
Abstract
Introduction:
This study examined whether spectral analysis of the electroencephalogram (EEG) can discriminate between mild and severe hypoxic–ischemic injury in the immature brain.
Results:
Total EEG power was profoundly suppressed after umbilical cord occlusion and recovered to baseline by 5 h after 15-min of occlusion, in contrast with transient recovery in the 25-min (P < 0.05). Power spectra were not different between groups in the first 3 h; α and β power were significantly higher in the 15-min group from 4 h, and Δ and θ power from 5 h (P < 0.05). The 25-min group showed severe neuronal loss in hippocampal regions and basal ganglia at 3 days, in contrast with no/minimal injury in the 15-min group.
Discussion:
EEG power after asphyxia did not discriminate between mild and severe injury in the first 3 h in preterm fetal sheep. Severe subcortical neural injury was associated with persistent loss of high-frequency activity.
Methods:
Chronically instrumented fetal sheep at 0.7 gestation (101–104 days; term is 147 days) received either 15-min (n = 13) or 25-min (n = 13) of complete umbilical cord occlusion. The Δ (0–3.9 Hz), θ (4–7.9 Hz), α (8–12.9 Hz), and β (13–22 Hz) components of the EEG were determined by power spectral analysis. Brains were taken at 3 days for histopathology.
Similar content being viewed by others

Main
Premature birth is associated with a high rate of abnormal neurodevelopmental outcomes (1). In the first 48 h after premature birth abnormal electroencephalogram (EEG) activity, including seizures, is common and is associated with adverse outcome (2). For potential trials of neuroprotection, it is essential to identify infants with a high risk of adverse outcome as early as possible in the first 6 h of life (3). Amplitude-integrated EEG is an easily applied bedside technology that at term can be used to identify high-risk infants after neonatal hypoxia–ischemia (4). However, there is increasing evidence that abnormal patterns may be associated with rather variable outcomes (5,6) and that initially abnormal amplitude-integrated EEG patterns shortly after birth can recover to normal within 24 h (7,8). The mechanism of this rapid recovery is unclear. Moreover, there is relatively limited information on neurophysiological recovery after asphyxia in preterm infants (9), when important visual prognostic markers such as sleep–wake cycling have not yet developed (10).
An alternative approach to amplitude or pattern analysis is power spectral analysis of the continuous EEG, which provides relative and absolute power in defined frequency bands. Studies in adults suggest that lower-frequency activity recovers more rapidly than higher-frequency activity after cardiac surgery (11). In one study, lower frequency of the EEG was associated with adverse prognosis in preterm infants (12), although others have not reproduced this association (13). The purpose of this study was therefore to test whether recovery of EEG spectral power in the first 6 h after short or prolonged asphyxia in preterm fetal sheep at 0.7 gestation could predict subsequent neural injury. Brain development at this age is broadly consistent with 28 to 32 wk in humans, before the development of cortical myelination (14). The fetal EEG at this age is consistent with that of the preterm human infant, with discontinuous mixed-frequency activity with periods of quiescence (the so called interburst interval) alternating with periods of high-amplitude slow-wave activity (15,16).
Results
Metabolic
Umbilical cord occlusion was associated with profound hypoxemia with a rapid and progressive respiratory and metabolic acidosis that was greater with more prolonged occlusion ( Table 1 ). Two hours after release of occlusion, the metabolic and respiratory acidosis had resolved in both groups; 72 h after occlusion partial pressure of CO2 and HCO3− were slightly lower in the 25-min group.
Cardiovascular Variables
There were no significant baseline differences. At the end of occlusion, mean arterial pressure was significantly lower in the 25-min group than the 15-min group (11.1 ± 1.1 vs. 15.9 ± 1.6 mmHg, P < 0.05), as were fetal heart rate (59.8 ± 3.8 beats per min (bpm) vs. 94.5 ± 7.1 bpm, P < 0.01) and carotid blood flow (24.1 ± 2.4% vs. 46.0 ± 3.3% of baseline, P < 0.005). After release of occlusion, both groups showed transient hyperperfusion, hypertension, and tachycardia, which resolved much more rapidly in the 15-min group (P < 0.001, Figure 1 ). Delayed cerebral hypoperfusion occurred in both groups (p < 0.05); the 25-min group showed significantly more rapid onset and greater duration of hypoperfusion than the 15-min group (P < 0.001).

