
Abstract
The present studies examine how agonist-induced increases in cytosolic Ca2+ concentration and sensitivity vary with maturation. Basilar arteries from term fetal (138-141 d) and nonpregnant adult sheep were denuded of endothelium, mounted for measurements of contractile tension, and then loaded with Fura-2 to enable estimation of cytosolic Ca2+ responses to both potassium and serotonin (5-hydroxytryptamine, 5-HT). In response to potassium, normalized values of intracellular Ca2+ and tension increased in parallel in both fetal and adult preparations; no age-related differences were apparent. In contrast, 5-HT increased Ca2+ sensitivity significantly more in fetal than in adult arteries. In the absence of extracellular Ca2+, 5-HT increased cytosolic Ca2+ in adult but not fetal arteries. In addition, responses to repeated applications of 5-HT in the absence of extracellular Ca2+ were exhausted more rapidly in fetal than in adult arteries. We interpret these data to indicate that vascular maturation involves important shifts in the mechanisms mediating cerebrovascular pharmacomechanical coupling. Specifically, the data suggest that normal development involves a reduction in the Ca2+ sensitizing effects of agonists with parallel increases in the agonist-induced intracellular Ca2+ release. In so doing, these studies offer one possible reason why vascular reactivity varies dramatically with age. From a pathophysiologic perspective, these studies also advance the possibility that failure to shift from the increased Ca2+ sensitivity typical of immature arteries may lead to vascular hyperreactivity in adult arteries.
Similar content being viewed by others


Main
The contraction of smooth muscle in response to agonist stimulation is mediated by multiple distinct intracellular signaling pathways. Activation of these pathways independent of changes in membrane potential is referred to as pharmacomechanical coupling and generally consists of two major components:1) increases in [Ca2+]i; and/or 2) increases in the sensitivity of the contractile proteins to Ca2+ ("Ca2+ sensitization")(1,2). Increases in cytosolic [Ca2+]i within vascular smooth muscle cells result from either increased release of Ca2+ from intracellular stores, or from increased influx of Ca2+ from the extracellular space. Both processes are closely associated with receptor-mediated activation of the phosphoinositide cascade which precipitates the formation of IP3 and diacylglycerol(3,4). Although increased cytosolic Ca2+ concentrations are widely recognized as the common second messenger initiating vascular contraction, it is also well established that receptor-mediated agonist stimulation of vascular smooth muscle elicits proportionately smaller changes in cytosolic Ca2+ for a given force production than does depolarization with K+, indicating that modulation of the Ca2+ sensitivity of the contractile apparatus is a second key mechanism governing contractile responses in vascular smooth muscle(5). The receptor-mediated signals governing both of these main components of pharmacomechanical coupling are mediated via multiple different G proteins, both large and small, which together ultimately determine overall vascular reactivity(1–5).
To date, the mechanisms involved in pharmacomechanical coupling have been studied almost exclusively in smooth muscle from adult arteries. Thus, relatively little information is available regarding the effects of maturation on these signaling systems, and in particular, how maturation may influence the balance between increases in cytosolic Ca2+ concentration, and increases in Ca2+ sensitivity, in response to a given agonist. On the other hand, it is well established that reactivity in fetal and neonatal arteries is strikingly different, and often much greater, than in adult arteries(6–9). Such maturational differences in reactivity may have important consequences for neonatal cerebrovascular homeostasis, and may contribute to the increased vulnerability of neonates to insults such as hypoxia and/or asphyxia, which often culminate in hypoxicischemic encophalopathy(10). Certainly, changes in membrane receptor density and affinity appear to be involved(8,11), but these differences alone cannot fully explain the observed age-related adjustments in vasoreactivity. Given these considerations, we hypothesized that developmental modifications of the main components of pharmacomechanical coupling may play a key role in age-related differences in cerebrovascular reactivity.
The major goal of the present work was to evaluate for the first time how agonist-induced increases in Ca2+ concentration and sensitivity vary with maturation. To address this goal, we determined these variables in basilar artery segments taken from term fetal lambs and nonpregnant adult sheep. Owing to its well recognized importance as both a physiologic and pathophysiologic contractile agonist, we chose 5-HT for use in these studies. An additional advantage offered by the use of 5-HT was that previous observations in our laboratory have demonstrated that reactivity to 5-HT varies markedly with maturation in the ovine basilar artery in a manner that cannot be fully explained by changes in the 5-HT receptor apparatus alone(7,12).
