
Abstract
Mature myocardium utilizes calcium released by the sarcoplasmic reticulum(SR) for cell contraction. Transient exposure of mature myocytes to caffeine is known to directly trigger Ca2+ release from the SR. In contrast, neonatal rabbit heart cells rely on transsarcolemmal Ca2+ influx for tension generation. SR function is decreased in immature heart and appears to play a minimal role as a calcium source. Accordingly, we hypothesized that neonatal rabbit myocytes would not respond to a caffeine pulse. Isolated neonatal and adult myocytes were paced to load the SR with calcium and then exposed to a 1-s pulse of 10 mM caffeine. As previously described, adult myocytes exhibited a brisk contraction in response to caffeine. Unexpectedly, neonatal myocytes also exhibited a similar, brisk response. These caffeine-induced contractions were not dependent on extracellular Ca2+ but were dependent upon the loading of SR Ca2+ stores. When SR Ca2+ stores were depleted by exposure to caffeine, mature myocytes exhibited only small, slow contractions in response to electrical field stimulation. Replenishing the SR Ca2+ stores resulted in normal, brisk contractions. In contrast, electrically stimulated contractions in immature myocytes were largely unaffected by caffeine-induced SR depletion. Thus, although neonatal myocytes are capable of loading and releasing calcium from the SR, such SR calcium release is not normally required for contraction in the developing heart. The minor role of SR Ca2+ release in immature rabbit heart may not result from immaturity of the SR, but rather from an inadequate mechanism to trigger SR calcium release.
Similar content being viewed by others


Main
Myocardial contractility is dependent on a transient rise in intracellular calcium concentration during an action potential. Depolarization of the cell opens transsarcolemmal, voltage-dependent Ca2+ channels, resulting in a localized rise in intracellular Ca2+ at the cell membrane. This calcium influx triggers the release of Ca2+ stored in the SR adjacent to the sarcolemma or t-tubules, which then provides the majority of the Ca2+ required for cell contraction(1–5). Transsarcolemmal Ca2+ influx contributes only about 10% of the total rise in intracellular Ca2+(6, 7). The SR also plays a predominate role in sequestering Ca2+ during cell relaxation(7, 8).
In comparison with mature myocardium, immature heart exhibits decreased SR function in a variety of different species. Studies using immunofluorescent probes and electron microscopy have demonstrated that the SR and t-tubular systems are underdeveloped in immature heart(9–11). Biochemical studies show a decrease in calcium pump density and calcium sequestration by SR vesicles(12, 13). Corresponding deficiencies in SR calcium release channels (ryanodine receptors) as well as Ca2+ pump mRNA and protein have been reported(14–17). Electrophysiologic studies from our laboratories have demonstrated evidence of SR-mediated Ca2+ release only under conditions of abnormal Ca2+ loading (prolonged depolarizations)(18, 19). Finally, as might be expected from these reports, we have also demonstrated that immature rabbit heart is dependent on transsarcolemmal calcium influx as the major source of the calcium required for cell contraction(19–22).
The goal of the present study was to use caffeine-induced contractions to examine age-related changes in the functional maturation of the SR in rabbit heart. In addition to augmenting depolarization-induced heart cell contraction amplitude, brief applications of caffeine have been shown to induce cell contractions directly by stimulating calcium release from the SR(23). Caffeine activates SR calcium release channels by increasing the frequency and duration of open channel events(24). Because neonatal rabbit myocytes have decreased SR function and do not exhibit evidence of significant SR calcium release during depolarization-induced contractions, we hypothesized that neonatal myocytes would not respond to a caffeine bolus in the same manner as adult myocytes.
METHODS
Cell isolation. Single, Ca2+-stable, cardiac ventricular myocytes were isolated by enzymatic digestion as previously described(19). Briefly, neonatal (2-5 d old), young (10 d old), juvenile (14 d old), and adult (2 mo old) New Zealand White rabbits were anticoagulated with sodium heparin and anesthetized with sodium pentobarbital. The heart of each animal was excised and rinsed free of blood in 3.5 mM Ca2+ Tyrode's solution (see below). The aorta was cannulated, and the heart was perfused with Ca2+-free Tyrode's solution for 3 min (2-18 mL/min; Minipulse, Gilson International, Middleton, WI). The perfusion solution was then changed to recirculated Ca2+-free Tyrode's solution, with 1 mg/mL of collagenase (Sigma Chemical Co., blend type L or H) and 0.04 mg/mL type XIV protease. After the digestion process was completed (9-11 min for neonates, up to 55 min for adults), the heart was perfused for 3 min with 0.1 mM Ca2+ Tyrode's solution to remove residual enzyme. Myocytes were then isolated by gently teasing apart the tissue with forceps. Isolated cells were stored in 0.1 mM Ca2+ Tyrode's solution and used within 5 h of isolation.
