
Abstract
Background/objectives
Patients with obesity and lipedema commonly are misdiagnosed as having lymphedema. The conditions share phenotypic overlap and can influence each other. The purpose of this study was to delineate obesity-induced lymphedema, obesity without lymphedema, and lipedema in order to improve their diagnosis and treatment.
Subjects/methods
Our Lymphedema Center database of 700 patients was searched for patients with obesity-induced lymphedema (OIL), obesity without lymphedema (OWL), and lipedema. Patient age, sex, diagnosis, cellulitis history, body mass index (BMI), and treatment were recorded. Only subjects with lymphoscintigraphic documentation of their lymphatic function were included.
Results
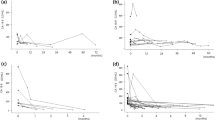
Ninety-eight patients met inclusion criteria. Subjects with abnormal lymphatic function (n = 46) had a greater BMI (65 ± 12) and cellulitis history (n = 30, 65%) compared to individuals with normal lymphatic function [(BMI 42 ± 10); (cellulitis n = 8, 15%)] (p < 0.001). Seventeen patients had a history of lipedema and two exhibited abnormal lymphatic function (BMI 45, 54). The risk of having lower extremity lymphedema was predicted by BMI: BMI < 40 (0%), 40–49 (17%), 50–59 (63%), 60–69 (86%), 70–79 (91%), ≥80 (100%). Five patients with OIL (11%) underwent resection of massive localized lymphedema (MLL) or suction-assisted lipectomy. Three individuals (18%) with lipedema were treated with suction-assisted lipectomy.
Conclusions
The risk of lymphedema in patients with obesity and lipedema can be predicted by BMI; confirmation requires lymphoscintigraphy. Individuals with OIL are at risk for cellulitis and MLL. Patients with a BMI > 40 are first managed with weight loss. Excisional procedures can further reduce extremity size once BMI has been lowered.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Schook CC, Mulliken JB, Fishman SJ, Alomari AI, Grant FD, Greene AK. Differential diagnosis of lower extremity enlargement in pediatric patients referred with a diagnosis of lymphedema. Plast Reconstr Surg. 2011;127:1571–81.
Maclellan RA, Couto RA, Sullivan JE, Grant FD, Slavin SA, Greene AK. Management of primary and secondary lymphedema: analysis of 225 referrals to a center. Ann Plast Surg. 2015;75:197–200.
Greene AK, Grant FD, Slavin SA. Lower-extremity lymphedema and elevated body-mass index. N Engl J Med. 2012;366:2136–7.
Executive Committee. The diagnosis and treatment of peripheral lymphedema: 2016 consensus document of the international society of lymphology. Lymphology. 2016;49:170–84.
Rudkin GH, Miller TA. Lipedema: a clinical entity distinct from lymphedema. Plast Reconstr Surg. 1994;94:841–7.
Child AH, Gordon KD, Sharpe P, Brice G, Ostergaard P, Jeffery S, et al. Lipedema: an inherited condition. Am J Med Genet Part A. 2010;152:970–6.
Halk AB, Damstra RJ. First Dutch guidelines on lipedema using the international classification of functioning, disability and health. Phlebology. 2017;32:152–9.
Bauer AT, von Lukowicz D, Lossagk K, Aitzetmueller M, Moog P, Cerny M, et al. New insights on lipedema: the enigmatic disease of the peripheral fat. Plast Reconstr Surg. 2019;144:1475–84.
Greene AK, Grant FD, Slavin SA, Maclellan RA. Obesity-induced lymphedema: clinical and lymphoscintigraphic features. Plast Reconstr Surg. 2015;135:1715–9.
Hassanein AH, Maclellan RA, Grant FD, Greene AK. Diagnostic accuracy of lymphoscintigraphy for lymphedema and analysis of false-negative tests. Plast Reconstr Surg - Glob Open. 2017;5:e1396.
Szuba A, Shin WS, Strauss HW, Rockson S. The third circulation: radionuclide lymphoscintigraphy in the evaluation of lymphedema. J Nucl Med. 2003;44:43–57.
Maclellan RA, Zurakowski D, Voss S, Greene AK. Correlation between lymphedema disease severity and lymphoscintigraphic findings: a clinical-radiologic study. J Am Coll Surg. 2017;225:366–70.
Lowry R. VassarStats: website for statistical computation. 2019. http://vassarstats.net/.
Maclellan RA, Zurakowski D, Grant FD, Greene AK. Massive localized lymphedema: a case-control study. J Am Coll Surg. 2017;224:212–6.
Greene AK, Grant FD, Maclellan RA. Obesity-induced lymphedema nonreversible following massive weight loss. Plast Reconstr Surg Glob Open. 2015;3:e426.
Greene AK, Maclellan RA. Operative treatment of lymphedema using suction-assisted lipectomy. Ann Plast Surg. 2016;77:337–40.
Greene AK, Voss SD, Maclellan RA. Liposuction for swelling in patients with lymphedema. N Engl J Med. 2017;377:1788–9.
Peled AW, Slavin SA, Brorson H. Long-term outcome after surgical treatment of lipedema. Ann Plast Surg. 2012;68:303–7.
Couto JA, Maclellan RA, Greene AK. Management of vascular anomalies and related conditions using suction-assisted tissue removal. Plast Reconstr Surg. 2015;136:511e–4e.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Greene, A.K., Sudduth, C.L. Lower extremity lymphatic function predicted by body mass index: a lymphoscintigraphic study of obesity and lipedema. Int J Obes 45, 369–373 (2021). https://doi.org/10.1038/s41366-020-00681-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-020-00681-6
