
Abstract
Rice gruels have been used as home remedies to treat dehydration associated with diarrheal illness in developing countries. These preparations have produced conflicting results, most likely due to the heterogeneity of starch used. We investigated whether the modified tapioca starch, Textra™ (TX), at 5.0 or 10.0 g/L added to a 90 mmol/L Na+-111 mmol glucose oral rehydration solution (ORS) enhanced water and electrolyte absorption in two models of diarrhea. To induce a secretory state (model A), the jejunum of juvenile rats was perfused with 10 mmol/L theophylline (THEO) under anesthesia and then perfused with the solutions indicated above. To produce chronic osmotic-secretory diarrhea (model B), rats had a magnesium citrate-phenolphthalein solution as the sole fluid source for 1 wk, and then were perfused as the THEO-treated rats. Water, electrolyte, and glucose absorption were measured during both perfusions. As an extension of the perfusion studies, we compared how fast rats recovered from chronic osmotic diarrhea by offering them either water, ORS, or ORS containing 5.0 g/L TX along with solid food. Recovery rate markers were measured after 24 h and included weight gain, food and fluid intake, and stool output. In model A, addition of 5.0 g/L TX to ORS reversed Na+ secretion and improved net water as well as K+ and glucose absorption, compared with THEO-treated rats perfused with ORS without TX. In model B, addition of TX to ORS increased water, Na+, K+, and glucose absorption, compared with rats perfused without TX. Increasing TX from 5.0 to 10.0 g/L had no additional benefit. In recovery experiments, animals with free access to ORS with TX had significantly greater weight gain and decreased stool output compared with animals recovering with water or ORS without TX. Our experiments suggest that TX may be a useful additive to standard ORS to promote fluid and electrolyte absorption and may provide additional energy without increasing ORS osmotic load.
Similar content being viewed by others


Main
The WHO has promoted the use of ORS as the first line of defense against diarrheal illness regardless of etiology(1). Neither the currently recommended formula WHO-ORS nor its variants shorten disease duration or decrease stool losses, despite their effectiveness in compensating for dehydration and redressing electrolyte imbalance(1,2). Numerous studies have been devoted to investigating ORS additives that might further increase water and electrolyte absorption(3). These studies have included clinical trials investigating the efficacy of ORS containing amino acids such as glutamine, maltodextrins, and other glucose polymers. However, these studies have generally produced limited results(4–7). Therefore, research efforts continue for the development of an ORS capable of enhancing water and electrolyte absorption with the ultimate hope of shortening disease duration and reducing mortality, especially in infants and children(2,8).
Home remedies for diarrheal illness, such as rice extracts and gruels, have been universally used in an attempt to increase water electrolyte absorption in children with diarrhea(9,10). The addition of rice and starch-rich cereal grains to ORS has received attention as a method of both rehydration and provision of greater energy than the standard WHO-ORS because these products have been shown to be proabsorptive without increasing the osmotic load. An additional benefit is that infants and children can tolerate and digest starch products with little difficulty(10–13). Previous studies from our laboratory indicate that other additives can accelerate water and solute availability from ORS, such as the poorly absorbed soluble fibers gum arabic and carboxymethylcellulose(14–16). In this study, we investigated whether a digestible modified tapioca starch, TX, when added to a standard ORS, could enhance absorption during acute jejunal perfusions in two models of diarrheal disease. In one, an acute secretory status was induced via a jejunal perfusion of THEO, a methylxanthine capable of increasing cAMP and cGMP levels, promoting water and electrolyte secretion(17–19). The second approach was a model of chronic diarrhea induced in rats by a Mg Cit solution provided as their sole source of fluid for 7 d. In addition to jejunal perfusions assessing the effects of TX on improving water and electrolyte absorption, we also investigated whether a TX-based ORS could accelerate the recovery of animals with chronic osmotic diarrhea.
METHODS
Animals. All animals used in this study were male Sprague-Dawley rats (Harlan-Sprague-Dawley, Indianapolis, IN) weighing 60-80 g with free access to food (Purina Lab Chow; Ralston Purina Co., St. Louis, MO) and water. They were acclimated for a minimum of 48 h in polycarbonate cages at 72°F with a 12-h light-dark cycle before dietary treatment or intestinal perfusion as described below. Food was withheld from the rats before laparotomy unless otherwise indicated.