Cell selection. Cells were selected based on the following criteria: 1) the cell was firmly attached to the base of the perfusion chamber, 2) the cell consistently contracted with electrical stimulation (spontaneously contracting cells were excluded from the study), and 3) the cell contracted along its longitudinal axis.
Procedure and measurements. The cells were allowed to adhere to the bottom of the experimental chamber for 5 min before the beginning of the study. Selected cells were superfused with physiologic solution (1.8 mM Ca2+ Tyrode's solution). Positioning the mouth of the pipette close to the subject cell allowed for immediate delivery of the solution without dilution. The perfusing solution could be easily changed by a solenoid valve that was capable of providing a 1-s pulse of various solutions. The entire experimental apparatus was maintained at 37 °C.
Action potential-mediated contractions were induced by electrical field stimulation using platinum electrodes at 2× threshold (approximately 30 V) for a 3.5-ms duration every 3 s. The effect of a caffeine bolus was assessed by pausing the electrical stimulations and exposing the cell for 1 s to Tyrode's solution containing 10 mM caffeine. Cell contraction was measured using a video edge detector and was recorded for later analysis. The contraction amplitude and time to peak contraction was determined using p-Clamp software (Axon Instruments, Foster City, CA). This study was approved by the UCLA Chancellor's Animal Research Committee.
Tyrode's solution consisted of 136 mM NaCl, 5.4 mM KCl, 0.3 mM NaH2PO4, 1 mM MgCl, 10 mM HEPES, 4 mM D-mannitol, 0.6 mM thiamin HCl, 10 mM glucose, 2 mM pyruvic acid, and 1.8 mM CaCl2 (unless otherwise indicated), titrated to pH 7.4 with NaOH. All chemicals were obtained from Sigma Chemical Co. (St. Louis, MO) unless otherwise indicated.
RESULTS
Response to caffeine. Isolated myocytes received a train of eight stimulations every 3 s to load the SR with calcium. After a 3-s pause, the cells were then perfused with a pair of 1-s pulses with 10 mM caffeine.Figure 1 (upper traces) shows the response of an adult myocyte to the final three electrical stimulations as well as the two caffeine pulses. Electrical stimulation results in reproducible, brisk contractions in adult myocytes. The transient application of caffeine resulted in a similar(larger) contraction in the absence of electrical stimulation. As previously described, this contractile response is the result of caffeine-induced Ca2+ release from the SR(23). A second caffeine pulse does not elicit a contractile response, indicating that the caffeine-releasable pool of Ca2+ was depleted or otherwise inhibited.

Electrical and caffeine induced contractions.(Upper traces) Tracings of contraction amplitude are shown for an adult myocyte. A series of eight electrically stimulated contractions at 3-s intervals (to load the SR) was followed by a pair of 1-s pulses with 10 mM caffeine. The bars below the tracings indicate the timing of the sixth through the eighth electrical stimulations (vertical lines) and the caffeine pulses. For illustrative purposes, the contraction portion of each tracing is shown without the intervening rest periods. The initial caffeine pulse elicits a brisk contraction, larger than those induced by electrical stimulation. The second caffeine pulse does not elicit a contraction, indicating that the caffeine-releasable Ca2+ stores are depleted by the initial caffeine pulse. Similar results were seen in 13 cells isolated from four adult rabbits. (Lower traces) Tracings from a neonatal myocyte are shown for the same protocol. The initial caffeine pulse triggers a contraction much larger than the electrically stimulated contractions and relatively larger than that seen in adult cells. Depletion of the releasable Ca2+ stores is demonstrated by the lack of response to the second caffeine pulse. Similar results were observed in 11 cells isolated from three neonatal rabbits. Thus, immature myocytes are capable of sequestering and releasing Ca2+ in response to caffeine.
The same protocol was then used for neonatal myocytes. Contrary to our initial hypothesis, neonatal cells responded to the caffeine pulse in a manner similar to the adult myocytes. Exposure to caffeine elicits a rapid contraction, much larger than electrically stimulated contractions (Fig. 1, lower traces). This result was observed for all cells tested and suggests that the SR in neonatal myocytes is competent to both sequester and release large quantities of Ca2+. As with the adult cells, neonatal myocytes did not respond to the second pulse of caffeine, again indicating that the SR Ca2+ stores were depleted by the initial caffeine exposure. Similar contractile responses to caffeine have recently been reported in preliminary form by other investigators(25).
Controlling for transsarcolemmal calcium movement. To demonstrate that the caffeine-induced contractions are the result of the release of an intracellular calcium source (i.e. the SR) and not an extracellular source (sarcolemmal Ca2+ channel or the Na+-Ca2+ exchanger), experiments were performed to eliminate transsarcolemmal calcium influx. Identical experiments were performed using either Ni2+, to block transsarcolemmal calcium channels and the Na+-Ca2+ exchanger, or EGTA, to chelate extracellular calcium to diastolic levels (pCa approximately 7).
