
Abstract
S. aureus is a significant cause of late-onset sepsis in neonates. Increasing antibiotic resistance, however, requires additional treatment options. Lysostaphin, an endopeptidase, has that potential. The objective of this study is to compare lysostaphin versus vancomycin against methicillin-resistant Staphylocococcus aureus (MRSA) in a neonatal mouse model. Minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) against MRSA strain USA300 were determined using standard methods. To determine pharmacokinetics, neonatal pups received either vancomycin or lysostaphin intraperitoneal and serum samples were obtained. To evaluate efficacy, pups were infected s.c. and littermates randomized to receive either saline, vancomycin, or lysostaphin intraperitoneal. Pups were observed for survival and growth. Quantitative blood cultures were obtained 24 h after infection. The MIC/MBC for vancomycin and lysostaphin were 0.71/1.19 μg/mL and <0.008/0.015 μg/mL, respectively. Mean lysostaphin concentrations ranged from 2.34 to 8.92 μg/mL. Mean vancomycin concentrations ranged from 1.72 to 11.2 μg/mL. Lysostaphin improved survival compared with placebo (p < 0.00001) and vancomycin (p < 0.03). There was no significant difference in growth among the groups. All treatment regimens resulted in less bacteremia compared with placebo (p < 0.0001). Lysostaphin appears to be more effective than vancomycin in treating MRSA in a neonatal model.
Similar content being viewed by others


Main
Late-onset sepsis is a significant problem among infants in the Neonatal Intensive Care Unit. Staphylococcus aureus is the second most common pathogen for late-onset sepsis among very low birth weight infants, and nearly 20% die as a direct result of the infection (1). In developing countries, neonatal S. aureus bacteremia is even more prevalent, causing nearly a quarter of all bacteremic episodes (2). In comparison to coagulase-negative staphylococci (CONS), S. aureus infections in neonates are associated with greater morbidity and mortality (3). The increasing outbreaks of Methicillin-Resistant Staphylococcus aureus (MRSA) only add to the impact of the disease; both in terms of antibiotic pressure and the associated isolation and infection control costs (4). As a result, the use of empiric vancomycin to treat suspected or confirmed late-onset sepsis is increasing (3). However, the history of S. aureus has been to develop antibiotic resistance and development of vancomycin-intermediate and resistant specimens support this trend (5). Additional therapies for suspected or confirmed neonatal late-onset MRSA infection are needed.
Lysostaphin is one potential candidate. First described in 1964, lysostaphin is an antimicrobial initially isolated from Staphylococcus simulans (6). In 1986, a recombinant form of lysostaphin was reported using a strain of E. coli as the host (7). It is a 27 kD glycylglycine endopeptidase, which cleaves the cross-linking pentaglycine bridges in the cell walls of Staphylococcus species and has been shown effective against S. aureus both in vitro and in vivo (8). Our laboratory has previously shown that lysostaphin is as effective as vancomycin or oxacillin in treating Methicillin-Sensitive Staphylococcocus aureus (MSSA) infection in a neonatal rat model (9). In this study, we describe the effects of lysostaphin against MRSA in vitro and in vivo in a neonatal mouse model compared with vancomycin.
METHODS
Bacteria.
MRSA strain USA 300 (gift from Sheldon Kaplan, M.D., Houston, TX) was used in these experiments. Samples were stored in tryptic soy broth (TSB) at −80°C. Before each experiment, a vial of the organism was thawed, plated on TSB with 5% sheep blood agar, incubated at 37°C for 24 h, and then screened for strain homogeneity. On the day of each experiment, plated organism was incubated in TSB on a shaker for 2 h at 37°C, centrifuged and washed with normal saline (NS), and then reconstituted with NS using OD to a final concentration of 1 × 104 colony forming unit (CFU)/mL. Bacterial concentration was confirmed via quantitative culture.
MIC and MBC.
The minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) for vancomycin was determined using Clinical and Laboratory Standards Institute (CLSI) guidelines (10). To determine the lysostaphin MIC and MBC, the guidelines were modified by adding 0.1% BSA to cation-adjusted Mueller-Hinton Broth as described in the literature (8).