METHODS
General preparation. All procedures and protocols were approved by the Animal Research Committee of Loma Linda University. Segments of basilar artery were obtained from young adult sheep (18-24 mo old) and near-term (∼140-d gestation) fetuses. Segments of cranial arteries were withdrawn and placed in a Krebs' solution that contained (in mM): 122 NaCl, 25.6 NaHCO3, 5.56 dextrose, 5.17 KCl, 2.49 MgSO4, 1.60 CaCl2, 0.114 ascorbic acid, and 0.027 EGTA and was continuously bubbled with 95% O2-5% CO2. Arteries were cleaned of adhering tissues and cut into segments approximately 2-3 mm long. Each segment was mounted on wires and suspended between a force transducer and a post attached to a micrometer as previously described(13). Each vessel was examined at an optimal stretch that was determined as previously described(8). During all contractility experiments the contractile tensions were continuously digitized, normalized, and recorded using an on-line computer. To avoid any possible endothelium-mediated effects, we removed the endothelium by rotating each arterial segment around the mounting wires several times to gently scrape the entire luminal surface. The loss of endothelium produced by this method was verified by the absence of a vasodilator response to 1 µM acetylcholine. After verification of endothelium denudation, all arteries were contracted with 120 mM K+, after which one of the following two protocols were conducted.
Protocol 1. Ca2+ transients in smooth muscle cells in responses to K+ and 5-HT. The purpose of this protocol was to evaluate the effects of maturation on the time courses of changes in cytosolic Ca2+ produced by K+ depolarization and 5-HT. For these experiments, segments of basilar artery were incubated with the Ca2+-sensitive fluorescent dye Fura-2AM (5 µM) premixed with Pluronic F127 (final concentration 0.01%) for 3 h at 25°C under protection from light(14). The segments were then washed and attached to a fluorometer (CAF-110, Japan Spectroscopic) which alternately illuminated the segments with two excitation wavelengths of 340 and 380 nm. The fluorescence emitted from the preparation was collected into a photomultiplier circuit through a 500-nm filter. The ratio of the energies emitted at 340 and 380 nm (the F340/F380), which is a measure of intracellular [Ca2+]i, was calculated automatically and simultaneously registered along with isometric tension. Given that the time course and peak magnitude of contractile responses to 120 mM K+ was not altered after Fura loading, the possible acidification of the cells as a result of formaldehyde release from AM-ester hydrolysis(15) appears to have been negligible in our preparations. To distinguish the Fura-2 Ca2+ signal from autofluorescence or movement artifacts, the energies emitted at F340 and F380 were always monitored separately in addition to measurements of their ratio. Only those preparations in which F340 and F380 changed as mirror images of one another were used in the present study.
The contractile responses of Fura-loaded basilar rings were recorded during sequential cumulative administrations of potassium solution (20-120 mM) after which the arteries were washed and stabilized at resting levels of tone. Then, responses to sequential cumulative administrations of 5-HT(0.001-10 µM) were determined. After completion of this dose-response protocol, the minimum fluorescence was obtained by incubation of the preparations in Ca2+-free solution containing 140 mM K+, 2 mM EGTA, and 10 µM ionomycin (at pH 8.6 to optimize the ionomycin effect). After the determination of a minimum signal ratio, the vessels were incubated with an excess of Ca2+ (10 mM), which gives the maximum signal ratio. All measurements of fluorescence were then corrected for autofluorescence, and the concentration of intracellular Ca2+ was calculated using the standard equation of Grynkiewicz et al.(16).
Protocol 2. Effects of 5-HT on tension and[Ca2+]i in arterial preparations in the presence and absence of extracellular Ca2+. The purpose of this protocol was to evaluate the effects of maturation on the contribution of Ca2+ influx to the increases in cytosolic Ca2+ produced by K+ and 5-HT. To this end, arteries were loaded with Fura-2 as described above, after which the arteries were exposed to 120 mM K+ for approximately 10 min. This procedure defined the maximum contractile response to K+, and also optimally loaded all intracellular Ca2+ stores(14). Next, the bath solution was changed to a nominally free Ca2+ solution that contained only 10 µM Ca2+ to prevent disorganization of the membrane structures. After incubation in the nominally free Ca2+ solution, responses to 10 µM 5-HT were obtained after which minimum and maximum fluorescence were obtained as described above.
Data analysis and statistics. All values are given as means± SEM for the numbers of animals studied. The data sets obtained in these studies were all subjected to distribution analysis before making any statistical comparisons. Those data sets which were not normally distributed were log transformed. In all cases, these log transformations resulted in normal distributions (skew and kurtosis values between -1.0 and 1.0 overall). Statistical comparisons of normally distributed data were performed using both factorial and repeated measures ANOVA techniques, followed by post hoc comparisons via Duncan's analysis. Unless stated otherwise, n implies the number of animals, and statistical significance implies p < 0.05.
RESULTS
A total of 38 basilar arteries were prepared from 16 young adult sheep and 12 near-term fetuses, respectively. The unstressed baseline diameters of these arteries averaged 0.62 ± 0.01 mm in adults and 0.53 ± 0.01 in fetuses, respectively.