Isolated cells were electrically stimulated while the perfusing solution was changed to contain either 5 mM NiCl2 or 10 mM EGTA. Exposure of neonatal myocytes to either solution results in a total inhibition of contraction in response to the electrical stimulations (Fig. 2). However, each of these cells continues to respond to a caffeine pulse with large, brisk contractions. Thus, the caffeine-induced contractions are not dependent on an extracellular source of calcium ions.

Effects of EGTA and Ni2+ on caffeine-induced contractions. Traces of contraction amplitude are shown for neonatal myocytes during eight electrical stimulations and a caffeine-induced contraction. Caffeine-induced contractions are not dependent on transsarcolemmal Ca2+ influx. The contraction portion of each tracing is shown without the intervening rest periods. (A) Caffeine induced a large contraction under control conditions. (B) EGTA added to the perfusing solution chelates free Ca2+ to diastolic levels(pCa ≈ 7) and eliminates the electrically stimulated contractions but not the caffeine-induced contraction. Similar results were observed for eight myocytes isolated from two neonatal rabbits. (C) Addition of 5 mM NiCl2 to the perfusing solution blocks sarcolemmal Ca2+ influx and inhibits electrically stimulated cell contractions but not the caffeine-induced contraction. Similar results were observed for six myocytes isolated from two neonatal rabbits.
The role of caffeine in depleting SR Ca2+stores. The lack of response of the myocytes to the second pulse of caffeine suggests that the initial caffeine exposure is sufficient to essentially deplete the SR of its store of releasable Ca2+. However, this observation could also be explained as the rapid development of a desensitization of the Ca2+ release channels to caffeine. Accordingly, the time course of recovery from caffeine resistance was examined. In quiescent cells, the second caffeine pulse could be delayed by at least 2 min without recovery of caffeine sensitivity. However, when the myocytes were electrically stimulated to contract during the period between caffeine pulses, the myocytes regained their sensitivity to caffeine (Fig. 3). This result indicates that the recovery of caffeine sensitivity is dependent on reloading the SR with Ca2+ derived from transsarcolemmal Ca2+ influx. This experiment confirms the role of SR Ca2+ release in the caffeine-induced contractions observed in neonatal heart. Furthermore, this result indicates the capacity of the SR in immature heart to both release and sequester Ca2+ in a physiologically significant fashion.

Reloading of intracellular Ca2+ stores. Traces of contraction amplitude are shown for a neonatal myocyte. Intracellular Ca2+ stores were loaded by a train of electrical stimulations (first eight contractions) and then depleted by a 1-s pulse of 10 mM caffeine (large contraction). The contraction portion of each tracing is shown without the intervening rest periods. (A) A second series of eight electrical stimulations (right side of figure) replenished the SR Ca2+ stores as indicated by the second caffeine-induced contraction (final large contraction). (B) If the myocyte was not electrically stimulated after the first caffeine contraction, a second pulse of caffeine did not result in cell contraction (far right tracing, performed 27 s after the initial caffeine pulse). Thus, reloading of the cell Ca2+ stores during electrically stimulated cell contractions is required for subsequent caffeine-induced contractions. Similar results were obtained from four myocytes isolated from two neonatal rabbits.
The functional role of the SR Ca2+stores in developing heart. Several previous studies, using a variety of approaches, have demonstrated that immature rabbit heart is dependent on transsarcolemmal Ca2+ influx rather than SR Ca2+ release for cell contraction and tension generation(19–22). Those previous results are in marked contrast to the robust contractions in response to caffeine seen in Figure 1, lower traces. Accordingly, additional studies were performed to reevaluate the physiologic significance of SR Ca2+ release in developing heart using the same preparation.
SR Ca2+ stores were loaded to steady-state levels by a train of eight electrical stimulations and then depleted with a pair of 1-s caffeine pulses (as in Fig. 1). As noted previously, the effectiveness of SR Ca2+ depletion is demonstrated by the absence of contraction in response to a second caffeine pulse. The contractile response to a second series of eight electrical stimulations was then recorded. The initial contractions in adult myocytes after depletion of SR Ca2+ stores (Fig. 4, upper traces) were quite small in amplitude. Furthermore, the time required to reach the peak of the contraction was prolonged. This result reflects the small, slow contraction seen in mature heart preparations resulting from a gradual transsarcolemma Ca2+ influx in the absence of the rapid, dramatic release of Ca2+ from the SR. Subsequent contractions became progressively larger and more rapid as the result of a gradual reloading of the SR with Ca2+.