The time sequence of changes in mean arterial blood pressure (MAP, mmHg top panel), fetal heart rate (FHR, beats per minute (bpm), middle panel), and carotid blood flow (CaBF, ml/min, bottom panel) after 15 min (open circles) or 25 min of umbilical cord occlusion (filled circles). Data are 1 min averages from 5 min before until 15 min after occlusion then 10 min averages from 40 min to 72 h after asphyxia. Data are mean ± SEM. EMG, electromyogram. *P < 0.05, 15 min vs. 25 min.
Continuous EEG
EEG activity before occlusion in both groups showed a typical pattern of discontinuous mixed-frequency activity, with bursts alternating with periods of reduced activity ( Figure 2 ). After occlusion, the EEG was markedly suppressed in both groups for the first 3 h; however, low-amplitude epileptiform transients were seen in the 25-min group but not the 15-min group. From 4 h onward, there was progressive recovery of background EEG activity in the 15-min group, whereas the 25-min group showed very abnormal, low-frequency activity, and, from 6 h, many developed overt seizures.

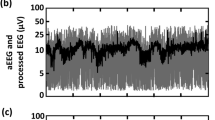
Examples of continuous electroencephalogram (EEG). (a) Discontinuous mixed-frequency activity prior to asphyxia; (b) 2 h after asphyxia, 15-min group; (c) 2 h after asphyxia, 25-min group; (d) 6 h after asphyxia, 15-min group; (e) 6 h after asphyxia, 25-min group (note the different y-axis scale required to show the large-amplitude seizure); (f) 72 h after asphyxia, 15-min group; (g) 72 h after asphyxia, 25-min group.
Total EEG Power, Spectral Edge, and Nuchal Electromyogram Activity
There were no significant baseline differences. Immediately after occlusion, both groups showed profound suppression of total EEG power, with no significant difference between groups until 5 h after asphyxia. The 15-min group showed progressive and sustained recovery of total power to baseline values by 5 h after occlusion (P < 0.005, Figure 3 ). In contrast, the 25-min group showed relatively delayed recovery of total power with reduced power relative to the 15-min group at 5 and 6 h and a transient return to baseline values, with maximal power at 10 h, followed by severely reduced EEG power from 18 h until the end of the study as compared with either baseline values or the 15-min group (P < 0.001). Inspection of the continuous EEG recordings confirmed that the secondary increase in power in the 25-min group corresponded closely with the appearance of intense delayed seizures, similar to previous studies of this paradigm (17). The median seizure onset was 407 (range 307–1,663) min after occlusion, mean duration was 56.2 ± 6.0 s, and mean power was 175 ± 24.9 µV2 ( Figure 3 ). No seizures were observed in the 15-min group.

Time per hour having seizures, total electroencephalogram (EEG) power, spectral edge, and nuchal electromyogram activity before and after 15 min (open circles) or 25 min of umbilical cord occlusion (filled circles). Data are mean ± SEM. *P < 0.05 between groups.
Spectral edge progressively recovered to baseline values by 26 h in the 15-min group but did not recover in the 25-min group. Spectral edge was higher in the 25-min group at 2 h but then remained lower than in the 15-min group from 6 h ( Figure 3 ). Nuchal electromyogram (EMG) activity showed a progressive recovery to baseline within 4 h in the 15-min group ( Figure 1 ). The 25-min group showed a tri-phasic pattern and was below baseline at 1, 5–11, and 26–40 h and above baseline from 66–72 h. Nuchal EMG was significantly higher from 6 to 8 h in the 15-min group. Within subjects regression between nuchal EMG and the proportion of θ activity in the first 36 h showed a weak but highly significant relationship in the 25-min group only (r2 = 0.07, P < 0.001).
Power in Spectral Bands
Recovery of spectral band power broadly followed the changes in overall power. The 15-min group showed rapid recovery of low-frequency (Δ) power, followed by progressive recovery of higher-frequency bands ( Figure 4 ). Δ power returned to baseline values by 5 h after asphyxia, whereas θ power recovered by 18 h, α power by 22 h, and β power by 33 h after occlusion (P < 0.05). In contrast, the 25-min group showed a transient increase of Δ power to baseline values, paralleling the total EEG power, but the higher-frequency bands remained suppressed until the end of recordings at 72 h. In the 15-min group, Δ power was significantly greater than in the 25-min group after 5–6 h and from 23–72 h (P < 0.05), θ power from 5 h, and α and β power from 4 h (P < 0.01).