Solutions used and experimental protocol. The basal WHO-ORS contained 60 mmol/L Na chloride and 10 mmol/L trisodium citrate for a final Na concentration of 90 mmol/L, 20 mmol/L K chloride, and 111 mmol/L glucose. The osmolality of each solution was 300 ± 4 mOsm/kg (Wescor vapor pressure osmometer, model 5500, Logan, UT). The modified tapioca starch, TX, was added to or omitted from the ORS at 5.0 or 10.0 g/L with gentle heating. Addition of TX did not contribute free glucose to the solutions, and there was no difference in osmolality between the preparations containing TX and those not containing TX. In addition, heating the solutions to facilitate TX dissolution did not affect the osmolality or viscosity of either ORS containing TX. TX was a gift from the National Food Starch and Chemical Company (Bridgewater, NJ). Viscosity of the solution was determined with a Brookfield viscometer (model DV-I; Brookfield Engineering Labs, Stoughton, MA). The relative viscosity (η) of each solution containing 0, 0.5, and 10.0 g/L TX was 1.00, 1.25, and 1.60, respectively. Chemicals for the ORS were purchased from Sigma Chemical Co. (St. Louis, MO). Tritiated water (3H2O, 2 µCi/L = 74 kBq/L; DuPont-New England Nuclear, Boston, MA) was added to all experimental solutions to monitor lumen-to-serosa water flux.
Anesthesia was induced with ketamine/xylazine (87/13 g/L, at a dose of 0.15 mL/100 g, intramuscularly). After induction, a midline incision was made, the jejunum was cannulated with polyethylene tubing at the ligament of Treitz, and an exit port was inserted 20-30 cm distally. Twelve rats were used in each perfusion and three solutions were perfused in each experiment to decrease interexperimental variability, although only one solution was perfused in each rat.
Solutions were heated in a water bath to reach body temperature (37°C) as they entered the rat intestine and were perfused with a peristaltic pump (model 1203; Harvard Instruments, Boston, MA) at a rate of 10-12 mL/h. The actual flow rate of each line was determined by collecting 30-min effluents pre- and postperfusion. The experimental protocol consisted of a 1-h equilibration to stabilize ion gradients, followed by 6-15 min collections. The weight differences between fluid entering and leaving the intestinal segment in each collected fraction were used to calculate net H2O absorption. Jin was measured by the disappearance of 3H2O from the perfusate. Jeff was determined by the difference between Jin and net H2O absorption. In addition, values of Jin/Jeff were calculated for each rat. Electrolyte and glucose absorption rates, as well as the algorithms used in the calculation of absorption rates and unidirectional water fluxes, have been published(16). This study was approved by the Institutional Animal Care Committee.
Secretory diarrhea model. Rats were fasted overnight, and anesthetized, and the jejunum was perfused with the WHO-ORS containing 10 mmol/L THEO, to which TX was added at concentrations of 0, 5.0, or 10.0 g/L. Weights of the control and THEO-treated rats, perfused with or without TX, did not significantly differ [control: 107.0 ± 3.2 g (n = 8); THEO: 104.0 ± 4.3 g (n = 30)]. Controls were perfused with the WHO-ORS without THEO.
Chronic osmotic diarrhea model. Juvenile rats (60-80 g) had free access to solid food for 1 wk and were offered as their only source of fluid a cathartic solution containing magnesium citrate USP diluted with an equal volume of tap water to a final magnesium concentration of 4.8 g/L with the addition of 0.1 g/L phenolphthalein. Control animals were fed the same solid diet and tap water. After 1 wk, rats were anesthetized and the jejunum was perfused, as described above. To compare transport in animals with the same final weight, initial weights of rats receiving the cathartic solution were selected such that their initial weight before Mg Cit treatment was greater than that of the controls [Mg Cit: 72.6 ± 5.2 g (n = 22); controls: 61.0 ± 3.7 g (n = 11)]. This was done because in previous experiments, rats ingesting the cathartic solution failed to grow as well as controls(16). At the end of the treatment period, immediately before perfusion, rat weights were indistinguishable [Mg Cit: 114.0 ± 6.7 g (n = 22); controls = 108.0 ± 7.3 g (n = 11)].