Animals.
Seven-day timed pregnant-inbred FVB albino dams were obtained from Charles River Laboratories (Wilmington, MA). They received antibiotic-free water and food ad libitum and delivered approximately 10 pups each at 21–22 d gestation. Pups remained with their dams for the entire experiment. Approval for the experiments was obtained from the Animal Use Committee at Baylor College of Medicine.
Pharmacokinetics.
Two-day-old littermate pups were randomly assigned to receive intraperitoneal (IP) injections of lysostaphin 15 mg/kg/dose or vancomycin 15 mg/kg/dose in a total volume of about 0.2 mL, at start (time 0) and again 6, 24, and 30 h later. Vancomycin dosing reflects doses used in clinical care (11). The dosing of lysostaphin was based on previous published clinical and laboratory doses (8,12). Blood samples were collected at 1, 5, 7, 23, 25, 29, 31, 48, 72, and 96 h after the initial injection by direct cardiac puncture. To obtain an adequate sample for drug analysis, blood from 2 to 5 pups was pooled for each data point. There were two data points for each time point. Blood samples were centrifuged at 1500 rpm for 10 min, sera removed, and samples stored at −80°C until batch analysis.
Lysostaphin concentration was determined by ELISA (13). In short, a 96-well plate was coated with 100 μL of rabbit anti-lysostaphin (gift from Biosynexus, Gaithersburg, MD, lot 40321) at a concentration of 1 μg/mL for 2 h at room temperature, washed with PBS with 0.01% Tween 20, 100 μL of standard or sample sera were added to each well for 60 min, the plate was washed five times with PBS with 0.01% Tween 20, and then incubated with biotinylated rabbit anti-lysostaphin (gift from Biosynexus, Gaithersburg, MD, lot 4270) and Extravidin (Sigma Chemical Co., 81K4875) for 30 min separately. Substrate tetramethylbenzadine (BioFx, TMBW0100-01) was then added. The plate was read by a kinetic microplate reader and absorbance was converted to lysostaphin concentration using SOFTmax PRO 3.1.1 software from Molecular Devices Corporation.
Vancomycin concentration was determined by competitive inhibition ELISA performed on a VITROS 5, 1 Fusion 2 System (14) by Texas Children's Hospital Pathology Department.
Efficacy.
Two-day-old pups were infected via s.c. injection cephalad to their tail with 1 dose of 2 × 103 CFU of S. aureus (0.2 mL of the previously prepared solution). Based on previous experiments, this bacterial dose is nearly 100% lethal. Littermates were then randomized to four treatment groups. Each group was given a series of four injections of 0.2 mL each. Group 1 received a saline injection, group 2 received vancomycin 15 mg/kg/dose, group 3 received lysostaphin (gift from Biosynexus, Gaithersburg, MD) at 10 mg/kg/dose, and group 4 received lysostaphin at 15 mg/kg/dose. Each pup received IP injections of their assigned treatment at 0.5, 6, 24, and 30 h after infection. Pups were observed for survival and growth for 7 d and weighed 1 h before infection and then daily for 7 d or until death.
Quantitative blood cultures.
In randomly selected litters, quantitative blood cultures were obtained 24 h after infection via cardiac puncture. Approximately 100 μL of blood was obtained, serially diluted in normal saline, and then plated on blood agar plates. After 24-h incubation, colonies were counted on each plate and bacterial blood culture concentration calculated.
Statistical analysis.
Based on prior studies, the efficacy study sample size estimate assumed a vancomycin treatment survival of 25% and a lysostaphin treatment survival of 50%. A two-tailed Fisher's exact test, with a power of 0.8 and a p value of ≤0.05, a sample size of ≥66 pups per group was determined using Calculation for Sample Sizes and Related Problems (version 4.3; Department of Biostatistics & Applied Mathematics, University of Texas MD Anderson Cancer Center [http://biostatistics.mdanderson.org/SoftwareDownload/SingleSoftware.aspx?Software_Id=41].