Time course of total and percent EEG power in frequency bands before and after 15 min (open circles) or 25 min of umbilical cord occlusion (filled circles). (a) Δ-power (μV2, first panel), θ-power (μV2, second panel), α-power (μV2, third panel), β-power (μV2, fourth panel). Data are mean ± SEM. *P < 0.05 between groups. (b) Proportion of electroencephalogram activity in Δ (0–3.9 Hz), θ (4–7.9 Hz), α (8–12.9 Hz), and β (13–22 Hz) frequency bands. Data are mean ± SEM. *P < 0.05 between groups. EEG, electroencephalogram.
Relationship Between Carotid Blood Flow and β Spectral Power
Both groups showed secondary hypoperfusion; this recovered by the end of the first day in the 15-min group, whereas carotid blood flow remained suppressed in the 25-min group until the end of the study. These changes showed a significant within-subjects correlation with recovery of β power after asphyxia in both the 15-min (r2 = 0.50, P < 0.0001) and the 25-min groups (r2 = 0.25, P < 0.0001).
Percentage of Power in Spectral Bands
As shown in Figure 4 , EEG power was predominantly (62.5 ± 3.4%) in the lowest-frequency (Δ) band. After occlusion, there was a marked increase in the proportion of Δ power in both groups; this completely recovered over the first 20 h in the 15-min group but not the 25-min group (P < 0.05 vs. baseline). Conversely, the proportion of θ, α, and β activity recovered progressively in the 15-min group only, and the percentage of θ activity was greater from 5–10 h and 15–72 h whereas α and β activity were significantly greater in the 15-min group from 5 h until the end of recordings (P < 0.05).
EEG Continuity
EEG continuity >25 µV was profoundly suppressed for the first 3 h after occlusion in both groups, but from 4 h onward it recovered much more rapidly in the 15-min group than in the 25-min group ( Figure 3 , P < 0.05) and was not significantly different from baseline values by 13 h after occlusion. In contrast, continuity remained significantly lower than baseline for the duration of the experiment in the 25-min group, with only a partial relative improvement starting approximately 36 h after occlusion.
Histopathology
Fifteen minutes of complete umbilical cord occlusion was associated with no or minimal selective neuronal loss only in subcortical neuronal structures ( Figure 5 ). In contrast, 25-min of occlusion was associated with severe neuronal loss in subcortical neuronal structures, particularly in the dorsolateral aspect of the basal ganglia and the cornu ammonis (CA) regions of the dorsal horn of the hippocampus at 3-d recovery ( Figure 5 , P < 0.05 vs. 15-min group, repeated-measures ANOVA). There was only trivial neuronal loss in the cortex, typically only a few cells in the parasagittal gyri even in the 25-min group.

Effect of 25-min or 15-min complete umbilical cord occlusion on neuronal loss, assessed by light microscopy 3 days after recovery from occlusion. Photomicrographs of the caudate nucleus of the basal ganglia and CA3 region of the hippocampus in the (a) 15-min and (b) 25-min groups. Black arrows indicate examples of dead cells exhibiting ischemic cell change with nuclear condensation and acid fuchsin (pink) staining of the cytoplasm. White arrows indicate examples of viable (thionin-stained) cells. Scale bar = 40 µm. (c) Neuronal loss in the 15-min (open bars) and 25-min occlusion groups (filled bars). Data are mean ± SEM. *P < 0.05. CA, cornu ammonis; DG, dentate gyrus; PSC, parasagittal cortex.
Discussion
Effective neuroprotection after acute hypoxia-ischemia with nearly all experimental therapies so far appears to require intervention within approximately 6 h of the insult, with far better protection with earlier treatment (3). Thus, it is critical to find ways of identifying injured infants as soon as possible in the early recovery phase (18). Disappointingly, this study shows that in preterm fetal sheep, total EEG power and power in each of the spectral bands was identically and profoundly suppressed for the first 3 h after both a prolonged (25-min) insult that induced extensive subcortical neural injury and the much shorter (15-min) insult that was associated with little or no injury. The normal burst-suppression pattern of the preterm EEG was profoundly suppressed after occlusion and recovered in a similar pattern to spectral power, ranging from approximately 4 h in the mild group to more than 36 h in the severe group.
It is notable that whereas higher-frequency power and the continuity of the EEG recovered 4 h after the mild insult, high-frequency power remained suppressed throughout the 72-h recovery period after severe injury, with only partial recovery of EEG continuity. In this study, both total and Δ power showed a transient “recovery” from 7 to nearly 23 h after the 25-min occlusion. This confounding increase corresponded with the development of delayed seizures, similar to previous reports of this paradigm (17,19,20). Even after resolution of seizures, although total EEG power did improve in part, the severe injury group showed a continuing disproportionate percentage of low-frequency (Δ) power. This is broadly consistent with the previous finding in near-term fetal sheep that asphyxia induced by repeated umbilical cord occlusions was associated with persistent loss of θ and α activity, with basal ganglia damage (21).