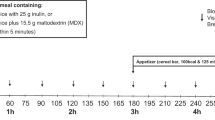
Recovery experiments. Osmotic secretory diarrhea was induced in juvenile rats as reported above. After the 7-d treatment with the cathartic solution, animals were divided into four treatment groups offive to six animal each. Each animal was individually housed in acid-washed steel metabolic cages during the recovery trial. Rats in group 1 (no recovery) were not placed on a recovery trial and was continued on Mg Cit for an additional 24 h. Group 2 (water recovery) received water, group 3 received the WHO-ORS (ORS recovery), and group 4 received the same WHO-ORS supplemented with 0.5 g/L TX (TX recovery). Fluid intake, food consumption, animal weights, and stool weights were monitored after 24 h of rehydration therapy. A flow chart outlining the experimental protocol for both the recovery and perfusion experiments can be found in Figure 1.

Experimental protocol of perfusion and metabolic studies. Animals were acclimatized for 48 h and then either fasted overnight and perfused with 90 mmol/L Na+-111 mmol/L glucose ORS in the presence or absence of 10 mM THEO containing 0, 5.0, or 10.0 g/L TX or placed on Mg Cit for 7 d to induce diarrhea. Those rats drinking Mg Cit were either perfused with the ORS containing 0, 5.0, or 10.0 g/L TX or placed on a recovery trial in which each group of rats received either Mg Cit (no recovery), water, ORS, or ORS + 5.0 g/L TX for 24 h, after which metabolic parameters were measured (see "Methods").
Statistics. Data were analyzed with a one-way analysis of variance with a post hoc Tukey's test for critical differences(20). Significance was set at the 95% level (p < 0.05). All data are expressed as means ± SEM.
RESULTS
Acute Jejunal Secretory Model
General characteristics. The jejunal perfusion of 10 mM THEO, as reported here and previously published, results in secretion of Na into the lumen and reduced water and K absorption(16).
Water, electrolyte, and glucose absorption. Net water, electrolyte, and glucose absorption were impaired by perfusion with THEO-containing ORS. The fluid and solute absorption effects described above were reversed by the addition of TX (Fig. 2 and Table 1). TX (5.0 g/L) added to ORS enhanced net water absorption by increasing Jin compared with THEO-treated rats without TX and untreated controls (Table 1). TX (10 g/L) added to ORS maintained the proabsorptive effects seen at 5.0 g/L; however, no additional benefit was apparent. TX (5.0 and 10.0 g/L) normalized Na absorption and enhanced K and glucose absorption above THEO-perfused and control values (Fig. 2). TX (10 g/L), although maintaining electrolyte absorption seen at 5.0 g/L, did not provide any additional benefit. Rats treated with THEO without TX had a reduced water Jin/Jeff compared with untreated controls (Table 1). This reduction in Jin/Jeff was reversed by the addition of TX to ORS to values indistinguishable from controls.

Intestinal absorption rates of sodium, potassium, and glucose in THEO-treated rats. Data are means ± SEM. Controls, n = 8 (□); THEO + 0 g/L TX, n = 13 (▪); THEO + 5.0 g/L TX, n = 12 (□); THEO + 10.0 g/L TX, n = 13 (□). Values that do not share a common letter are significantly different (p < 0.05). The control group was perfused with 90 mmol/L Na+-111 mmol/L glucose ORS. The other groups were perfused with the same ORS containing 10 mmol/L THEO with or without the modified tapioca starch, TX.
Chronic Osmotic Diarrhea Model
General characteristics. Rats drinking the Mg Cit solution for 7 d presented with loose stools, failed to grow as well as controls, and had fluid-filled ceca at laparotomy. Quantitative physical and biochemical characteristics of this model have been published(16,19).