Treatment groups were compared by the: independent t test for pharmacokinetic and pharmacodynamic parameters; χ2 or Fisher exact tests as appropriate for survival; Kruskal-Wallis test for blood cultures. Growth curves were constructed for individual pups, the slope of each curve was calculated, and a one-way analysis of variance was used to compare the mean slope values for each group. Statistical significance was predefined as p ≤0.05.
To assist us in comparing efficacy, we chose to evaluate the following pharmacodynamic parameters: Time-above-the-MIC, Area under the curve (AUC), the AUC above the MIC, the AUC-to-MIC ratio, and the Peak-to-MIC ratio. The Time-above-the-MIC and the AUC-to-MIC ratio have been found to be important in evaluating drugs like vancomycin which display time-dependent killing (15).
RESULTS
The geometric mean vancomycin MIC and MBC for USA 300 were 0.71 μg/mL (95% CI 0.37–1.34) and 1.19 μg/mL (95% CI 0.69–2.06), respectively. For lysostaphin, the geometric mean MIC and MBC were less than 0.008 μg/mL (95% CI not applicable) and 0.015 μg/mL, respectively, (95% CI not applicable).
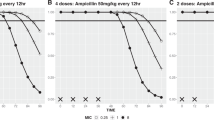
Figure 1a illustrates the mean serum levels of lysostaphin in μg/mL for 96 h. During the 48 h after infection (treatment period) the mean peak serum concentration was 8.92 ± 3.39 μg/mL, and the mean trough concentration was 2.34 ± 0.19 μg/mL. Ninety-six hours after infection, the mean concentration was 0.96 ± 0.59 μg/mL. At no point during the experiment did the mean or any individual measured lysostaphin concentration drop below the MIC.

(A) Serum levels of lysostaphin (μg/mL ± SEM) after injections of lysostaphin 15 mg/kg/dose intraperitoneal at 0 h (first dose), then again 6, 24, and 30 h later. Arrows indicate time of each dose and n = 2 for each time point. Horizontal dotted line represents MIC for USA300: 0.008 μg/mL. Levels ranged from a mean peak concentration of 8.92 ± 3.39 μg/mL, to a mean trough concentration of 2.34 ± 0.19 μg/mL during the 48-h treatment period after infection. (B) Serum levels for vancomycin (μg/mL ± SEM) after injections of vancomycin 15 mg/kg/dose intraperitoneal at 0 h (first dose), then again 6, 24, and 30 h later. Arrows indicate time of each dose and n = 2 for each time point. Horizontal dotted line represents MIC for USA300: 0.71 μg/mL. Levels ranged from a mean peak concentration of 11.2 ± 3.0 μg/mL, to a mean trough concentration of 1.72 ± 0.93 μg/mL during the 48-h treatment period after infection.
Figure 1b illustrates the mean serum levels of vancomycin in μg/mL for 96 h. During the treatment period (48 h after infection), the mean peak serum concentration was 11.2 ± 3.0 μg/mL, and the mean trough concentration was 1.72 ± 0.93 μg/mL. Ninety-six hours after infection, the mean concentration was 0.77 ± 0.02 μg/mL. At no point during the experiment did the mean or any individual measured vancomycin concentration drop below the MIC.
The pharmacodynamic results are depicted in Table 1 and no significant difference was observed between vancomycin and lysostaphin for AUC, AUC above the MIC, AUC to MIC ratio, and Peak to MIC ratio. Although, there appeared to be a trend toward significance for AUC/MIC ratio and Peak to MIC ratio.
Figure 2 illustrates the survival of each of the four groups. Group 1 (control) survival was 6.2% (5 of 81 pups). In group 2 (vancomycin 15 mg/kg), survival was 34% (26 of 77 pups). In group 3 (lysostaphin 10 mg/kg), survival was 41% (32 of 79 pups). In group 4 (lysostaphin 15 mg/kg), survival was 52% (39 of 75 pups). All three treatment groups had significantly improved survival compared with the control group (p < 0.00001). Group 4 (lysostaphin 15 mg/kg) had significantly improved survival compared with group 2 (vancomycin 15 mg/kg) (p = 0.03). We observed no clinical toxicities in the animals who received lysostaphin or vancomycin.

