
Abstract
Low birth weight (LBW) due to intrauterine growth restriction (IUGR) in humans is associated with increased blood pressure (BP) in adulthood. In Western countries, IUGR is based on uteroplacental dysfunction. We used an animal model of uteroplacental dysfunction to evaluate this correlation. We hypothesize that IUGR increases baseline BP and alters the BP response to acute stress, which may explain BP differences in previous studies using stressful methods to obtain BP. IUGR was induced by bilateral uterine artery ligation in pregnant Wistar rats according to a modified method of Wigglesworth. BP was measured in the offspring using telemetry, allowing for unstressed measurements in conscious animals. Cardiovascular data were obtained at the age of 12 wk during baseline and acute olfactory stress induced by an ammonia gauze. Rats born after IUGR had a lower birth weight versus controls and did not completely catch up in weight. At baseline, systolic BP (SBP), mean arterial pressure (MAP), and pulse pressure (PP) were elevated in IUGR rats versus controls, by 8, 6, and 5 mm Hg, respectively. There was a strong negative correlation between birth weight and SBP and between birth weight and PP. During acute stress, there was a tendency to reach a higher peak in SBP and to need a longer period to recover in IUGR animals. We conclude that IUGR is associated with increased baseline BP.
Similar content being viewed by others

Main
IUGR leads to LBW, which is linked to an increased risk of various chronic diseases in adulthood (1–4). Numerous studies have described the association between LBW and hypertension (for review, see Huxley et al. (5)). The pathways that may lead to a rise in BP are not fully understood (6–18).
Several previous authors have studied BP in growth-restricted animals (19). In these studies, BP is commonly measured indirectly using the tail-cuff method. This method entails restraining and preheating the animal, which leads to increased BP, heart rate (HR), and plasma levels of epinephrine and norepinephrine (20). In fact, restraints on laboratory animals have been used as a stressor (21). Results obtained from these studies should therefore be interpreted with caution. The described raised BP in IUGR animals might reflect a different stress response rather than a raised baseline BP.
BP can be measured both directly as in a nonstressed manner by telemetry (20). Previously, only two reports using telemetry have addressed the effect of IUGR on BP in rats. Tonkiss et al. (22) found a small rise in baseline diastolic BP (DBP) but not in SBP in IUGR rats. They also described a marked difference in the response to acute stress with a greater increase in DBP and SBP in IUGR rats. Jansson and Lambert (23) found no evidence for BP elevation after IUGR. In these studies, different models for IUGR were used. For a review of currently applied IUGR models, see Holemans et al. (19). Tonkiss et al. (24) applied an IUGR model based on prenatal protein restriction, which might not be representative of the human situation. In Western countries, the leading cause of IUGR is uteroplacental insufficiency. Therefore, an animal model using reduced uteroplacental blood flow will be the most appropriate model to study the effect of IUGR. Jansson and Lambert (23) used an IUGR model based on unilateral uterine artery ligation.
To evaluate the raised BP in human IUGR, we studied BP by telemetry in an IUGR rat model based on bilateral ligation of the uterine arteries. The pups are classified as IUGR if their birth weight is 2 SD below the mean weight of control pups, which is consistent with the human situation. Age-matched controls are obtained from sham-operated dams.
Second, we were interested in the stress response of IUGR animals. We hypothesized that an altered stress response might be reflected by an augmented rise in cardiovascular parameters during stress and a prolonged period of recovery. Various odors, including predator odor and ammonia, are well-known stressors for the rat and lead to a cortisol release and BP increase (22,25). We used ammonia as a stressor as it is a naturally occurring stressor, being present in rat secretions (26). Furthermore, it is easy to administer and remove.
MATERIALS AND METHODS
Timed pregnant Wistar rats were obtained from Harlan CPB (Horst, The Netherlands). Animals were housed individually in plastic cages with wood chips as bedding in the Clinical Animal Laboratory of the VU University Medical Center. A 12:12-h light-dark cycle was maintained (light on at 06:00 h) in the room, at constant temperature (22 ± 1°C) and relative humidity. Rats had free access to tap water and were fed a standard rodent chow (ssniff R/M-H, Bio Services, Schaijk, The Netherlands). All experiments were in accordance with the approval obtained from the Animal Welfare Committee (DEC) of the VU University Medical Center, Amsterdam.