Water, electrolyte, and glucose absorption. Rats drinking the cathartic solution did not show a decrease in net jejunal water absorption, Jin, or Jeff (Fig. 3, and Table 2); however, the addition of TX at 5.0 or 10.0 g/L increased net water absorption, attributable to a greater Jin than the Mg Cit-treated rats and control rats. Na transport was unchanged by the cathartic solution treatment compared with controls but was enhanced by the addition of TX (5.0 or 10.0 g/L) to the ORS (Fig. 3). Net K absorption was sharply reduced in the Mg Cit rats compared with controls, but the addition of TX to ORS (5.0 and 10.0 g/L) restored the absorption of this ion to normal levels. Although the cathartic treatment did not alter glucose transport, TX at 5.0 g/L increased glucose absorption compared with rats with diarrhea not perfused with TX and controls. Raising the TX concentration from 5.0 to 10.0 g/L maintained, but did not improve, ORS efficacy.

Intestinal absorption rates of sodium, potassium, and glucose in rats with Mg Cit-induced chronic osmotic diarrhea. Data are means ± SEM. Controls, n = 8 (□); Mg Cit + 0 g/L TX, n = 13 (squlf]); Mg Cit + 5.0 g/L TX, n = 12 (□); Mg Cit + 10.0 g/L TX, n = 11 (□). Values that do not share a common letter are significantly different (p < 0.05). The control group was perfused with 90 mmol/L Na+-111 mmol/L glucose ORS. The other groups were offered Mg Cit for 7 d and perfused with the same ORS containing either 0, 5.0, or 10.0 g/L TX.
Recovery Trials
Animals with Mg Cit-induced diarrhea not placed on a recovery trial presented with virtually no weight gain over 24 h despite eating and drinking similar amounts compared with other groups (Table 3). The rats receiving water or ORS as recovery solutions gained significantly more weight than those animals not placed on a recovery solution. However, rats receiving the TX containing ORS (5.0 g/L) had a greater weight gain compared with all other groups. The TX recovery group ate significantly greater amounts of solid food compared with all other groups. However, fluid intake, which we believe is an indicator of overall improvement in physiologic and nutritional status of the animals on the TX recovery regimen, did not differ among treatments. Stool output of animals not recovering from diarrhea, as well as those in the water and ORS groups, was indistinguishable after 24 h. By contrast, rats offered the TX containing ORS had a lower stool output compared with all other groups.
DISCUSSION
This study extends our earlier work on the proabsorptive properties of TX in WHO-ORS to two animal models of diarrhea(21). Earlier findings showed that 5.0 g/L TX added to WHO-ORS stimulated small intestinal water and Na+ absorption in normal rats, compared with ORS without the additive(21). In this report, we show that the addition of TX enhanced Na, K, and glucose absorption during jejunal perfusions in the acute model of secretory diarrhea induced by THEO, as well as in the model of chronic diarrheal disease produced by administration of the Mg Cit solution. The physiologic transport effects produced by the addition of TX are paralleled by morphologic evidence of expansion of the villus extracellular spaces, a structural feature associated with enhanced lumen-to-serosa flow of water and electrolytes (data not shown)(22). Similar results were also seen in the intact animals who received TX during recovery from osmotic diarrhea. These animals showed a decrease in stool output and an increase in weight gain during recovery compared with other groups. These are precisely the goals sought after to improve the efficacy of ORS.
The THEO model is used to emulate certain aspects of the secretion induced by the toxins of Vibrio cholerae and some strains of Escherichia coli. These toxins, like THEO, elevate mucosal epithelial cyclic nucleotides, leading to the stimulation of crypt chloride secretion, the former by increasing guanylyl cyclase activity and the latter by phosphodiesterase inhibition resulting in increased cAMP(17,18,23,24). The experimental model of chronic osmotic diarrhea used in this study, induced by the administration of a Mg Cit solution, intends to reproduce some aspects of chronic osmotic diarrhea in infants associated with repeated cow's milk feedings and recurrent gastrointestinal infections linked to lactase deficiency and lactose intolerance. Poorly absorbed lactose increases the osmotic load in the gut resulting in persistent diarrhea(13). Rats drinking the Mg Cit solution present with marked fluid accumulation in the cecum and decreased rate of growth, paralleling common characteristics seen in recurrent clinical diarrheal episodes in infants and children. The mechanisms of phenolphthalein-induced catharsis involves the inhibition of (Na/K)-ATPase in the basolateral membrane of the enterocyte(25), either directly or through the stimulation of the inducible or constitutive form of nitric oxide synthase, resulting in increases in cGMP and subsequent smooth muscle relaxation and intestinal secretion(26). Although neither the acute nor chronic forms of experimental diarrhea are ideal models because the mode of inducing fluid and electrolyte loss differ from that triggering diarrhea in humans, they permit systematic studies on formula modifications or the utilization of additives to ORS(16,19).