Ca2+ transients in responses to K+ depolarization and 5-HT. Baseline concentrations of Ca2+ averaged 107 ± 15 and 87 ± 17 nM in adult and fetal basilar arteries, respectively. Both 120 mM K+ and 10 µM 5-HT increased contractile force and intracellular Ca2+ concentration, as shown in Figure 1. In both adult and fetal arterial segments, 5-HT produced proportionally more force for a given increase in[Ca2+]i than did K+. To facilitate comparisons of differences between fetal and adult responses to 5-HT, responses of both tension and Ca2+ to 10 µM 5-HT were normalized relative to those to 120 mM potassium. Using this normalization, the 5-HT/Kmax ratios revealed that fetal arteries produced proportionately more tension for a smaller increase in cytosolic Ca2+ than did the adult arteries (Fig. 1). In fetuses, the 5-HT/Kmax ratios for tension were significantly greater than that in adults, but those for Ca2+ were less than those in adults, although this difference was not quite statistically significant. Overall, these data suggest that 5-HT-induced increases in Ca2+ sensitivity were more marked in fetal than in adult arteries.

Relation between contraction and increases in [Ca2+]i in ovine adult and fetal basilar arteries. Shown here are maximum increases in absolute tension (top panels) and [Ca2+]i (lower panels) in responses to 120 mM K+ and 10 µM 5-HT. The ratios of the responses to 5-HT relative to those to K+ are shown in the rightmost columns for both tension and [Ca2+]i. Vertical error bars indicate SE for seven adults and five fetuses. Asterisks indicate significant (p < 0.05) differences between corresponding age groups, and the § symbol indicates significant differences between responses to K+ and 5-HT. The finding that the 5-HT/K ratio was greater in the fetus for tension, but less in the fetus for [Ca2+]i, suggests that calcium sensitivity during 5-HT-induced contractions was greater in fetal than in adult basilar arteries.
In light of concerns that ratio-based estimates of absolute changes in Ca2+ concentrations may be unpredictably affected by artery-to-artery variations in the actual dissociation constant for Fura-2, we normalized the Ca2+-force relations observed in each artery such that the tension values at rest and at maximum response to K+ were 0 and 100%, respectively. In addition, the relative Ca2+ concentrations were normalized such that the minimum and maximum fluorescence ratios observed in response to potassium were taken as 0 and 100%, respectively. This approach facilitated comparisons of baseline Ca2+-force relations obtained in response to graded concentrations of K+ and 5-HT, independent of possible age-related variations in the dissociation constant for Fura-2.
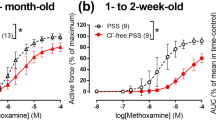
As shown in Figure 2, both K+ and 5-HT produced concentration-related increases in tension and intracellular Ca2+. Potassium increased contractile force similarly in fetal and adult basilar arteries, and only the increases observed at 24 mM were significantly greater in the fetal arteries. Correspondingly, potassium also increased the normalized intracellular Ca2+ values to a similar extent in both fetal and adult arteries. In contrast, 5-HT increased contractile tension proportionately more in fetal than in adult arteries. Accompanying this difference were corresponding significant age-related differences in sensitivity to 5-HT; separately determined pD2 values (-log ED50) for 5-HT averaged 6.95 ± 0.23 for adults and 7.34 ± 0.43 for fetuses. In spite of these age-related differences in responsiveness to 5-HT, however, the effect of 5-HT on normalized Ca2+ values in adult arteries was greater than or equal to the effect on fetal arteries at all concentrations. At 10 µM, this difference was statistically significant. Thus overall, responses of both tension and [Ca2+] to potassium varied little with age, whereas 5-HT was more potent and produced greater increases in tension, but stimulated smaller increases in Ca2+, in fetal compared with adult basilar arteries.

Effects of K+ and 5-HT on simultaneous changes in tension and [Ca2+]i. Both K+(left panels) and 5-HT (right panels) produced simultaneous concentration-related increases in tension (upper panels) and intracellular Ca2+ (lower panels). To correct for age-related differences in wall thickness and protein content, tension responses were normalized relative to the corresponding maximum response to K+. To correct for possible age-related differences in the dissociation constant for Fura-2, Ca2+ responses were also normalized relative to the maximum Ca2+ concentration observed in response to 120 mM K+ in both age groups. The data shown represent means and SE for multiple artery segments from five adults and five fetuses. Asterisks indicate significant (p < 0.05) differences between corresponding age groups. Note that the responses of tension and Ca2+ did not vary much with age for K+, but did for 5-HT.