Movement artifact is another potential confounding factor for neonatal EEG recordings. In this preclinical study, we minimized this with driven-shield electrodes, provision of a relatively large area for the ground electrode at surgery, and electrical isolation of the recording amplifier/filters (22). In contrast, the neonatal intensive care unit is a much less well-controlled environment. Artifacts due to seizures, rapid/deep respiration, and electronic noise are common and may introduce both larger-amplitude, low-frequency activity and higher-frequency components (23). Such noise could confound quantitative analysis as used in this study, unless the continuous EEG recording is carefully monitored as well.
These findings are consistent with studies in term infants that have highlighted that initially abnormal amplitude-integrated EEG patterns shortly after birth sometimes recover to normal within 24 h (7,8). The specific mechanisms of this early transient suppression are unclear. Potentially, it could be related to early or reversible neural injury (24). Other key factors likely include time required for recovery of aerobic metabolism after profound anoxia, active endogenous suppression of neuronal activity, and dysregulation of cortical activity secondary to subcortical injury.
The rapid EEG suppression at the onset of asphyxia is actively mediated through adenosine and other inhibitory neuromodulators in near-term fetal sheep (25). However, the continuing suppression after approximately the first 3 min is mediated by profound depletion of high-energy phosphates as measured by magnetic resonance spectroscopy in the piglet (26), and inhibition of mitochondrial cytochrome oxidase activity in preterm fetal sheep (27). In turn, this metabolic failure leads to cell swelling (cytotoxic edema) that may be measured by increased brain impedance (27). In fetal sheep, the increase in impedance during asphyxia or ischemia peaks approximately 10 min after reperfusion and takes 30 to 60 min to resolve (27,28). By 2 h after release of occlusion in the current paradigm, cytochrome activity and impedance are normal (15,27). Thus, metabolic failure cannot explain continuing EEG suppression.
There is some evidence that actively mediated suppression continues after asphyxia. After release of occlusion, a secondary (i.e., delayed) reduction in brain blood flow is common at all ages. In near-term fetal sheep, this phase is associated with significantly increased tissue oxygen levels, reduced cerebral oxygen extraction, and suppression of cerebral metabolism (28,29). The hypoperfusion is actively mediated, as in the current paradigm, α-adrenoreceptor blockade prevents the secondary hypoperfusion and advances the onset of postasphyxial seizures (30). Furthermore, selective blockade of inhibitory α-2-adrenoreceptors after asphyxia is associated with increased (but rather abnormal) cortical EEG activity, with greater neuronal damage after 3-d recovery in preterm fetal sheep (31). Other inhibitory neuromodulators are also likely to be important; for example, inhibition of endogenous neurosteroid activity increases neural injury after asphyxia in near-term fetal sheep (32). This period of active suppression typically resolves after approximately 6 to 8 h (29), corresponding with the onset of delayed seizures ( Figure 3 ), and a transition to relative or absolute hyperperfusion as measured by near-infrared spectroscopy (15).
These data suggest that secondary hypoperfusion is associated with a protective, active inhibition of brain activity (31). Consistent with this, there was a strong within-subject correlation between secondary hypoperfusion of carotid blood flow and delayed recovery of high-frequency activity. Critically, in the 15-min group, the return of high-frequency activity to baseline values ( Figure 3 ) corresponded closely with the recovery of carotid blood flow ( Figure 1 ). The one apparent disconcordant feature was the postasphyxial EEG suppression in the hour after asphyxia during transient hyperperfusion; however, this is consistent with the known delay before restoration of neuronal metabolism discussed earlier.
Finally, it is notable that the severe insult was associated with sparing of the cortex, despite severe subcortical injury (33), consistent with patterns seen on magnetic resonance imaging after severe asphyxia in preterm infants (34). The persistent EEG suppression in this group without neuronal loss in the underlying cortex implies that subcortical injury must impair cortical activity. There is some evidence, for example, that even in adults, damage or dysfunction of the medullary reticular formation impairs thalamo–cortical interactions (35) and is associated with slower EEG waveforms both during and immediately after asphyxia.
Conclusion
This study suggests that quantitative EEG analysis can provide information on injury severity and timing of hypoxic-ischemic injury in preterm fetuses because a persistent loss of power in the higher-frequency bands from 4 or more hours after birth was associated with significant neural injury. The finding that in the first 3 h after asphyxia the EEG was suppressed after both mild and severe insults sheds some light on the limitations of early EEG monitoring for recruitment in clinical trials. Thus, although this objective, quantitative methodology appears to have some value, it is likely that it will need to be a part of a multimodal approach, perhaps including examination of the unfiltered continuous EEG or biochemical parameters, for recruitment of preterm infants for trials of neuroprotection (36).