Survival curves for pups in various treatment groups. Pups receiving normal saline injections (▪) (n = 81). Pups receiving vancomycin at 15 mg/kg/dose (▴) (n = 77). Pups receiving lysostaphin at 10 mg/kg/dose (▾) (n = 79). Pups receiving lysostaphin at 15 mg/kg/dose (♦) (n = 75). All three treatment groups had significantly improved survival compared with control (*, p < 0.00001). The group receiving lysostaphin at 15 mg/kg/dose (♦) had significantly improved survival compared with the group receiving vancomycin (▴) (§, p = 0.03).
Figure 3 illustrates the mean growth rate for each treatment group. The average growth rates were 0.23 ± 0.06, 0.67 ± 0.04, 0.59 ± 0.03, and 0.59 ± 0.02 g/d, respectively, for groups 1–4. All three treatment groups (groups 2, 3, and 4) had significantly higher growth rates compared with control (group 1) (p < 0.001), but there was no significant difference between the three treatment groups: between the vancomycin group and the lysostaphin groups at 10 and 15 mg/kg, p = 0.5 and 0.4, respectively, and between the two lysostaphin groups p = 1.

Growth curves for pups in various treatment groups (mean ± SEM). All three treatment groups had significantly higher growth rates compared with the control (normal saline) group (*, p < 0.001). There was no significant difference between the three treatment groups.
Figure 4 illustrates the quantitative blood cultures for each group. The average blood bacterial count was 1.86 ± 0.6 × 104 (n = 10), 1.26 ± 0.2 × 103 (n = 20), 0.93 ± 0.2 × 103 (n = 20), 0.91 ± 0.1 × 103 CFU/mL (n = 24), respectively, for groups 1–4. All three treatment groups (groups 2, 3, and 4) had significantly lower colony counts compared with control (p < 0.0001), but there was no significant difference among each of the three treatment groups, although group 4 trended toward a lower colony count compared with group 2 (p = 0.16).

Quantitative blood cultures from pups in various treatment groups (mean ± SEM). All three treatment groups had significantly lower colony counts compared with control (normal saline) group (§, p < 0.0001). There was no significant difference between the three treatment groups, although: the group receiving lysostaphin at 15 mg/kg/dose trended toward a lower colony count compared with the group receiving vancomycin (**, p = 0.16); the group receiving lysostaphin 10/mg/kg/dose trended toward a lower colony count compared with the group receiving vancomycin (*, p = 0.24).
DISCUSSION
S. aureus infections are the second most common pathogen among very low birth-weight infants, causing about 8% of infections with a mortality rate of 20% (1). MRSA has become an increasing cause of these infections reaching nearly 50% of all S. aureus infections in many neonatal intensive care units (16). With the development of vancomycin-intermediate strains of S. aureus also increasing, there is increased interest in new treatment options (5).
Lysostaphin may prove to be a viable option. Schindler et al. (6) reported that lysostaphin was active against all 54 strains of S. aureus they tested, regardless of whether the bacterium was actively dividing, coagulase-producing, antibiotic resistance, or nosocomial association. To date, very little experience with human subjects has been reported in the literature. Previous experiments have shown that intranasally administered lysostaphin can decrease or eradicate S. aureus colonization of the anterior nares of human adults, children, and infants (17,18). Quickel et al. (18) reported no local or systemic reactions in those who received intranasal lysostaphin. Furthermore, when subjects were injected intradermally with lysostaphin, there was no significant difference in erythema or induration between lysostaphin and control groups. Harris et al. (17) observed no side effects; however, one patient did develop antibodies and had a positive skin test although no clinical evidence of sensitization. In a case of compassionate use, a single 500 mg dose of lysostaphin (approximately 10 mg/kg) was given to an adult patient with leukemia and disseminated MRSA infection unresponsive to conventional treatment. Following drug administration, the patient had a brief episode of flushing, hypotension, and tachycardia, which resolved with diphenhydramine and epinephrine. Although the patient died from complications of chemotherapy, postmortem evaluation revealed only sterile abscesses and no tissues positive for MRSA (12). Although the lysostaphin used for the clinical studies above were described as purified, they were all produced directly from staphylococci and may have contained contaminants, whereas the current material was produced using recombinant technology. However, before the current recombinant lysostaphin can be made available for clinical use, further studies are needed to evaluate its safety and efficacy.