To estimate the effects of maturation on Ca2+ sensitivity, the values of normalized tension shown in Figure 2 were plotted against their corresponding values of normalized Ca2+ for responses to both potassium and 5-HT (Fig. 3, upper panels). In these plots, the normalized Ca2+-force relations obtained in response to K+ were slightly left-shifted in fetal relative to adult arteries. However, for responses to 5-HT the magnitude of this age-related shift was much more pronounced, and suggested that high concentrations of 5-HT appeared to increase tension with little or no further increase of [Ca2+]i in the fetal arteries. Although these normalized Ca2+-force plots provide insight into the effects of age on Ca2+ sensitivity, the discontinuous nature of the data used to construct these plots precludes straightforward statistical comparisons between fetal and adult responses. To enable such statistical comparisons, the ratio of percent maximum tension to percent maximum Ca2+ was calculated as an index of Ca2+ sensitivity at each concentration of potassium and 5-HT applied. Given that these ratios were not normally distributed (composite skewness = 4.147, composite kurtosis value = 17.522), all analyses were performed on log transformed values of this ratio, which were normally distributed (composite skewness = 0.332, composite kurtosis value = 1.147). As shown in the lower left panel of Figure 3, the log values of this ratio differed significantly between fetal and adult arteries only at the lowest concentration of potassium used, suggesting that Ca2+ sensitivity is relatively independent of age, and does not change significantly in response to potassium activation in ovine basilar arteries. For responses to 5-HT, however, the values of the tension/Ca2+ ratio were generally greater than those observed for responses to potassium, suggesting that 5-HT increased Ca2+ sensitivity. Most importantly, the values of the tension/Ca2+ ratio were significantly greater in fetal than adult arteries at all 5-HT concentrations applied, suggesting that 5-HT increased Ca2+ sensitivity proportionately more in fetal than in adult basilar arteries.

Age-related differences in Ca2+-tension relations in response to 5-HT and K+. The simultaneous values of normalized tension and intracellular Ca2+ shown in Figure 2 are plotted against one another for the responses to K+ (upper left) and 5-HT (upper right). Please note that the vertical scale for 5-HT is twice that used for the K+ responses. For both of the upper two figures, the horizontal and vertical error bars indicate SE for tension and Ca2+, respectively. To enable statistical comparisons between corresponding fetal and adult responses, the ratio of percent maximum tension to percent maximum Ca2+ concentration was calculated for each concentration of K+ and 5-HT applied. The resulting values are plotted against their corresponding agonist concentrations in the lower two panels. Again, error bars indicate SE, and asterisks indicate significant (p < 0.05) differences between corresponding fetal and adult values. Statistical comparisons were performed using a repeated measures ANOVA on log transformed ratio data, followed by a Duncan's post hoc analysis. Note that the tension/Ca2+ ratio values were consistently greater in the fetus than the adult for responses to 5-HT, but not for responses to K+.
Ca2+ transients in response to 5-HT in the absence of extracellular Ca2+. To gain insight into possible age-related differences in the sources of activator Ca2+, the simultaneous responses of tension and intracellular Ca2+ to 5-HT were recorded in the presence and absence of extracellular Ca2+. In the presence of extracellular Ca2+, 10 µM 5-HT produced parallel increases in cytosolic Ca2+ in fetal and adult basilar arteries (Figs. 4 and 5). However, when extracellular Ca2+ was removed, the magnitude of the increase in cytosolic Ca2+ concentration observed in response to 5-HT was attenuated in adult arteries, but almost completely eliminated in fetal arteries, suggesting that fetal basilar arteries depend to a greater extent on external Ca2+ than do adult arteries. To examine this dependence in another way, we quantified the sizes of the responses of tension and Ca2+ to consecutive exposures to 5-HT in the absence of extracellular Ca2+ (Fig. 5). Even when age-related differences in initial tone and Ca2+ responses were eliminated by normalizing relative to the magnitudes of these initial responses, removal of extracellular Ca2+ more rapidly and severely attenuated tension and Ca2+ responses to 5-HT in fetal than in adult basilar arteries. Together, these data strongly suggest that fetal basilar arteries depend more on extracellular Ca2+ for activation by 5-HT, and are more easily depleted of intracellular Ca2+, than are adult basilar arteries.

Effects of extracellular Ca2+ withdrawal on 5-HT-induced increases in cytosolic Ca2+ in fetal and adult basilar arteries (BAS). Shown here are representative traces of ratio values, plotted against time, for Fura-2 fluorescence at wavelengths 340 and 380 nm (F340/F380) which reflect intracellular Ca2+ concentration. Note that 10 µM 5-HT dramatically increased cytosolic Ca2+ concentration in both adult(left panels) and fetal (right panels) basilar arteries in the presence of extracellular Ca2+ (upper panels), but in the absence of extracellular Ca2+ (lower panels) 5-HT increased Ca2+ only in adult arteries.