Experimental groups.
IUGR was induced by bilateral ligation of the uterine arteries on d 17 of gestation according to a modified method of Wigglesworth (27), under general anesthesia using ketamine HCl (75 mg/kg i.p.) and xylazine (5 mg/kg i.p.). Control animals (CTRL) were obtained from sham-operated dams that underwent the same procedure except for the actual ligation. At d 21–22 of gestation, the pups were born. IUGR was defined as a weight on d 2 (day of birth was defined as d 1) below 5.3 g, corresponding to −2 SD of the mean of CTRL pups. Litters were reduced to nine to 10 pups. IUGR and CTRL pups were cross-fostered by a recipient mother that had had the same surgery as the natural mother and was matched for the day of delivery. Animals were weaned at d 28 and housed two per cage. Body weight was measured at regular intervals. Because surgery is known to influence body weight (28), only preimplantation weight data are used.
Telemetry.
At the age of 11 wk, eight IUGR (born from eight different mothers) and eight CTRL (born from four different mothers) males were selected. Animals were ranked according to their body weight, and the highest and lowest ranked animals were excluded. Animals were anesthetized with ketamine HCl (75 mg/kg i.p.) and xylazine (5 mg/kg i.p.), shaved, and cleaned with chlorhexidine. Telemetry transmitters (TA11PA-C40, Data Sciences International, St. Paul, MN; body:transmitter size ratio = 27:1 to 43:1 [28]) were implanted according to standard procedure (29). Briefly, a midline abdominal incision was made, and the aorta was exposed. The catheter of the transmitter was inserted into the abdominal aorta and guided upstream. Tissue adhesive was used to secure the catheter and obtain hemostasis. The transmitter was placed in the abdominal cavity and sutured to the abdominal musculature.
Data acquisition.
Animals were allowed to recover at least 1 wk after surgery. This has been shown to be sufficient (28) and was confirmed in our study group, where body weight returned to the preoperative value within 3 d after surgery. The Dataquest ART 2.1 Silver telemetry system (Data Sciences International) with RPC-1 receivers was used for telemetric measurement of SBP (mm Hg), MAP (mm Hg), DBP (mm Hg), HR (beats/min), and spontaneous locomotor action (SLA) in the animal house. SLA is detected by the system as a change in received signal strength and expressed as counts per minute, with every count representing a movement of the rat of 1.5 to 2 cm.
The Dataquest ART Acquisition software was used to sample all animals during the same period. Baseline sampling was performed every 6 min, setting segment duration at 30 s. In this mode, the average of a 30-s segment is stored as a single value every 6 min. Data were exported from the Dataquest ART Analysis software (Data Sciences International) to Microsoft Excel 2000 (Microsoft Corporation, Seattle, WA). PP (mm Hg) was calculated as the difference between SBP and DBP. If PP fell below 20 mm Hg, the BP measurements were considered to be unreliable, but HR was used unless PP fell below 10 mm Hg. Baseline cardiovascular measurements were obtained from18:00 until 06:00 h to exclude the influence of the presence of people. Data from two consecutive dark periods were averaged and are presented.
Stress test.
When studying the effect of acute stress on BP and HR, continuous sampling (storing one value every 2 s) was performed during the light phase. Sampling started with a reference period of 15–20 min. Following the reference sampling, acute olfactory stress was induced by hanging a 5 × 5-cm gauze with 2 mL ammonia from the wire top of the cage for 5 min. Care was taken to prevent ammonia from touching or dripping on the interior of the cage. The maximum value during stress in HR and SBP was recorded as well as the period to reach this maximum. Values were included only when the value directly before and after the maximum were within a 10% range of the maximum value. Sampling was continued for 45 min to measure recovery from stress. Values from the recovery period were averaged over a 30-s segment. Recovery was defined as a parameter being 100% or less of the reference value during at least two consecutive 30-s segments.
Statistics.
Values are presented as means (± SD) unless stated otherwise. Differences between groups were analyzed with analysis of variance (ANOVA). Correlations between variables were estimated by calculating the Pearson correlation coefficient using SPSS (version 11, SPSS Inc., Chicago, IL) as statistical analysis system. A p < 0.05 was considered to be statistically significant (two tailed).