Methods
Experimental Preparation
All procedures were approved by the Animal Ethics Committee of Auckland University, New Zealand. Twenty-six Romney/Suffolk fetal sheep (98–99 days gestation; term = 147 days) were operated on using sterile techniques. Ewes were given 5 ml of Streptocin (procaine penicillin (250,000 IU) and dihydrostreptomycin (250 mg/ml), Stockguard Labs, Hamilton, New Zealand) intramuscularly for prophylaxis 30 min prior to surgery. Anesthesia was induced by intravenous injection of Alfaxan (alphaxalone, 3 mg/kg, Jurox, Rutherford, Australia) and maintained using 2–3% isoflurane in oxygen.
Following a maternal midline abdominal incision and exteriorization of the uterus, fetal catheters were placed in the left femoral artery and vein, right brachial artery and vein, and the amniotic sac for the recording of blood pressure and blood sampling. Electrocardiograph electrodes were sewn across the chest to record fetal heart rate. An ultrasonic blood flow probe (size 3S; Transonic Systems, Ithaca, NY) was placed around the left carotid artery to measure carotid blood flow as an index of global cerebral blood flow (25,37). Two pairs of EEG electrodes (AS633-7SSF, Cooner Wire, Chatsworth, CA) were placed on the dura bilaterally over the parasagittal parietal cortex (5 mm and 10 mm anterior to bregma and 5 mm lateral). A reference electrode was sewn over the occiput. Electromyographic electrodes were placed in the nuchal muscle to measure EMG activity. The fetus was then retracted slightly to expose the umbilical cord. A 16-mm internal diameter silastic inflatable umbilical cord occluder (In Vivo Metric, Healdsburg, CA) was then placed and secured around it. The fetus was returned to the uterus and all leads exteriorized through the maternal flank. The maternal long saphenous vein was catheterized for postoperative maternal care and euthanasia. Gentamicin (80 mg, Pharmacia and Upjohn, Perth, Australia) was administered into the amniotic sac prior to uterus closure.
After surgery, sheep were housed together in separate metabolic cages with access to water and food ad libitum, in a temperature-controlled room (16 ± 1 °C, humidity 50 ± 10%) with a 12 h light/dark cycle. Antibiotics were administered daily for 4 d intravenously to the ewe, comprising 2 d of gentamicin (80 mg), and 4 d of benzylpenicillin (600 mg benzylpenicillin sodium, Novartis, Auckland, New Zealand). Fetal arterial blood was taken daily for blood gas analysis for assessment of fetal condition. Fetal catheters were maintained patent by continuous heparinized isotonic saline infusion (20 IU/ml at 0.2 ml/h).
Recordings
Movement artifact was reduced by using driven-shield electrodes, constructed from shielded Teflon-insulated wire (AS633-7SSF, Cooner Wire, Chatsworth, CA) (22). All signals were acquired at 512 Hz, processed online, and stored to disk as 1-min averaged intervals by custom software (Labview for Windows, National Instruments, Austin, TX). Fetal mean arterial pressure, corrected for maternal movement by subtraction of amniotic fluid pressure (Novatrans II MX860, Medex, Hilliard, OH), fetal heart rate, and EEG were recorded continuously from 12 h before umbilical cord occlusion until 72 h afterward. The EEG signal was high-pass filtered at 1.6 Hz and low-pass filtered at 50 Hz and then stored for offline analysis at a sampling rate of 256 Hz. The high-pass filter had a first-order roll-off of 6 dB per octave, thus attenuating but not removing frequencies below this. Total EEG power (µV2) was calculated from the intensity spectra. Quantitative EEG measurements for each waveform were performed to quantify power in the Δ (0–3.9 Hz), θ (4–7.9 Hz), α (8–12.9 Hz), and β (13–22 Hz) bands. This involved calculating power spectra (by fast Fourier transform) of the EEG on sequential epochs, using a 10 s Hanning window to minimize spectral leakage. The continuous EEG recording was assessed for continuity by quantifying the percentage of time per minute the EEG amplitude was >25 µV.