Effects of extracellular Ca2+ withdrawal on consecutive responses of tension and cytosolic Ca2+ to 5-HT in fetal and adult basilar arteries. Simultaneous responses of tension(upper panels) and cytosolic Ca2+ (lower panels) to 10 µM 5-HT were obtained three times in succession, first in the presence of extracellular Ca2+ (With), second in the absence of extracellular Ca2+ (Without#1), and then again in the absence of extracellular Ca2+ (Without#2). To correct for differences in wall thickness and protein content, tension values were normalized relative to maximum initial tone. To correct for differences in the magnitudes of the initial Ca2+ increases, Ca2+ values were also normalized relative to maximum initial values. In absolute units, these maximum initial values for Ca2+ concentration were significantly greater in adult (63.6 ± 8.8 nM) than in fetal (32.4 ± 5.2 nM) arteries. The values shown represent the means and SE for five adults and four fetuses. Asterisks indicate significant (p < 0.05) differences between corresponding fetal and adult values. Withdrawal of extracellular Ca2+ attenuated subsequent contractile responses, and corresponding increases in cytosolic Ca2+, more in fetal than in adult arteries.
DISCUSSION
The major new finding of this study is that the relative importance of intracellular Ca2+ release and increased Ca2+ sensitivity in responses to 5-HT differs dramatically in mature and immature ovine basilar arteries. The data strongly suggest that the functional importance of agonist-induced release of Ca2+ from intracellular stores is much greater in mature than in immature basilar arteries. Conversely, the data also suggest that agonist-induced increases in Ca2+ sensitivity are of much greater magnitude in immature than in mature cerebral arteries. Thus, maturation of ovine basilar arteries appears to shift the balance between Ca2+ release and Ca2+ sensitization in responses to 5-HT.
In the present work, direct parallel measurements of tension and[Ca2+]i in Fura-2-loaded vascular rings enable characterization of [Ca2+]i-force relations and also revealed the relative importance of intracellular and extracellular sources of Ca2+ for contractile responses to 5-HT. This approach thus permitted examination of the two main components of pharmacomechanical coupling: increased [Ca2+]i and increased myofilament sensitivity to Ca2+(1,2). Although numerous pathways (including membrane depolarization and hyperpolarization, changes in protein kinase C activity, and artery stretch) independently influence contractility, all of these influences ultimately can be attributed to effects on either [Ca2+]i or contractile protein calcium sensitivity.
Fura-2 offers many advantages including the ability to load smooth muscle cells without permeabilization or disruption, high fluorescence intensity, and most importantly the ability to measure intracellular Ca2+ concentrations independent of the concentration of the indicator, which in turn minimizes problems related to the leakage of the indicator from the tissue(16). Aside from these advantages, use of Fura-2 can also be limited by compositional and morphologic variations among different arteries to be compared. For example, differences in artery wall thickness, hydration, and protein content, which are typical of arteries of different maturational stages(7), could potentially alter the distribution of Fura-2 within smooth muscle cells due to variations in smooth muscle geometry and diffusion gradients, variations in esterase activity toward Fura-2AM, dissimilar incorporation of the fluorescent moiety into cellular organelles, alterations of the dissociation constant for Fura-2 or its binding to intracellular proteins, or shifts in spectral characteristics among different vascular preparations(17–21). In light of such limitations, all of which could potentially compromise the accuracy of absolute measurements of[Ca2+]i using Fura-2, the reliability of measurements of Ca2+ concentration is much greater for relative than for absolute changes. Thus, for comparisons of Ca2+-force relations among different artery types in the present studies, Ca2+ concentrations were normalized relative to the maximum response to depolarization by K+ and thus avoided many of the above mentioned inaccuracies(21–25).
Given that high K+ contracts smooth muscle via depolarization-mediated activation of voltage-operated Ca2+ channels and subsequent elevation of [Ca2+]i,[Ca2+]i-force relations obtained using K+ generally reflect basal myofilament Ca2+ sensitivity(21–25). Because the effects of K+ on normalized tension and [Ca2+]i were similar in adult and fetal arteries (Figs. 2 and 3), basal Ca2+ sensitivity does not appear to vary dramatically with age. In contrast to K+, many contractile agonists including 5-HT increase myofilament Ca2+ sensitivity and left-shift the[Ca2+]i-force relationship(17–25). The present data reinforce this view (Fig. 1) and further demonstrate that 5-HT-induced shifts in ovine cerebrovascular[Ca2+]i-force relations were dramatically different in immature and mature arteries (Figs. 2 and 3). In both fetal and adult basilar arteries, the K+-normalized[Ca2+]i-force relations for 5-HT were left-shifted relative to those for K+ (Fig. 3), and the magnitude of this increase in calcium sensitivity was significantly greater in fetal than in adult basilar arteries. At the highest concentrations of 5-HT applied, force increased with little or no further increment in[Ca2+]i in fetal, but not adult, basilar arteries, emphasizing the importance of increased Ca2+ sensitivity in fetal responses to 5-HT.