RESULTS
Figure 1 shows body weight of the IUGR and CTRL rats from birth to the age of 11 wk. By definition, the IUGR rats had a lower birth weight (4.3 ± 0.7 g) than CTRL rats (6.3 ± 0.4 g) (F = 35.1, p < 0.001). IUGR rats showed no complete catch-up growth and had a persistent significantly lower body weight. At the age of 11 wk, body weight was 310 ± 31 g versus 369 ± 15 g in controls (F = 23.0, p < 0.001).

Body weight from d 2 until d 21 (A) and d 21 until d 78 (B) in male IUGR (○; n = 8) and CTRL (•; n = 8) rats. *p < 0.05, **p < 0.01, †p < 0.001.
Baseline BP values are presented in Table 1. BP measurements were not reliable in two IUGR rats because of poor signals and were excluded from all BP analyses. Compared with the CTRL rats, IUGR rats had significantly higher mean SBP, MAP, and PP. Birth weight showed a strong negative correlation with SBP (r = 0.712, p = 0.004) and PP (r = 0.633, p = 0.015) as depicted in Fig. 2. The correlation between birth weight and DBP did not reach significance (r = 0.298, p = 0.30).

Correlation between birth weight and SBP (r = 0.712; p = 0.004) (A), birth weight and DBP (r = 0.298; p = 0.30) (B), and birth weight and PP (r = 0.633; p = 0.015) (C) in 12-wk-old male rats (n = 14).
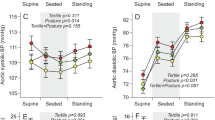
Before the stress test, daytime cardiovascular measurements found similar differences in SBP values (138 versus 130 mm Hg, F = 20.3, p = 0.001, Fig. 3 B) and MAP (121 versus 114 mm Hg, F = 13.0, p = 0.004) but not in PP between IUGR and CTRL rats.

HR (A), SBP (B), and DBP (C) during reference period, acute olfactory stress, and recovery in 12-wk-old male IUGR (○) and CTRL (•) rats.
The cardiovascular stress response is depicted in Figure 3. Acute stress made HR increase gradually and reach a plateau after 5 min (Fig. 3A). SBP and DBP increased instantly to remain at a plateau for the duration of the stress (Fig. 3B and C). During acute stress, SBP did not differ significantly between groups (154 versus 149 mm Hg). Cardiovascular parameters during stress are presented in Table 2.
DISCUSSION
This study shows a difference in cardiovascular parameters between IUGR and CTRL rats at the age of 12 wk under basal conditions in a rat model of IUGR induced by maternal bilateral uterine artery ligation. Also, a tendency to an altered response to acute olfactory stress was noted.
This is the first study to apply telemetric measurement of cardiovascular data in an animal model of IUGR induced by bilateral ligation of the uterine arteries in the pregnant rat. This method is more laborious than others, but closely resembles the human situation of uteroplacental insufficiency, so conclusions derived from this animal model may be more relevant.
Most studies use the indirect and stress-inducing tail-cuff method, which has serious flaws. Stress can be avoided by measuring BP during anesthesia, which allows for a direct intraarterial BP monitoring, but these results may only show the effect of the anesthesia rather than the true changes in BP. Telemetry is the most reliable method for measuring BP in conscious and freely moving animals. However, it is an invasive method and may therefore influence the results. To minimize these influences, transmitters were implanted at a time that the body:transmitter size ratio was in an acceptable range (28). Also, animals were allowed to recover for at least 1 week before measurements started. This has been shown to suffice for rats (28) and was confirmed in our study by the return of body weight to presurgical levels within 3 d after implantation. Furthermore, many factors can induce stress in rodents, like sounds, odors, and activities, which influences measurements (30). In our laboratory, the time when most stimuli can be avoided is during the night, when staff is not present regularly and sounds are reduced to a minimum (M.F. Schreuder, unpublished observations). For these reasons, our data reflect basal BP values. We found a significant correlation between birth weight and baseline SBP. In humans, a higher body weight is associated with a higher BP (31). Huxley et al. (32) suggested that the regression coefficient should not be adjusted for current size since adjustment might produce an association even if birth weight and current BP are uncorrelated. Therefore, only an unadjusted regression is presented which shows a negative correlation.