The basis for the addition of TX to ORS stems from the considerable interest in the use of rice or other cereal derivatives as components of ORS to shorten the illness and ameliorate electrolyte loss during diarrheal episodes(27–29). Although preliminary studies appeared promising, the lack of standardization of the additives and the complexity of the differing products, including starchy gruels and amylase-treated starch, have produced largely inconclusive results(4). We reasoned that a standardized product that shares some chemical characteristics of partially hydrolyzed starch should yield positive proabsorptive effects comparable with those seen in the field with homemade heterogeneous solutions, thus facilitating analysis and interpretation of results. TX can remain in suspension without increasing viscosity, whereas non-modified types of starch tend to precipitate upon standing, which may confound their effectiveness in the ORS or make their evaluation inaccurate.
ORS with a greater energy content than that provided by glucose, without an osmotic penalty, has an added potential benefit for infants with diarrhea. Malnourished infants with chronic diarrhea commonly present with deficiencies in α-amylase, maltase, and isomaltase, which impairs or abolishes the digestion of complex carbohydrates provided by solid foods(30). Only salivary glucoamylase remains unaffected by gastroenteritis. This enzyme can hydrolyze starch into free glucose(31); therefore, modified starch products added to currently used ORS offer a readily useable energy source for infants with diarrhea. Although a TX-enriched ORS could not substitute for the timely introduction of regular feedings, it could serve as a bridge during recovery from gastroenteritis.
Although the mechanism(s) by which TX stimulates increased water and electrolyte absorption from ORS remains undetermined, we can offer several hypotheses to explain its proabsorptive effects. These include 1) TX-induced release of the proabsorptive gut hormone PYY or 2) induction of apical GLUT1 in the small intestine by TX. Recent studies have shown that colonic perfusions of fibers and gums such as pectin or gum arabic were secretagogues of PYY, a peptide known to stimulate water and electrolyte absorption in the intestine(32,33). Similarly, a glucose polymer such as TX, which resembles gum arabic chemically may stimulate the release of PYY, thus stimulating intestinal absorption.
Alternatively, TX may enhance electrolyte absorption through the activation of the GLUT1 transporter. This could occur by the recruitment of GLUT1 transporters from prestored intracellular sites to the apical plasma membrane or induction of GLUT1 mRNA synthesis, because it has been shown that the GLUT1 transporter can be up-regulated by feedings of a carbohydrate-rich diet(34–37). This potential mechanism, however, may be more significant in the recovery trials presented in this study rather than in acute perfusion studies. This mechanism along with the release of gut trophic factors(38) might improve intestinal morphology and function, and thereby play a positive role in the shortening of disease duration(39,40). Further research is required to evaluate the specific mechanisms underlying the improvement in transport function produced by the addition of TX to ORS and other long-chain polysaccharides to ORS. These studies could provide the physiologic and biochemical basis for the formulation of more effective ORS.
Abbreviations
- GLUT1 :
-
Na-coupled glucose transporter
- J in :
-
mucosa-to-serasa water influx
- J eff :
-
serosa-to-mucosa water efflux
- J in /J eff :
-
H2O influx/efflux ratio
- Mg Cit :
-
Magnesium citrate-phenolphthalein
- ORS :
-
oral rehydration solution
- PYY :
-
peptide YY
- THEO :
-
theophylline
- TX :
-
Textra™
- USP :
-
United States Pharmacopeia
- WHO :
-
World Health Organization
References
Ballisteri WF 1990 Oral rehydration in acute infantile diarrhea. Am J Med 88: 30S–33S.
Avery ME, Synder JD 1990 Oral therapy for acute diarrhea: the underused solution. N Engl J Med 323: 891–894.
Patra FC, Mahalanabis D, Jalan KN, Sen A, Banerjee P 1984 In search of a super solution: controlled trial of glycine-glucose ORS in infantile diarrhoea. Acta Paediatr Scand 73: 18–21.
