have focused on high-risk older populations, middle-age mothers are critical to families as caregivers and to society as active contributors to the workforce and economy. Second, our findings support that the obesity pandemic has significantly intersected with and exacerbated the COVID-19 pandemic. Third, our findings illustrate the need for increased attention to the health of immigrant and refugee communities, who are at risk for many preventable health conditions in addition to COVID-19. Finally, our findings indicate that the interplay of biomedical and social factors contributes to and amplifies the impacts of the COVID-19 pandemic, a potential new source of health disparities among the most disenfranchised segments of the US population.
Our study has the following limitations. The study population is a predominantly urban, low-income, primarily Black and Hispanic cohort in Boston, MA. Thus, caution is needed when assessing the generalizability of the findings to other populations with different characteristics. The sample size of our study, particularly those with a positive COVID-19 test, was modest. As a result, we were not able to perform detailed analyses on severity of COVID-19 cases. We did not have information on individual occupations, exposures, or living conditions, nor did we have patient-reported data regarding their decisions to seek testing including symptomatic illness. Our findings remain to be confirmed in larger studies. In addition, we may miss some testing done in other settings outside of BMC and cannot exclude the possibility that some non-tested mothers would have tested positive for COVID-19. Therefore, our findings might be underestimated and real-world findings could, in fact, be even stronger.
The strengths of this study are its prospective cohort design with a well-defined population and baseline characteristics before the pandemic; the availability of data on individual-level COVID-19 testing and test positivity; and a rich database of potential biomedical and social determinants of COVID-19 from a predominantly US urban, low-income cohort of Black and Hispanic mothers, which included a high proportion of immigrants [30]. More importantly, we hope this study will stimulate more research along these lines, with a goal to better understand and improve health and well-being and reduce health disparities among U3 populations now and in the future.
Conclusions
This study demonstrated the intersectionality of obesity and social factors in modulating incident risk of COVID-19 in this sample of US low-income Black and Hispanic middle-aged mothers. The findings further underscore the methodological importance of accounting for test selection factors in order to better estimate risk factors of COVID-19 infection.
References
CDC. Centers for Disease Control and Prevention, Coronavirus Disease 2019 (COVID-19), CDC COVID Dara Tracker. https://covid.cdc.gov/covid-data-tracker/#cases_casesinlast7days. Accessed 19 July 12021.
Millett GA, Jones AT, Benkeser D, Baral S, Mercer L, Beyrer C, et al. Assessing differential impacts of COVID-19 on black communities. Ann Epidemiol. 2020;47:37–44.
Gu T, Mack JA, Salvatore M, Prabhu Sankar S, Valley TS, Singh K, et al. Characteristics associated with racial/ethnic disparities in COVID-19 outcomes in an academic health care system. JAMA Netw Open. 2020;3:e2025197.
Munoz-Price LS, Nattinger AB, Rivera F, Hanson R, Gmehlin CG, Perez A, et al. Racial disparities in incidence and outcomes among patients with COVID-19. JAMA Netw Open. 2020;3:e2021892.
de Lusignan S, Dorward J, Correa A, Jones N, Akinyemi O, Amirthalingam G, et al. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. Lancet Infect Dis. 2020;20:1034–42.
Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). COVID-19 hospitalization and death by rave/ethnicity. 2020. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html. Accessed 23 Nov 2020.
Denova-Gutierrez E, Lopez-Gatell H, Alomia-Zegarra JL, Lopez-Ridaura R, Zaragoza-Jimenez CA, Dyer-Leal DD, et al. The association of obesity, type 2 diabetes, and hypertension with severe coronavirus disease 2019 on admission among Mexican patients. Obesity. 2020;28:1826–32.
Hernandez-Garduno E. Obesity is the comorbidity more strongly associated for Covid-19 in Mexico. A case-control study. Obes Res Clin Pract. 2020;14:375–9.
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. Jama. 2014;311:806–14.
Howard G, Lackland DT, Kleindorfer DO, Kissela BM, Moy CS, Judd SE, et al. Racial differences in the impact of elevated systolic blood pressure on stroke risk. JAMA Intern Med. 2013;173:46–51.
Rentsch CT, Kidwai-Khan F, Tate JP, Park LS, King JT Jr., Skanderson M, et al. Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: a nationwide cohort study. PLoS Med. 2020;17:e1003379.
Ho FK, Celis-Morales CA, Gray SR, Katikireddi SV, Niedzwiedz CL, Hastie C, et al. Modifiable and non-modifiable risk factors for COVID-19, and comparison to risk factors for influenza and pneumonia: results from a UK Biobank prospective cohort study. BMJ Open. 2020;10:e040402.