In this study, PP was increased after IUGR and an inverse relationship between birth weight and PP was found. A rise in PP is primarily due to an increased arterial stiffness and is an independent predictor of cardiovascular disease risk in humans (33). IUGR is linked with a increased large artery stiffness, and a negative correlation with birth weight has been described (34). Future research using the described animal model is necessary to study the underlying factors that determine the altered arterial elasticity.
We noted no significant elevation in DBP and no association between birth weight and DBP. One possible interpretation of these data together with the increase in SBP and PP is that IUGR does not influence BP per se, but programs arterial stiffness only. However, the relatively small number of animals can also explain the absence of significance.
Jansson and Lambert (23) were the first to study the effect of uteroplacental insufficiency on BP using telemetry in a large group of rats and found no association between birth weight and BP after IUGR. Differences in experimental design may account for this. First, different rat strains were used (Wistar versus Sprague-Dawley), which could influence the effect of IUGR on BP since BP does differ between strains (35). Second, the ligation was performed on different days during pregnancy (d 18 versus d 17). The timing of insults during fetal life is known to influence the effects of these insults on BP (36). Third, ligation of the uterine artery may induce hypertension in the mother, which makes the hemodynamic situation in the contralateral unoperated uterine horn different from the hemodynamics in the uterine horns from an unoperated dam (37). Since this can influence BP in the CTRL animals, a difference with IUGR rats can be smaller and therefore more difficult to be found. Using a moderate sound stress (7-mm Hg rise in MAP), Jansson and Lambert found no relation between birth weight and the change in cardiovascular parameters. We used a more severe stressor and found no significant difference in change in BP either, even though there was a tendency to an altered stress response.
During baseline conditions, we found an increase of 8 mm Hg in SBP. Most studies using the tail-cuff method have found a much higher difference in BP between controls and IUGR animals (38,39). These data are more in line with the increase of 15 mm Hg that we found during acute stress. In our opinion, this underlines the known stressed effect of the tail-cuff method. The time to reach maximum values of HR and SBP, and the time to return to reference values were not significantly different between groups. However, we hypothesize that the trend seen in 12-wk-old rats is indicative of an altered stress response after IUGR. More information on cardiovascular data later in life is needed, both under basal as well as stressed conditions.
Some studies have described a difference in BP between sexes in various models of hypertension. After IUGR, BP is affected more in male than female rats (40). As Jansson and Lambert (23) found no difference in BP after IUGR, we selected male rats as they are more likely than females to show a difference in BP.
A negative association between birth weight and BP has been confirmed in several different animal species, including the guinea pig (41), pig (42), and sheep (43). As these associations are present in several animal models after only a short period of IUGR, BP should be checked in children after IUGR to prevent secondary damage due to a raised BP. A possible explanation for the association between LBW and a higher BP is a reduction in the number of nephrons, which has been shown after IUGR (6–12,44) and may be due to an increased renal apoptosis (13). To compensate for the reduced filtration surface, hypertrophy and hyperfiltration occur, leading to raised glomerular blood pressure and SBP and finally proteinuria and end-stage renal disease (14–17). A relationship between low nephron number and raised BP has been confirmed in patients with “essential” hypertension: compared with individuals with normal BP, patients with hypertension had less glomeruli at autopsy (18).
In conclusion, telemetric assessment of cardiovascular parameters revealed an increase in SBP, MAP, and PP under baseline conditions in 12-wk-old male rats after IUGR. We showed a strong and significant negative relationship between birth weight and SBP and between birth weight and PP.