Lysostaphin has been more extensively studied in animals. It has been shown to treat bovine mastitis caused by S. aureus (19), S. aureus endophthalmitis and endocarditis in adult rabbit models (8,20), to eradicate S. aureus colonization in rats (21), and to treat S. aureus infection in adult mice (22). Furthermore, we have previously reported our experiences in treating MSSA infection in a neonatal rat sepsis model, concluding that lysostaphin appears to be as effective as oxacillin and vancomycin in the treatment of this neonatal infection (9).
In this study, we report the use of lysostaphin to treat MRSA infection in a neonatal mouse sepsis model. We found that we can achieve lysostaphin serum levels (2.34–8.92 μg/mL) well above the MIC of ≤0.008 μg/mL we determined for this MRSA strain. A study looking at 17 strains of MRSA found MIC's ranging from 0.007 to 0.125 μg/mL, again well below the serum levels we obtained (8).
Lysostaphin pharmacokinetics have been described in adult mice (13) and neonatal rats (9). Vancomycin pharmacokinetics have been described in adult mice (23,24). To our knowledge, we are the first to describe the pharmacokinetics of lysostaphin and vancomycin in a neonatal mouse model. In comparing the pharmacodynamics of vancomycin and lysostaphin, we found no significant differences between the two drugs. However, the AUC-to-MIC ratio and the Peak-to-MIC trended toward significance, with p values of 0.07 and 0.1, respectively. The pharmacokinetic arm of the experiment was not powered to detect such differences. A larger sample size would likely have allowed us to demonstrate significance. There are some shortcomings in our analysis. A review of the literature did not reveal which, if any, of the pharmacodynamic parameters we calculated are useful in determining lysostaphin efficacy. The fact that lysostaphin is an enzymatic antimicrobial rather than a classic antibiotic may render our evaluation of the parameters we chose, moot. However, our results strongly suggest that favorable, and probably superior, pharmacodynamics can be achieved with lysostaphin when treating MRSA.
In evaluating the survival curves, we found that lysostaphin at either the 10 mg/kg or 15 mg/kg/dose resulted in significantly improved survival compared with control. Furthermore, we observed that lysostaphin at 15 mg/kg/dose had improved efficacy compared with vancomycin. This may be due in part to the likely superior pharmacodynamics of lysostaphin compared with vancomycin. Thus, milligram for milligram, lysostaphin may be more effective against MRSA infection compared with vancomycin.
We chose to evaluate the growth rate of each group for two reasons. First, it could serve as an indirect measure of treatment impact. Secondly, it could be seen as a surrogate for toxicity. Both lysostaphin groups had significantly faster growth rates compared with control, which is consistent with the survival data. However, there was no significant difference between the vancomycin group and lysostaphin group, suggesting that either the magnitude of the difference was too small or this outcome may not be a good measure of efficacy. Because the growth rate comparison could not distinguish between the lysostaphin and vancomycin groups, this may suggest lysostaphin is not more toxic than vancomycin at the doses given or again the magnitude of difference was too small for this sample size.