Because stretch can significantly modify myofilament Ca2+ sensitivity(24), the present studies were all performed at optimal stretch, which was independently determined in fetal and adult arteries using established methods(8). Thus the observed age-related differences in the effects of 5-HT on Ca2+ sensitivity cannot be attributed to differences in basal stretch and instead suggest that some aspect of coupling between 5-HT and contraction is up-regulated in fetal compared with adult basilar arteries. This suggestion is consistent with previous measurements of myofilament Ca2+ sensitivity in permeabilized immature ovine cerebral arteries(26) and with reports that Ca2+ sensitivity in endothelin-contracted rat mesenteric arteries is greater in newborns than in adults(27).
The second objective of the present study was to evaluate maturational differences in sources of activator Ca2+. Although the responses were less than observed in the presence of extracellular Ca2+(Figs. 4 and 5), 5-HT still increased contractile force and [Ca2+]i in adult arteries in the absence of extracellular Ca2+ due presumably to IP3-dependent mobilization of Ca2+ from intracellular pools(17,19,23,28). In contrast, withdrawal of extracellular Ca2+ essentially eliminated 5-HT-induced increases in [Ca2+]i in fetal arteries, although the contractile responses were maintained, albeit at a reduced level, which appeared slowly and gradually. Such retarded rates of contraction are typical of increases in myofilament Ca2+ sensitivity in the absence of increases in [Ca2+]i(14,23).
In our previous studies of Ca2+ sensitivity usingβ-escinpermeabilized ovine arteries(26), IP3 produced contractions and presumably intracellular Ca2+ release, in both adult and fetal cerebral arteries. In the present studies, however, 5-HT had little if any effect on Ca2+ release in fetal arteries. At least three explanations for this inconsistency are possible. First, the measurements [Ca2+]i may not have been sensitive enough to register small but effective increases in fetal [Ca2+]i release after withdrawal of extracellular Ca2+. Altered Ca2+ buffering due to variations in Fura-2 concentration or binding to intracellular proteins in fetal compared with adult arteries may have lowered apparent Ca2+ release. Functional or ultrastructural smooth muscle heterogeneity (which is pronounced in immature arteries due to high proportions of the synthetic relative to the contractile phenotype) might also differentially quench the Fura-2 signal and attenuate sensitivity to changes in[Ca2+]i. Second, spatial variations in Ca2+ mobilization may have affected Fura-2 measurements of Ca2+, but not measurements of contraction in permeabilized arteries. Fura-2 underestimates subsarcolemmal changes in[Ca2+]i, which alternatively may be detected using near-membrane indicators such as C18-Fura-2(29). Fura-2 predominantly measures mean cytoplasmic[Ca2+]i in contrast to other indicators which can detect focal and inhomogeneous increases in[Ca2+]i(30). Thus, temporal and spatial differences in intracellular Ca2+ mobilization between fetal and adult arteries might differentially alter the sensitivity of Fura-2 to changes in [Ca2+]i.Third, because Fura-2 accumulation in subcellular organelles is highly sensitive to vessel composition and loading conditions(31), Fura-2 may have accumulated in intracellular organelles more efficiently in fetal than adult arteries, resulting in greater buffering of small Ca2+ transients in the absence of extracellular Ca2+. If fetal smooth muscle sarcoplasmic reticulum is not fully developed or has a different ultrastructure and/or composition, accumulation and deesterification of Fura-2 may be modified, thus altering sensitivity to Ca2+ transients.
Aside from the differences between our studies based on β-escin permeabilized(26) and Fura-2-loaded preparations, both approaches strongly suggest that Ca2+ mobilization in response to 5-HT varies markedly with maturation and indicate that intracellular Ca2+ release is generally smaller in immature, than in mature, arteries, for contractile responses to 5-HT. The data also suggest that 5-HT significantly increases [Ca2+]i in fetal arterial smooth muscle cells (Fig. 1), due primarily to increased inward fluxes of extracellular Ca2+. Although the mechanisms responsible for these age-related differences in Ca2+ mobilization remain uncertain, it is possible that the mass of releasable intracellular Ca2+ is simply less in fetal than in adult arteries. In support of this possibility, 45Ca2+ release from the sarcoplasmic reticulum is reportedly less in newborn than in adult cultured arterial smooth muscle cells(32). This reduced release suggests that either the volume of sarcoplasmic reticulum, or its ability to release Ca2+, is reduced in immature compared with mature arteries. Consistent with the latter possibility are recent observations by Zhou et al.(33) that the density of IP3 receptors, which are presumably located primarily on the sarcoplasmic reticulum, are similar in fetal, newborn, and adult cerebral arteries. If the average amount of sarcoplasmic reticulum surface area per IP3 receptor is relatively stable during maturation, these observations suggest that the sarcoplasmic reticulum is present, but not fully functional, in immature, compared with mature, cerebral arteries. If intracellular Ca2+ is localized in two or more intracellular stores of which only one is sensitive to IP3(34), then age-related differences in 5-HT-induced Ca2+ mobilization may also reflect important basic differences in the distribution of intracellular Ca2+ among different intracellular stores.