Abbreviations
- BP:
-
blood pressure
- CTRL:
-
control
- DBP:
-
diastolic blood pressure
- HR:
-
heart rate
- IUGR:
-
intrauterine growth restriction
- LBW:
-
low birth weight
- MAP:
-
mean arterial pressure
- PP:
-
pulse pressure
- SBP:
-
systolic blood pressure
- SLA:
-
spontaneous locomotor action
References
Hales CN, Barker DJ, Clark PM, Cox LJ, Fall C, Osmond C, Winter PD 1991 Fetal and infant growth and impaired glucose tolerance at age 64. BMJ 303: 1019–1022
Barker DJ 1995 Fetal origins of coronary heart disease. BMJ 311: 171–174
Godfrey KM, Barker DJ 2000 Fetal nutrition and adult disease. Am J Clin Nutr 71: 1344S–1352S
Barker DJ 2001 The malnourished baby and infant. Br Med Bull 60: 69–88
Huxley RR, Shiell AW, Law CM 2000 The role of size at birth and postnatal catch-up growth in determining systolic blood pressure: a systematic review of the literature. J Hypertens 18: 815–831
Beech DJ, Sibbons PD, Howard CV, van Velzen D 2000 Renal developmental delay expressed by reduced glomerular number and its association with growth retardation in victims of sudden infant death syndrome and in "normal" infants. Pediatr Dev Pathol 3: 450–454
Hinchliffe SA, Lynch MR, Sargent PH, Howard CV, van Velzen D 1992 The effect of intrauterine growth retardation on the development of renal nephrons. Br J Obstet Gynaecol 99: 296–301
Merlet-Benichou C, Gilbert T, Vilar J, Moreau E, Freund N, Lelievre-Pegorier M 1999 Nephron number: variability is the rule. Causes and consequences. Lab Invest 79: 515–527
Zidar N, Cor A, Premru Srsen T, Stajer D 1998 Is there an association between glomerular density and birth weight in healthy humans. Nephron 80: 97–98
Manalich R, Reyes L, Herrera M, Melendi C, Fundora I 2000 Relationship between weight at birth and the number and size of renal glomeruli in humans: a histomorphometric study. Kidney Int 58: 770–773
Merlet-Benichou C, Vilar J, Lelievre-Pegorier M, Moreau E, Gilbert T 1997 Fetal nephron mass: its control and deficit. Adv Nephrol Necker Hosp 26: 19–45
Hughson M, Farris AB 3rd, Douglas-Denton R, Hoy WE, Bertram JF 2003 Glomerular number and size in autopsy kidneys: the relationship to birth weight. Kidney Int 63: 2113–2122
Pham TD, MacLennan NK, Chiu CT, Laksana GS, Hsu JL, Lane RH 2003 Uteroplacental insufficiency increases apoptosis and alters p53 gene methylation in the full-term IUGR rat kidney. Am J Physiol Regul Integr Comp Physiol 285: R962–R970
Hostetter TH, Olson JL, Rennke HG, Venkatachalam MA, Brenner BM 1981 Hyperfiltration in remnant nephrons: a potentially adverse response to renal ablation. Am J Physiol 241: F85–F93
Brenner BM, Lawler EV, Mackenzie HS 1996 The hyperfiltration theory: a paradigm shift in nephrology. Kidney Int 49: 1774–1777
Garrett PJ, Bass PS, Sandeman DD 1994 Barker, Brenner, and babies–early environment and renal disease in adulthood. J Pathol 173: 299–300
Brenner BM, Garcia DL, Anderson S 1988 Glomeruli and blood pressure. Less of one, more the other?. Am J Hypertens 1: 335–347
Keller G, Zimmer G, Mall G, Ritz E, Amann K 2003 Nephron number in patients with primary hypertension. N Engl J Med 348: 101–108
Holemans K, Aerts L, Van Assche FA 2003 Fetal growth restriction and consequences for the offspring in animal models. J Soc Gynecol Invest 10: 392–399
Kramer K, Kinter LB 2003 Evaluation and applications of radiotelemetry in small laboratory animals. Physiol Genomics 13: 197–205
Cherney A, Edgell H, Krukoff TL 2003 NO mediates effects of estrogen on central regulation of blood pressure in restrained, ovariectomized rats. Am J Physiol Regul Integr Comp Physiol 285: R842–R849
Tonkiss J, Trzcinska M, Galler JR, Ruiz-Opazo N, Herrera VL 1998 Prenatal malnutrition-induced changes in blood pressure: dissociation of stress and nonstress responses using radiotelemetry. Hypertension 32: 108–114
Jansson T, Lambert GW 1999 Effect of intrauterine growth restriction on blood pressure, glucose tolerance and sympathetic nervous system activity in the rat at 3-4 months of age. J Hypertens 17: 1239–1248
Henriksen T, Clausen T 2002 The fetal origins hypothesis: placental insufficiency and inheritance versus maternal malnutrition in well-nourished populations. Acta Obstet Gynecol Scand 81: 112–114