The results of the quantitative blood cultures confirm and support the survival data. All three treatment groups had lower colony counts compared with control. Furthermore, the lysostaphin 15 mg/kg/dose group trended toward a lower colony count compared with the vancomycin group. In light of the survival curve results, we would have expected to find significantly lower colony counts in the lysostaphin 15 mg/kg/dose group. Because we did not postulate that this outcome measure was not as sensitive as survival, our numbers were too small or there is some additional effect of lysostaphin on the mediators of survival (e.g., cytokine cascade). This hypothesis merits future study. We did not perform bacterial counts on end-organs, but others have reported such information (8,22). Specifically, in an adult rabbit model of MRSA bacterial endocarditis, Climo et al. (8) observed that 5 mg/kg of lysostaphin given three times daily for 3 d resulted in sterile vegetations in 10 of 11 and a mean reduction in vegetation bacterial counts of 8.5 log10 CFU/g, but they did not clear bacteremia. However, animals treated with antibiotics twice daily sterilized no vegetations, reduced mean vegetation bacterial counts by only 4.8 log10 CFU/g, and did not clear bacteremia. In an adult mouse model of MRSA infection, Kokai-Kun et al. (22) observed that 5 mg/kg of lysostaphin given daily for 3 d in 10 mice cleared the kidneys, significantly reduced spleen and liver bacterial counts, and did not provide data on bacteremia. These authors (22) also demonstrated that in the absence of neutrophils lysostaphin appears to clear infection more quickly than in normal mice and speculate that sequestration of MRSA in neutrophils may be responsible for the persistent organ infection.
To summarize, we have shown that at similar doses lysostaphin demonstrates superior efficacy compared with vancomycin in a neonatal mouse sepsis model as demonstrated by improved survival, similar growth rates, and a trend in improved bacteremia. We are the first to report lysostaphin efficacy against MRSA in a neonatal model. If the pattern of increasing neonatal infections with S. aureus, and MRSA in particular holds, we will need new treatment options for this most vulnerable pediatric population. We believe that we have demonstrated that lysostaphin could be one such option.
It has been shown that S. aureus can develop resistance to lysostaphin when exposed to subinhibitory levels (25). However, further studies have shown that MRSA isolates that are exposed to subinhibitory levels of lysostaphin become methicillin-sensitive. This was demonstrated in an adult endocarditis model, where the combination of nafcillin and lysostaphin were shown to be as effective as vancomycin (26). In future studies, we hope to evaluate this combination of drugs in a neonatal model of MSSA and MRSA infection.
As recombinant lysostaphin is a protein of 33 kD, the host has the potential to develop antibodies against it. One study observed that some cattle developed antibody predominantly of the IgG1 subclass, but none with significant anti-lysostaphin titers showed deleterious symptoms upon subsequent infusion and these titers did not affect lysostaphin's in vitro bacteriostatic activity (27). In a study evaluating lysostaphin antibody, lysostaphin treatment of lysyostaphin-immunized rabbits was effective in treating S. aureus infected eyes despite the presence of antibody, and no adverse reactions were observed (20). Finally, a rabbit model of endocarditis, despite the presence of neutralizing antibodies after extended dosing, high levels of serum batericidal activity persisted (8). Although the human neonate's immune response is limited, it has yet to be determined if the human neonate will develop antibody to lysostaphin. But if such antibody develops, it appears it should not be neutralizing (i.e., affect lysostaphin's in vitro activity).
Previous experiments have shown that the CONS species, Staphylococcus epidermidis, was either resistant to lysostaphin or susceptible only at higher concentrations of lysostaphin when compared with S. aureus (28,29). However, when given in combination with a beta-lactam antibiotic, lysostaphin was shown to have a synergistic effect against oxacillin-resistant S. epidermidis (ORSE) in an adult endocarditis model, without development of lysostaphin resistance (30). We are currently investigating whether this holds true in a neonatal ORSE sepsis model.
The increase of MRSA infections in the neonatal intensive care unit and the progressive concern for antibiotic resistance requires development of additional strategies to prevent or treat this infection. Lysostaphin should be one of those considerations. With continued laboratory and clinical development, it is possible that this product could be available for clinical use in neonates in the not too distant future.