Castilla J, Guevara M, Miqueleiz A, Baigorria F, Ibero-Esparza C, Navascues A, et al. Risk factors of infection, hospitalization and death from SARS-CoV-2: a population-based cohort study. J Clin Med. 2021;10:2608.
Bergman J, Ballin M, Nordstrom A, Nordstrom P. Risk factors for COVID-19 diagnosis, hospitalization, and subsequent all-cause mortality in Sweden: a nationwide study. Eur J Epidemiol. 2021;36:287–98.
Wang G, Divall S, Radovick S, Paige D, Ning Y, Chen Z, et al. Preterm birth and random plasma insulin levels at birth and in early childhood. JAMA. 2014;311:587–96.
City of Boston. Coronavirus disease (COVID-19) in Boston. https://www.boston.gov/news/coronavirus-disease-covid-19-boston. Accessed 19 July 2021.
Wang X, Zuckerman B, Pearson C, Kaufman G, Chen C, Wang G, et al. Maternal cigarette smoking, metabolic gene polymorphism, and infant birth weight. JAMA. 2002;287:195–202.
Wang G, Hu FB, Mistry KB, Zhang C, Ren F, Huo Y, et al. Association between maternal prepregnancy body mass index and plasma folate concentrations with child metabolic health. JAMA Pediatr. 2016;170:e160845.
Centers for Disease Control and Prevention. Overweight & obesity, defining adult overweight and obesity. https://www.cdc.gov/obesity/adult/defining.html.2020; Accessed 23 Nov. 2020.
Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–e596.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71:2199–269.
Centers for Disease Control and Prevention, Asthma, ICD-9-CM to ICD-10-CM Conversion. https://www.cdc.gov/asthma/data-analysis-guidance/ICD-9-CM-ICD-10-CM.htm. 2019. Accessed 23 Nov 2020.
Toomet O, Henningsen A. Sample selection models in R: package sampleSelection. J Stat Softw. 2008: 27. https://www.jstatsoft.org/v27/i07/.
Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity and severe obesity among adults: United States, 2017–2018. Hyattsville, MD: National Center for Health Statistics; 2020. NCHS Data Brief, no 360.
https://covid19.who.int/. Accessed 10 July 2021.
Fontana L, Eagon JC, Trujillo ME, Scherer PE, Klein S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes. 2007;56:1010–3.
Green WD, Beck MA. Obesity altered T cell metabolism and the response to infection. Curr Opin Immunol. 2017;46:1–7.
Goossens GH, Blaak EE, van Baak MA. Possible involvement of the adipose tissue renin-angiotensin system in the pathophysiology of obesity and obesity-related disorders. Obes Rev. 2003;4:43–55.
Hoffmann M, Kleine-Weber H, Schroeder S, Kruger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–80 e8.
Rasmussen SA, Thompson LA. Coronavirus disease 2019 and children: what pediatric health care clinicians need to know. JAMA Pediatr. 2020;174:743–4.
Acknowledgements
We would like to thank the study participants, the nursing staff at Labor and Delivery of the Boston Medical Center and the field team for their contributions to the Boston Birth Cohort. Linda Rosen, MSEE, and the Clinical Data Warehouse assisted in obtaining relevant clinical information; she was compensated for her time. The Clinical Data Warehouse service is supported by Boston University’s Clinical and Translational Institute and the National Institutes of Health Clinical and Translational Science Award (grant U54-TR001012).
Funding
This work is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number UJ2MC31074, Autism Longitudinal Data Project. The Boston Birth Cohort (the parent study) is supported in part by the March of Dimes PERI grants (20-FY02-56 and 21-FY07-605); and the National Institutes of Health (NIH) grants (2R01HD041702, R01HD086013, R01HD098232, R01ES031272). The information, content and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government.
Author information
Authors and Affiliations
Contributions
GW, DMF, JD, and XW: Designed and conceptualized the study, drafted and revised the manuscript. CP, GM, SR: Acquired data, reviewed and revised the manuscript. GW, XH, and HJ: Performed the analyses. XH, NS, KSK, HJ, JS, TLC, BZ: Interpreted the results, reviewed and revised the manuscript. GW and XW take full responsibility for the analyses and content presented in this manuscript. All authors approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
The authors would like to dedicate this manuscript in memory of the late Kwang Sik Kim, MD, who was a giant in the field of infectious diseases. He will be greatly missed and remembered fondly.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Wang, G., Foney, D.M., DiBari, J. et al. A prospective cohort study on the intersectionality of obesity, chronic disease, social factors, and incident risk of COVID-19 in US low-income minority middle-age mothers. Int J Obes 45, 2577–2584 (2021). https://doi.org/10.1038/s41366-021-00943-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-021-00943-x