Experimental Protocol
Experiments were conducted at 103–104 d gestation following 4 to 5 d postoperative recovery. Fetuses were randomly assigned to either 25-min (n = 13) or 15-min (n = 13) umbilical cord occlusion. Fetal arterial blood was taken 5 min before occlusion, 5 min and 12 min (15-min group) or 17 min (25-min group) during occlusion, and 2, 24, 28, and 72 h after occlusion. Blood samples were tested for pH and blood gas determination, acid–base balance (Ciba-Corning Diagnostics 845 Blood Gas Analyzer/Co-oximeter, East Walpole, MA), and glucose/lactate measurements (YSI 2300, Yellow Springs Instruments, Yellow Springs, OH).
Tissue Preparation
Three days after asphyxia the ewes and fetuses were killed with sodium pentobarbital (9 g intravenously to ewe; Pentobarb 300, Provet Pty, New Zealand). Fetal brains were perfusion-fixed in situ with 0.9% saline solution then 10% phosphate-buffered formalin (500 ml) and then removed and fixed for a further 3 d before processing and paraffin embedding (33). Coronal sections (10 µm) were taken for immunohistochemistry.
Histology
For assessment of neuronal loss, brain sections (n = 7 in the 25-min group and n = 6 in the 15-min group) were labeled with acid fuchsin-thionin. Prior to labeling, slides were deparaffinized in xylene (2 × 15 min), rehydrated in a series of ethanol concentrations (100%, 95%, 70% for 5 min each), and then washed in distilled water for 1 × 2 min. Sections were then labeled with thionin acetate (Sigma-Aldrich Pty.) for 1 × 12 min, dipped in distilled water to wash, then acid fuchsin for 1 × 35 s, followed by a quick wash in distilled water. The sections were then dehydrated (dipped in 2 × 95% ethanol, 1 × 100% ethanol, 2 min in 100% ethanol, xylene 2 × 15 min) and mounted.
Brain regions of the forebrain used for analysis included the midstriatum (comprising the caudate nucleus and putamen), and the parasagittal cortex, which were assessed on sections taken 26 mm anterior to stereotaxic zero, according to the stereological atlas of the preterm fetal sheep (38). The CA of the dorsal horn of the anterior hippocampus (divided into CA1/2, CA3, CA4, and dentate gyrus) were assessed on sections taken 17 mm anterior to stereotaxic zero.
Neuronal loss was scored on acid fuchsin-thionin–stained sections by light microscopy at ×10 or ×20 magnification on a Nikon 80i microscope with a motorized stage and Stereo investigator software v.8 (Microbrightfield Inc., Williston, VT) using seven fields in the striatum (four in the caudate nucleus, three in the putamen), and one field in each of the hippocampal divisions and the parasagittal cortex. The proportion of neurons showing ischemic cell change as shown by nuclear condensation and acid fuchsin (pink) staining of the cytoplasm in each brain region was scored on a 6-point scale as follows: 0 = no dead neurons; 5 = >0% to 10%; 30 = >10% to 50%; 70 = >50% to 90%; 95 = 90% to <100%; and 100 = 100% dead neurons (28). For each animal, average scores from one section across both hemispheres were calculated for each region.
Data Analysis
Offline analysis of the physiological data was performed using customized analysis programs developed in our laboratory using the Labview data acquisition environment. Seizures were identified visually from the raw EEG and defined as the concurrent appearance of sudden, repetitive, evolving stereotyped waveforms in the EEG signal lasting more than 10 s and of an amplitude greater than 20 μV (39). Physiological data were evaluated by ANOVA with time as a repeated measure (SPSS v15, SPSS, Chicago, IL) followed by one-way ANOVA post hoc test when a significant overall effect was found. Blood gas data were assessed by one-way ANOVA at each time point. Where baseline differences were found, an analysis of covariance was used in subsequent tests with baseline as a covariate. The relationships between secondary hypoperfusion and changes in high-frequency (β) power, and nuchal EMG and the proportion of θ activity were examined by within-subjects regression, correcting for multiple comparisons using the method of Bland and Altman (40). Histopathology data were compared with one-way ANOVA. Statistical significance was accepted when P < 0.05. Data are mean ± SEM.
Statement of Financial Support
This study was supported by the Health Research Council of New Zealand. P.P.D. is supported by the New Zealand Neurological Foundation W&B Miller Doctoral Scholarship.
References
Behrman RE, Butler AS. Committee on Understanding Premature Birth and Assuring Healthy Outcomes. Preterm Birth: Causes, Consequences, and Prevention. Washington DC, USA: Institute of Medicine of the National Academies; 2007. <http://books.nap.edu//catalog/11622.html#toc:>.
Logitharajah P, Rutherford MA, Cowan FM . Hypoxic-ischemic encephalopathy in preterm infants: antecedent factors, brain imaging, and outcome. Pediatr Res 2009;66:222–9.