Abbreviations
- AUC:
-
area under the curve
- CFU:
-
colony forming unit
- MBC:
-
minimum bactericidal concentration
- MIC:
-
minimum inhibitory concentration
- MRSA:
-
methicillin-resistant Staphylococcus aureus
- MSSA:
-
methicillin-sensitive Staphylococcus aureus
- TSB:
-
tryptic soy broth
References
Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, Lemons JA, Donovan EF, Stark AR, Tyson JE, Oh W, Bauer CR, Korones SB, Shankaran S, Laptook AR, Stevenson DK, Papille L, Poole WK 2002 Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 110: 285–291
Osrin D, Vergnano S, Costello A 2004 Serious bacterial infections in newborn infants in developing countries. Curr Opin Infect Dis 17: 217–224
Healy CM, Hulten KG, Palazzi DL, Campbell JR, Baker CJ 2004 Emergence of new strains of methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit. Clin Infect Dis 39: 1460–1466
Nambiar S, Herwaldt LA, Singh N 2003 Outbreak of invasive disease caused by methicillin-resistant Staphylococcus aureus and prevalence in the neonatal intensive care unit. Pediatr Crit Care Med 4: 220–226
Jones RN 2006 Microbiological features of vancomycin in the 21st Century: minimum inhibitory concentration creep, bactericidal/static activity, and applied breakpoints to predict clinical outcomes or detect resistant strains. Clin Infect Dis 42: S13–S24
Schindler CA, Schuhardt VT 1964 Lysostaphin: a new bacteriolytic agent for the Staphylococcus. Proc Natl Acad Sci USA 51: 414–421
Recsei PA, Gruss AD, Novick RP 1987 Cloning sequence, and expression of the lysostaphin gene from Staphylococcus simulans. Proc Natl Acad Sci USA 84: 1127–1131
Climo MW, Patron RL, Goldstein BP, Archer GL 1998 Lysostaphin treatment of experimental methicillin-resistant Staphylococcus aureus aortic valve endocarditis. Antimicrob Agents Chemother 42: 1355–1360
Oluola O, Kong L, Fein M, Weisman LE 2007 Lysostaphin in treatment of neonatal Staphylococcus aureus infection. Antimicrob Agents Chemother 51: 2198–2200
National Committee for Clinical Laboratory Standards 1997 Methods for Dilution Antimicrobial Susceptibility Test for Bacteria That Grow Anaerobically: Approved Standard M7-A4. 4th ed. Villanova, PA: National Committee for Clinical Laboratory Standards
Saez-Llorens X, McCracken GH Jr 2006 Clinical pharmacology of antibacterial agents. In: Remington JS, Klein JO, Wilson CB, Baker CJ (eds) Infectious Diseases of the Fetus and Newborn Infant. Philadelphia: Elsevier Saunders, pp 1223–1267
Stark FR, Thornsvard C, Flannery EP, Artenstein MS 1974 Systemic lysostaphin in man—apparent antimicrobial activity in a neutropenic patient. N Engl J Med 291: 239–240
Walsh S, Shah A, Mond J 2003 Improved pharmacokinetics and reduced antibody reactivity of lysostaphin conjugated to polyethylene glycol. Antimicrob Agents Chemother 47: 554–558
Ortho-Clinical Diagnostics/VITROS Products, Pub No. J21505_EN, ver 4.0. Rochester, NY: Ortho-Clinical Diagnostics
Hyatt JM, McKinnon PS, Zimmer GS, Schentag JJ 1995 The importance of pharmacokinetic/pharmacodynamic surrogate marks to outcome. Focus on antibacterial agents. Clin Pharmacokinet 28: 143–160
Healy CM, Palazzi DL, Edwards MS, Campbell JR, Baker CJ 2004 Features of invasive Staphylococcal disease in neonates. Pediatrics 114: 953–961
Harris RL, Nunnery AW, Riley HD Jr 1967 Effect of lysostaphin on staphylococcal carriage in infants and children. Antimicrob Agents Chemother 7: 110–112
Quickel KE, Selden R, Caldwell JR, Nora NF, Schaffner W 1971 Efficacy and safety of topical lysostaphin treatment of persistent nasal carriage of Staphylococcus aureus. Appl Microbiol 22: 446–450
Oldham ER, Daley MJ 1991 Lysostaphin: use of a recombinant bactericidal enzyme as a mastitis therapeutic. J Dairy Sci 74: 4175–4182.