Although the present studies focus exclusively on cerebral arteries, the observation that maturation alters intracellular Ca2+ mobilization may be a general phenomenon. In smooth muscle from bladder and trachea(35,36), the Ca2+ mobilized by many different agonists is depressed in immature relative to mature tissues. Myocardial Ca2+ release also appears to be less important for contraction in neonates than in adults(37). If maturational alteration of intracellular Ca2+ mobilization is a general phenomenon, it may also be possible that the effects of maturation on Ca2+ sensitivity, observed for the first time in our studies, may also apply generally. In essence, the increased Ca2+ sensitivity typical of immature artery responses to 5-HT, together with an increased dependence on extracellular calcium, appear to compensate for the concomitantly diminished ability to release intracellular Ca2+. In turn, the mechanisms involved in this apparent agonist-induced Ca2+ sensitization probably involve age-related changes in the role of G proteins in the coupling between receptor activation and Ca2+ mobilization(26).
Overall, the present data indicate that vascular maturation significantly alters the mechanisms mediating pharmacomechanical coupling, which helps explain why vascular reactivity varies so dramatically with age. Normal development apparently involves a reduction in the Ca2+-sensitizing effects of agonists with parallel increases in agonist-induced intracellular Ca2+ release. The data also suggest that failure to shift from the increased Ca2+ sensitivity typical of immature arteries may lead to the vascular hyperreactivity in adult arteries, such as that typical of many adult cardiovascular pathologies including hypertension and vasospasm. Although this possibility is highly speculative, the data suggest that contribution of elevated Ca2+ sensitivity to vascular hyperreactivity should be carefully evaluated in future studies.
Abbreviations
- 5-HT:
-
5-hydroxytryptamine; serotonin
- IP3:
-
inositol 1,4,5-trisphosphate
- [Ca2+]i:
-
concentration of intracellular Ca2+
References
Moreland RS, Cilea J, Moreland S 1991 Calcium dependent regulation of vascular smooth muscle contraction. Adv Exp Med Biol 308: 81–94
Somlyo AP, Somlyo AV 1994 Signal transduction and regulation in smooth muscle. Nature 372: 231–236
Zhang L, Bradley ME, Buxton ILO 1995 Inositol polyphosphate binding sites and their likely role in calcium regulation in smooth muscle. Int J Biochem Cell Biol 27: 1231–1248
Horowitz A, Menice CB, Laporte R, Morgan KG 1996 Mechanisms of smooth muscle contraction. Physiol Rev 76: 967–1003
Nishimura J, Khalil R, Drenth JP, van Breemen C 1990 Evidence for increased myofilament Ca2+ sensitivity in norepinephrine-activated vascular smooth muscle. Am J Physiol 259:H2–H8
Hayashi S, Park MK, Kuehl TJ 1985 Relaxant and contractile responses to prostaglandins in premature, newborn and adult baboon cerebral arteries. J Pharmacol Exp Ther 233: 628–635
Pearce WJ, Hull AD, Long DM, Longo LD 1991 Developmental changes in ovine cerebral artery composition and reactivity. Am J Physiol 261:R458–R465
Elliott SR, Pearce WJ 1994 Effects of maturation on alpha-adrenergic receptor affinity and occupancy in small cerebral arteries. Am J Physiol 267:H757–H763
Wagerle LC, Moliken W, Russo P 1995 Nitric oxide and beta-adrenergic mechanisms modify contractile responses to norepinephrine in ovine fetal and newborn cerebral arteries. Pediatr Res 38: 237–242
Johnston MV, Trescher WH, Taylor GA 1995 Hypoxic and ischemic central nervous system disorders in infants and children. Adv Pediatr 42: 1–45
Longo LD, Ueno N, Zhao Y, Zhang L, Pearce WJ 1996 NE-induced contraction, al-adrenergic receptors, and Ins(1:4, 5)P3 responses in cerebral arteries. Am J Physiol 270:H912–H923
Longo LD, Pearce WJ 1991 Fetal and newborn cerebral vascular responses and adaptations to hypoxia. Semin Perinatal 15: 49–57
Pearce WJ, Ashwal S, Long DM, Cuevas J 1992 Hypoxia inhibits calcium influx in rabbit basilar and carotid arteries. Am J Physiol 262:H106–H113
Himpens B, Kitazawa T, Somlyo AP 1990 Agonist-dependent modulation of Ca2+ sensitivity in rabbit pulmonary artery smooth muscle. Pflugers Arch 417: 21–28