Gunn AJ, Thoresen M . Hypothermic neuroprotection. NeuroRx 2006;3:154–69.
Gluckman PD, Wyatt JS, Azzopardi D, et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet 2005;365:663–70.
Sarkar S, Barks JD, Donn SM . Should amplitude-integrated electroencephalography be used to identify infants suitable for hypothermic neuroprotection? J Perinatol 2008;28:117–22.
Thoresen M, Hellström-Westas L, Liu X, de Vries LS . Effect of hypothermia on amplitude-integrated electroencephalogram in infants with asphyxia. Pediatrics 2010;126:e131–9.
ter Horst HJ, Sommer C, Bergman KA, Fock JM, van Weerden TW, Bos AF . Prognostic significance of amplitude-integrated EEG during the first 72 hours after birth in severely asphyxiated neonates. Pediatr Res 2004;55:1026–33.
van Rooij LG, Toet MC, Osredkar D, van Huffelen AC, Groenendaal F, de Vries LS . Recovery of amplitude integrated electroencephalographic background patterns within 24 hours of perinatal asphyxia. Arch Dis Child Fetal Neonatal Ed 2005;90:F245–51.
Hellström-Westas L, Klette H, Thorngren-Jerneck K, Rosén I . Early prediction of outcome with aEEG in preterm infants with large intraventricular hemorrhages. Neuropediatrics 2001;32:319–24.
Osredkar D, Toet MC, van Rooij LG, van Huffelen AC, Groenendaal F, de Vries LS . Sleep-wake cycling on amplitude-integrated electroencephalography in term newborns with hypoxic-ischemic encephalopathy. Pediatrics 2005;115:327–32.
Visser GH, Wieneke GH, Van Huffelen AC, De Vries JW, Bakker PF . The development of spectral EEG changes during short periods of circulatory arrest. J Clin Neurophysiol 2001;18:169–77.
Inder TE, Buckland L, Williams CE, et al. Lowered electroencephalographic spectral edge frequency predicts the presence of cerebral white matter injury in premature infants. Pediatrics 2003;111:27–33.
Wong FY, Barfield CP, Walker AM . Power spectral analysis of two-channel EEG in hypoxic-ischaemic encephalopathy. Early Hum Dev 2007;83:379–83.
McIntosh GH, Baghurst KI, Potter BJ, Hetzel BS . Foetal brain development in the sheep. Neuropathol Appl Neurobiol 1979;5:103–14.
Bennet L, Roelfsema V, Pathipati P, Quaedackers JS, Gunn AJ . Relationship between evolving epileptiform activity and delayed loss of mitochondrial activity after asphyxia measured by near-infrared spectroscopy in preterm fetal sheep. J Physiol (Lond) 2006;572(Pt 1):141–54.
Davidson JO, Quaedackers JS, George SA, Gunn AJ, Bennet L . Maternal dexamethasone and EEG hyperactivity in preterm fetal sheep. J Physiol (Lond) 2011;589(Pt 15):3823–35.
Dean JM, George SA, Wassink G, Gunn AJ, Bennet L . Suppression of post-hypoxic-ischemic EEG transients with dizocilpine is associated with partial striatal protection in the preterm fetal sheep. Neuropharmacology 2006;50:491–503.
Bennet L, Cowie RV, Stone PR, et al. The neural and vascular effects of killed Su-Streptococcus pyogenes (OK-432) in preterm fetal sheep. Am J Physiol Regul Integr Comp Physiol 2010;299:R664–72.
Dean JM, George S, Naylor AS, Mallard C, Gunn AJ, Bennet L . Partial neuroprotection with low-dose infusion of the alpha2-adrenergic receptor agonist clonidine after severe hypoxia in preterm fetal sheep. Neuropharmacology 2008;55:166–74.
Bennet L, Dean JM, Wassink G, Gunn AJ . Differential effects of hypothermia on early and late epileptiform events after severe hypoxia in preterm fetal sheep. J Neurophysiol 2007;97:572–8.
Pulgar VM, Zhang J, Massmann GA, Figueroa JP . Mild chronic hypoxia modifies the fetal sheep neural and cardiovascular responses to repeated umbilical cord occlusion. Brain Res 2007;1176:18–26.
Williams CE, Gunn AJ, Mallard C, Gluckman PD . Outcome after ischemia in the developing sheep brain: an electroencephalographic and histological study. Ann Neurol 1992;31:14–21.