Bhan MK, Mahalanabis D, Fontaine O, Pierce NF 1994 Clinical trials of improved oral rehydration salt formulation: a review. Bull World Health Organ 72: 945–955.
Lebenthal E, Lu RB 1991 Glucose polymers as an alternative to glucose in oral rehydration solutions. J Pediatr 118: 562–569.
Fayad IM, Hashem M, Duggan C, Refat M, Bakir M, Fontaine O, Santosham M 1993 Comparative efficacy of rice-based ORS plus early feeding versus glucose based ORS plus early feeding. Lancet 342: 772–775.
Santos Ocampo PD, Bravo LC, Rogacion JM, Battad GR 1993 A randomized double-blind clinical trial of a maltodextrin containing oral rehydration solution in acute infantile diarrhea. J Pediatr Gastroenterol Nutr 16: 23–28.
Farthing MJG 1988 History and rationale of oral rehydration and recent developments in the formulation of an optimum solution. Drugs 36: 80–90.
Molla AM, Molla A, Nath SK, Khatun M 1989 Food based oral rehydration salt solution for acute childhood diarrhoea. Lancet 2: 429–431.
Patra FC, Mahalanabis D, Jalan NK 1982 Is oral rice electrolyte solution superior to glucose electrolyte solution in infantile diarrhea?. Arch Dis Child 57: 910–912.
Kenya PR, Odongo HW, Oundo G, Waswa K, Mattunga J, Molla AM, Nath SK, Molla A, Greenough WB III, Juma R, Were BN 1989 Cereal based ORS. Arch Dis Child 64: 1032–1035.
Santosham M, Fayad IM, Hashem M, Goepp JG, Refat M, Sach BB 1990 A comparison of rice based ORS and "early feeding" for treatment of acute diarrhea in infants. J Pediatr 116: 868–875.
Lifshitz F 1981 Acquired carbohydrate intolerance in children. In: Paige DM, Bayless TM (eds) Lactose Digestion: Clinical and Nutritional Implications. Johns Hopkins University Press, Baltimore, 182–193.
Wapnir RA, Teichberg S, Go JT, Wingertzahn MA, Harper RG 1996 Oral rehydration solution: enhanced sodium absorption with gum arabic. J Am Coll Nutr 15: 377–382.
Wapnir RA, Wingertzahn MA, Teichberg S 1997 Cellulose derivatives and intestinal absorption of water and electrolytes: potential role in oral rehydration solutions. Proc Soc Exp Biol Med 215: 275–280.
Wapnir RA, Wingertzahn MA, Moyse J, Teichberg S 1997 Gum arabic promotes rat jejunal sodium and water absorption from oral rehydration solutions in two models of diarrhea. Gastroenterology 112: 1979–1985.
Field M, Plotkin GR, Silen W 1968 Effects of vasopressin, theophylline and cyclic adenosine monophosphate on short-circuit current across isolated rabbit ileal mucosa. Nature 217: 469–471.
Powell PW, Farris RK, Carbonetto ST 1974 Theophylline, cyclic AMP, choleragen, and electrolyte transport by rabbit ileum. Am J Physiol 227: 1428–1435.
Wapnir RA, Zdanowicz MM, Teichberg S, Lifshitz F 1988 Oral hydration solutions in experimental osmotic diarrhea: enhancement by alanine and other amino acids and oligopeptides. Am J Clin Nutr 48: 84–90.
Zar JH 1984 Biostatistical Analysis, 2nd Ed. Prentice-Hall, Englewood Cliffs, NJ, 162–183.
Wapnir RA, Wingertzahn MA, Moyse J, Teichberg S 1998 Proabsorptive effects of modified tapioca starch as an additive of oral rehydration solutions. J Pediatr Gastroenterol Nutr 27: 17–22.
Spring KR 1991 Mechanism of fluid transport by epithelium. In: Handbook of Physiology, Vol 6. American Physiological Society, Bethesda, MD, 195–207.
Lohmann SM, Vaandrager AB, Smolenski A, Walter U, De Jonge HR 1997 Distinct and specific functions of cGMP-dependent protein kinases. Trends Biochem Sci 22: 307–312.