Tsien RY, Pozzan T, Rink TJ 1982 Calcium homeostasis in intact lymphocytes: cytoplasmic free calcium monitored with new, intracellular trapped fluorescent indicator. J Cell Biol 94: 325–334
Grynkiewicz G, Poenie M, Tsien RY 1985 A new generation of Ca2+ indicators with greatly improved fluorescence properties. J Biol Chem 260: 3440–3450
Himpens B, Somlyo AP 1988 Free-calcium and force transients during depolarization and pharmacomechanical coupling in guinea-pig smooth muscle. J Physiol 395: 507–530
Bukoski RD, Bergmann C, Gairard A, Stoclet J-C 1989 Intracellular Ca2+ and force determined simultaneously in isolated resistance arteries. Am J Physiol 257:H1728–H1735
Karalki H 1989 Ca2+ localization and sensitivity in vascular smooth muscle. Trends Pharmacol Sci 10: 320–326
Cardeville-Atkinson C, Oster L, Thorin-Trescases N, Robert A, Boutinet S, Atkinson J 1993 Intracellular free Ca2+ and vasoconstriction determined simultaneously in the perfused rat tail artery. Am J Physiol 265:C1689–C1702
Bian K, Bukoski R 1995 Modulation of resistance artery force generation by extracellular Ca2+. Am J Physiol 269:H230–H238
Miwa Y, Hirata K, Matsuda Y, Suematsu M, Kawashima S, Yokoyama M 1994 Augmented receptor-mediated Ca2+ mobilization causes supersensitivity of contractile response to serotonin in atherosclerotic arteries. Circ Res 75: 1096–1102
Chen X, Rembold CM 1995 Phenylephrine contracts rat tail artery by one electromechanical and three pharmacomechanical mechanisms. Am J Physiol 268:H74–H81
Miyagi Y, Kobayashi S, Nishimura J, Fukui M, Kanaide H 1995 Resting load regulates vascular sensitivity by a cytosolic Ca2+-insensitive mechanism. Am J Physiol 268:C1332–C1341
Fukuzumi Y, Kobayashi S, Nishimura J, Kanaide H 1995 Cytosolic calcium-force relation during contractions in the rabbit femoral artery: time-dependency and stimulus specificity. Br J Pharmacol 114: 329–338
Akopov SE, Zhang L, Pearce WJ 1997 Physiological variations of ovine cerebrovascular calcium sensitivity. Am J Physiol 272:H2271–H2281
Touyz RM, Deng LY, Schiffrin EL 1995 Ca2+ and contractile responses of resistance vessels of WKY rats and SHR to endothelin-1. J Cardiovasc Pharmacol 26( suppl 3): S193–S196
Kobayashi S, Kitazawa T, Somlyo AV, Somlyo AP 1989 Cytozolic heparin inhibits muscarinic and α-adrenergic Ca2+ release in smooth muscle. J Biol Chem 264: 17997–18004
Etter EF, Kuhn MA, Fay FS 1994 Detection of changes in near-membrane Ca2+ concentrations using a novel membrane-associated Ca2+ indicator. J Biol Chem 269: 10141–10149
Rembold CM, Van Riper DA, Chen XL 1995 Focal[Ca2+]i increases detected by aequorin but not by fura-2 in histamine- and caffeine-stimulated swine carotid artery. J Physiol 488: 549–564
Goldman WF 1991 Spatial and temporal resolution of serotonin-induced changes in intracellular calcium in a cultured arterial smooth muscle cell line. Blood Vessels 28: 252–261
Fittingoff M, Krall JF 1988 Changes in inositol polyphosphate-sensitive calcium exchange in aortic smooth muscle cellsin vitro. J Cell Physiol 134: 297–301
Zhou L, Zhao Y, Nijland R, Zhang L, Longo L 1997 Ins(1,4,5)P3 receptors in cerebral arteries: changes with development and hypoxia. Am J Physiol 272:R1954–R1959
Golovina VA, Blaustein MP 1997 Spatially and functionally distinct Ca2+ stores in sarcoplasmic and endoplasmic reticulum. Science 275: 1643–1648
Grunstain MM, Rosenberg SM, Schramm CM, Pawlowski NA 1991 Mechanisms of action of endothelin 1 in maturing rabbit airway smooth muscle. Am J Physiol 260:L434–L443
Zderic SA, Sillen U, Liu GH, Snyder H, Duckett JW, Wein AJ, Levin RM 1993 Developmental aspects of bladder contractile function: evidence for an intracellular calcium pool. J Urol 150: 623–625
Wetzel GT, Klitzner TS 1996 Developmental cardiac electrophysiology: recent advances in cellular physiology. Cardiovasc Res 31:E52–E60
Author information
Authors and Affiliations
Additional information
Supported by U.S. Public Health Service Grants HL54120 and HD31266, and by the Loma Linda University School of Medicine.
Rights and permissions
About this article
Cite this article
Akopov, S., Zhang, L. & Pearce, W. Maturation Alters the Contractile Role of Calcium in Ovine Basilar Arteries. Pediatr Res 44, 154–160 (1998). https://doi.org/10.1203/00006450-199808000-00003
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199808000-00003