Neubauer D, Osredkar D, Paro-Panjan D, Skofljanec A, Derganc M . Recording conventional and amplitude-integrated EEG in neonatal intensive care unit. Eur J Paediatr Neurol 2011;15:405–16.
Brown AW, Brierley JB . Anoxic-ischaemic cell change in rat brain light microscopic and fine-structural observations. J Neurol Sci 1972;16:59–84.
Hunter CJ, Bennet L, Power GG, et al. Key neuroprotective role for endogenous adenosine A1 receptor activation during asphyxia in the fetal sheep. Stroke 2003;34:2240–5.
Iwata O, Iwata S, Bainbridge A, et al. Supra- and sub-baseline phosphocreatine recovery in developing brain after transient hypoxia-ischaemia: relation to baseline energetics, insult severity and outcome. Brain 2008;131(Pt 8):2220–6.
Bennet L, Roelfsema V, Dean JM, et al. Regulation of cytochrome oxidase redox state during umbilical cord occlusion in preterm fetal sheep. Am J Physiol Regul Integr Comp Physiol 2007;292:R1569–76.
Gunn AJ, Gunn TR, de Haan HH, Williams CE, Gluckman PD . Dramatic neuronal rescue with prolonged selective head cooling after ischemia in fetal lambs. J Clin Invest 1997;99:248–56.
Jensen EC, Bennet L, Hunter CJ, Power GC, Gunn AJ . Post-hypoxic hypoperfusion is associated with suppression of cerebral metabolism and increased tissue oxygenation in near-term fetal sheep. J Physiol (Lond) 2006;572(Pt 1):131–9.
Quaedackers JS, Roelfsema V, Heineman E, Gunn AJ, Bennet L . The role of the sympathetic nervous system in postasphyxial intestinal hypoperfusion in the pre-term sheep fetus. J Physiol (Lond) 2004;557(Pt 3):1033–44.
Dean JM, Gunn AJ, Wassink G, George S, Bennet L . Endogenous alpha2-adrenergic receptor-mediated neuroprotection after severe hypoxia in preterm fetal sheep. Neuroscience 2006;142:615–28.
Yawno T, Yan EB, Walker DW, Hirst JJ . Inhibition of neurosteroid synthesis increases asphyxia-induced brain injury in the late gestation fetal sheep. Neuroscience 2007;146:1726–33.
Bennet L, Roelfsema V, George S, Dean JM, Emerald BS, Gunn AJ . The effect of cerebral hypothermia on white and grey matter injury induced by severe hypoxia in preterm fetal sheep. J Physiol (Lond) 2007;578(Pt 2):491–506.
Barkovich AJ, Sargent SK . Profound asphyxia in the premature infant: imaging findings. AJNR Am J Neuroradiol 1995;16:1837–46.
Demetrescu M, Steriade M . Reticular alteration of the recovery cycle of the somaesthetic thalamo-cortical complex. Electroencephalogr Clin Neurophysiol 1967;22:572–3.
Bennet L, Booth L, Gunn AJ . Potential biomarkers for hypoxic-ischemic encephalopathy. Semin Fetal Neonatal Med 2010;15:253–60.
Gonzalez H, Hunter CJ, Bennet L, Power GG, Gunn AJ . Cerebral oxygenation during postasphyxial seizures in near-term fetal sheep. J Cereb Blood Flow Metab 2005;25:911–8.
Gluckman PD, Parsons Y . Stereotaxic method and atlas for the ovine fetal forebrain. J Dev Physiol 1983;5:101–28.
Scher MS, Hamid MY, Steppe DA, Beggarly ME, Painter MJ . Ictal and interictal electrographic seizure durations in preterm and term neonates. Epilepsia 1993;34:284–8.
Bland JM, Altman DG . Calculating correlation coefficients with repeated observations: Part 1–Correlation within subjects. BMJ 1995;310:446.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Keogh, M., Drury, P., Bennet, L. et al. Limited predictive value of early changes in EEG spectral power for neural injury after asphyxia in preterm fetal sheep. Pediatr Res 71, 345–353 (2012). https://doi.org/10.1038/pr.2011.80
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2011.80
This article is cited by
-
EEG sharp waves are a biomarker of striatal neuronal survival after hypoxia-ischemia in preterm fetal sheep
Scientific Reports (2018)
-
Synergistic white matter protection with acute-on-chronic endotoxin and subsequent asphyxia in preterm fetal sheep
Journal of Neuroinflammation (2014)
-
Partial Neural Protection with Prophylactic Low-Dose Melatonin after Asphyxia in Preterm Fetal Sheep
Journal of Cerebral Blood Flow & Metabolism (2014)