Dajcs JJ, Thibodeaux BA, Hume EB, Zheng X, Sloop GD, O'Callaghan RJ 2001 Lysostaphin is effective in treating methicillin-resistant Staphylococcus aureus endophthalmitis in the rabbit. Curr Eye Res 22: 451–457
Kokai-Kun JF, Walsh SM, Chanturiya T, Mond JJ 2003 Lysostaphin cream eradicates Staphylococcus aureus nasal colonization in a cotton rat model. Antimicrob Agents Chemother 47: 1589–1597
Kokai-Kun JF, Chanturiya T, Mond JJ 2007 Lysostaphin as a treatment for systemic Staphylococcus aureus infection in a mouse model. J Antimicrob Chemother 60: 1051–1059
Berthaud N, Montay G, Conard BJ, Desnottes JF 1995 Bactericidal activity and kinetics of RP 59500 in a mouse model of Staphylococcus aureus septicaemia. J Antimicrob Chemother 36: 365–373
Knudsen JD, Fuursted K, Espersen F, Frimodt-Moller N 1997 Activities of vancomycin and teicoplanin and penicillin-resistant pneumococci in vitro and in vivo and correlation to pharmacokinetic parameters in the mouse peritonitis model. Antimicrob Agents Chemother 41: 1910–1915
Zygmunt WA, Tavormina PA 1972 Lysostaphin: model for a specific enzymatic approach to infectious disease. Prog Drug Res 16: 309–333
Climo MW, Ehlert K, Archer GL 2001 Mechanism and suppression of lysostaphin resistance in oxacillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother 45: 1431–1437
Daley MJ, Oldham ER 1992 Lysostaphin: immunogenicity of locally administered recombinant protein used in mastitis therapy. Vet Immunol Immunopathol 31: 301–312
Wu JA, Kusuma C, Mond JJ, Kokai-Kun JF 2003 Lysostaphin disrupts Staphylococcus aureus and Staphylococcus epidermidis biofilms on artificial surfaces. Antimicrob Agents Chemother 47: 3407–3414
Zygmunt WA, Browder HP, Tavormina PA 1968 Susceptibility of coagulase-negative staphylococci to lysostaphin and other antibiotics. Appl Microbiol 16: 1168–1173
Kiri N, Archer G, Climo MW 2002 Combinations of lysostaphin with beta-lactams are synergistic against oxacillin-resistant Staphylococcus epidermidis. Antimicrob Agents Chemother 46: 2017–2020
Acknowledgements
We thank Travis Markham, B.S., and Don Pham, B.S., for their excellent technical assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported in part by Biosynexus Incorporated through an unrestricted research grant. Leonard E. Weisman, M.D. is a consultant to Biosynexus Incorporated, which sponsored a portion of the research in this manuscript. This potential conflict has been reviewed by Baylor College of Medicine and found to be resolved with this disclosure.
Rights and permissions
About this article
Cite this article
Placencia, F., Kong, L. & Weisman, L. Treatment of Methicillin-Resistant Staphylococcus aureus in Neonatal Mice: Lysostaphin Versus Vancomycin. Pediatr Res 65, 420–424 (2009). https://doi.org/10.1203/PDR.0b013e3181994a53
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/PDR.0b013e3181994a53
This article is cited by
-
Evaluation of the clinical relevance of vancomycin for the treatment of Lyme disease
Wiener klinische Wochenschrift (2023)
-
Self-cleaved expression of recombinant lysostaphin from its cellulose binding domain fusion
Applied Microbiology and Biotechnology (2022)
-
Identification and structural characterization of LytU, a unique peptidoglycan endopeptidase from the lysostaphin family
Scientific Reports (2017)
-
Bactericidal synergy of lysostaphin in combination with antimicrobial peptides
European Journal of Clinical Microbiology & Infectious Diseases (2011)