Volant K, Grishina O, Descroix-Vagne M, Pansu D 1997 Guanylin-, heat stable enterotoxin of Escherichia coli- and vasoactive intestinal peptide-induced water and ion secretion in the rat intestine in vivo. Eur J Pharmacol 328: 317–327.
Saunders DR, Sillery J, Surawica C, Tygat GN 1978 Effect of phenolphthalein on the function and structure of rodent and human intestine. Dig Dis 23: 909–913.
Gaginella T, Mascolo N, Izzo A, Autore G, Capasso F 1994 Nitric oxide as a mediator of bisacodyl and phenolphthalein laxative action: induction of nitric oxide synthase. J Pharmacol Exp Ther 270: 1239–1245.
Barclay DV, Gil-Ramos J, Mora JO, Durren H 1995 A packaged rice-based oral rehydration solution for acute diarrhea. J Pediatr Gastroenterol Nutr 20: 408–416.
Guiraldes E, Trivino X, Figueroa G, Parker M, Gutierrez C, Vasquez A, Harun A 1995 Comparison of an oral rice-based electrolyte solution and a glucose-based electrolyte solution in hospitalized infants with diarrheal dehydration. J Pediatr Gastroenterol Nutr 20: 417–424.
Pizarro D, Posada G, Sandi L, Moran JR 1991 Rice-based oral electrolyte solutions for the management of infantile diarrhea. N Engl J Med 324: 517–521.
Lifshitz F 1982 Perspectives of carbohydrate intolerance in infants with diarrhea. In: Lifshitz F (ed) Carbohydrate Intolerance in Infancy. Marcel Dekker, New York, 3–21.
Lebenthal E 1987 Role of salivary amylase in gastric and intestinal digestion of starch. Dig Dis Sci 32: 1155–1157.
Plaisancié P, Damoulin V, Chayvialle JA, Cuber JC 1996 Luminal peptide YY-releasing factors in the isolated, vascularly perfused rat colon. Endocrinol 151: 421–429.
Tatemoto K 1982 Isolation and characterization of peptide YY (PYY): a candidate gut hormone that inhibits pancreatic exocrine secretion. Proc Natl Acad Sci U S A 79: 2514–2518.
Corpe CP, Burant CF 1996 Hexose transporter expression in rat small intestine: effect of diet on diurnal variations. Am J Physiol 271:G211–G216.
Ferraris RP, Diamond J 1992 Crypt-villus site of glucose transporter induction by dietary carbohydrate in mouse intestine. Am J Physiol 262:G1069–G1073.
Dyer J, Scott D, Beechy RB, Care AB, Abbas KS, Shirazi-Beechy SP 1994 Dietary regulation of intestinal glucose transport. In: Lentze MJ, Grand RJ, Naim HY (eds) Mammalian Brush Border Membrane Proteins, Part II. Thieme-Verlag, Stuttgart, 65–72.
Shirazi-Beechy SP 1995 Molecular biology of intestinal glucose transport. Nutr Res Rev 8: 27–41.
Greeley G, Hashimoto T, Izukura M, Gomez G, Jeng J, Hill F, Lluis F, Thompson J 1989 A comparison of intraduodenally and intracolonically administered nutrients on the release of peptide-YY in the dog. Endocrinology 125: 1761–1765.
Liu C, Aloia T, Adrian T, Newton T, Bilchik A, Zinner M, Ashley S, McFadden D 1996 Peptide YY: A potential proabsorptive hormone for the treatment of malabsorptive disorders. Am Surg 62: 232–236.
Playford R, Domin J, Beacham J, Parmar K, Tatemoto K, Bloom S, Calam J 1990 Preliminary report: role of peptide YY in defence against diarrhoea. Lancet 335: 1555–1557.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported in part by National Institutes of Health Grant HD29255-03.
Rights and permissions
About this article
Cite this article
Wingertzahn, M., Teichberg, S. & Wapnir, R. Modified Starch Enhances Absorption and Accelerates Recovery in Experimental Diarrhea in Rats. Pediatr Res 45, 397–402 (1999). https://doi.org/10.1203/00006450-199903000-00018
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199903000-00018