Campbell T, Lin S, DeVries C, Lambert K 2003 Coping strategies in male and female rats exposed to multiple stressors. Physiol Behav 78: 495–504
Pan TM, Shimoda K, Cai Y, Kiuchi Y, Nakama K, Akimoto T, Nagashima Y, Kai M, Ohira M, Saegusa J, et al. 1995 Deodorization of laboratory animal facilities by ozone. Exp Anim 44: 255–259
Wigglesworth JS 1964 Experimental growth retardation in the foetal rat. J Pathol Bacteriol 88: 1–13
Leon LR, Walker LD, DuBose DA, Stephenson LA 2004 Biotelemetry transmitter implantation in rodents: impact on growth and circadian rhythms. Am J Physiol Regul Integr Comp Physiol 286: R967–R974
Brockway BP, Mills PA, Azar SH 1991 A new method for continuous chronic measurement and recording of blood pressure, heart rate and activity in the rat via radio-telemetry. Clin Exp Hypertens A 13: 885–895
Milligan SR, Sales GD, Khirnykh K 1993 Sound levels in rooms housing laboratory animals: an uncontrolled daily variable. Physiol Behav 53: 1067–1076
Davy KP, Hall JE 2004 Obesity and hypertension: two epidemics or one?. Am J Physiol Regul Integr Comp Physiol 286: R803–R813
Huxley R, Neil A, Collins R 2002 Unravelling the fetal origins hypothesis: is there really an inverse association between birthweight and subsequent blood pressure?. Lancet 360: 659–665
Franklin SS, Khan SA, Wong ND, Larson MG, Levy D 1999 Is pulse pressure useful in predicting risk for coronary heart Disease? The Framingham heart study. Circulation 100: 354–360
Cheung YF, Wong KY, Lam BC, Tsoi NS 2004 Relation of arterial stiffness with gestational age and birth weight. Arch Dis Child 89: 217–221
Lemmer B, Mattes A, Bohm M, Ganten D 1993 Circadian blood pressure variation in transgenic hypertensive rats. Hypertension 22: 97–101
Ortiz LA, Quan A, Weinberg A, Baum M 2001 Effect of prenatal dexamethasone on rat renal development. Kidney Int 59: 1663–1669
Podjarny E, Baylis C, Losonczy G 1999 Animal models of preeclampsia. Semin Perinatol 23: 2–13
Langley-Evans SC, Welham SJ, Jackson AA 1999 Fetal exposure to a maternal low protein diet impairs nephrogenesis and promotes hypertension in the rat. Life Sci 64: 965–974
Woodall SM, Johnston BM, Breier BH, Gluckman PD 1996 Chronic maternal undernutrition in the rat leads to delayed postnatal growth and elevated blood pressure of offspring. Pediatr Res 40: 438–443
Kwong WY, Wild AE, Roberts P, Willis AC, Fleming TP 2000 Maternal undernutrition during the preimplantation period of rat development causes blastocyst abnormalities and programming of postnatal hypertension. Development 127: 4195–4202
Persson E, Jansson T 1992 Low birth weight is associated with elevated adult blood pressure in the chronically catheterized guinea-pig. Acta Physiol Scand 145: 195–196
Poore KR, Forhead AJ, Gardner DS, Giussani DA, Fowden AL 2002 The effects of birth weight on basal cardiovascular function in pigs at 3 months of age. J Physiol 539: 969–978
Dodic M, Abouantoun T, O'Connor A, Wintour EM, Moritz KM 2002 Programming effects of short prenatal exposure to dexamethasone in sheep. Hypertension 40: 729–734
Schreuder MF, Nyengaard JR, Fodor M, Van Wijk JA, Delemarre-van de Waal HA 2005 Glomerular number and function are influenced by spontaneous and induced low birth weight in rats. J Am Soc Nephrol 16: 2913–2919
Acknowledgements
We would like to thank dr. K. Kramer for his expert advise on the telemetry system and Michiel Oosterveld for his helpful suggestions.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schreuder, M., Fodor, M., van Wijk, J. et al. Association of Birth Weight with Cardiovascular Parameters in Adult Rats During Baseline and Stressed Conditions. Pediatr Res 59, 126–130 (2006). https://doi.org/10.1203/01.pdr.0000190576.08501.df
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.pdr.0000190576.08501.df
This article is cited by
-
Echocardiographic assessment of fetal cardiac function in the uterine artery ligation rat model of IUGR
Pediatric Research (2021)
-
Bone growth and sexual dimorphism at birth in intrauterine-growth-retarded rats
Anatomical Science International (2011)