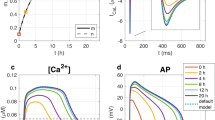
Contractions after caffeine-induced SR depletion. After a pair of caffeine-induced contractions to deplete SR Ca2+ stores, a series of eight electrically stimulated contractions were performed in neonatal and adult myocytes (see inset for protocol).Vertical bars indicate the timing of each stimulation. Adult myocytes (upper traces) exhibit a progressive increase in the contraction amplitude and decrease in the time to peak contraction as the SR is reloaded with Ca2+. Under the same conditions, neonatal myocytes exhibit little change in contraction amplitude or time to peak contraction. Reloading of the Ca2+ stores has little effect on contractions in neonatal heart.
In contrast, after caffeine-induced depletion of SR Ca2+ stores, neonatal myocytes exhibited little change in electrically stimulated contraction amplitude or time course (Fig. 4, lower traces). Studies of myocytes from 10- and 14-d-old rabbits exhibited intermediate levels of dependence on SR Ca2+ release.Figure 5 demonstrates the progressive dependence of contraction amplitude on SR Ca2+ release with development. Mean contraction amplitude is plotted against the number of stimulations after caffeine-induced SR Ca2+ depletion. Myocytes from neonatal and young rabbits exhibit little change in contraction amplitude when the SR is reloaded with Ca2+. In contrast, contraction amplitude of myocytes from juvenile and adult rabbits is markedly improved by reloading the SR. These results demonstrate that SR Ca2+ release does not play a major physiologic role in contraction in neonatal rabbit heart and suggest that maturation of excitation-contraction coupling is largely complete by 14 d of life.

Contraction amplitude during repletion of SR Ca2+ stores. Average contraction amplitude is plotted for each of eight electrical stimulations. After caffeine-induced depletion of SR Ca2+ stores, contraction amplitude was initially markedly inhibited in myocytes from adult (○, n = 6 cells from two rabbits) and 14-d-old(□, n = 8 cells from two rabbits) rabbits. Contraction amplitude gradually recovered during successive contractions. In contrast, neonatal(×, n = 5 cells from one rabbit) and 10-d-old myocytes(▵, n = 8 cells from one rabbit) exhibited little inhibition in response to SR depletion by caffeine and showed little increase in contraction amplitude when the intracellular Ca2+ stores were replenished. Restoration of SR Ca2+ stores during this protocol is documented in Figure 3. Thus, immature myocytes exhibited little dependence on caffeine-releasable Ca2+ stores. Values are normalized to the magnitude of a control stimulation and plotted as means ± SEM.
DISCUSSION
Previous reports have demonstrated the paucity or absence of a physiologic role for SR Ca2+ release in contraction of immature rabbit heart(19–22). Accordingly, we hypothesized that the immature myocytes would not exhibit a significant caffeine-induced Ca2+ release from the SR. The results of these experiments contradict this hypothesis. As Figures 1 and 3 demonstrate, immature rabbit heart is capable of both loading with Ca2+ and releasing significant quantities of stored Ca2+ when stimulated by caffeine. However, in the same immature cells, caffeine-mediated depletion of myocyte Ca2+ stores had little effect on contraction amplitude (Fig. 5) during an action potential. Thus, although immature myocytes are capable of using Ca2+ stores for cell contraction, these Ca2+ stores may have little or no role in cell contraction under physiologic conditions.
These experiments have not directly demonstrated that the caffeine-mediated contractions represent the release of SR Ca2+ stores. However, previous studies in adult myocardium have attributed these caffeine-induced contractions to the storage and release of Ca2+ from the SR(23). As illustrated by Figure 2, B and C, caffeine-induced contractions are independent of transsarcolemmal Ca2+ influx and therefore reflect the release of an intracellular source of Ca2+. Furthermore, a single caffeine-induced contraction appears to deplete the Ca2+ stores (repeated exposure to caffeine elicits no response; Fig. 1). Recovery of the response to caffeine is dependent upon repletion of the Ca2+ stores by action potential-induced contractions (Fig. 3). Caffeine is also known to activate adenylyl cyclase and to sensitize the contractile proteins to Ca2+. These other effects of caffeine are unlikely to significantly effect the peak magnitude of the caffeine-induced contractions (which occur within a few hundred milliseconds of the application of caffeine) because the effects of other positive ionotropic agents (e.g. β-adrenergic agonists) are not seen for seconds to minutes after drug exposure.
These findings clearly suggest that some form of SR Ca2+ store is responsible for the caffeine-induced contractions in immature rabbit heart. However, immature rabbit myocytes do not develop t-tubules until the 2nd wk of life and are deficient in the junctional form of SR, which adjoins the t-tubules and forms the dyadic cleft in mature myocardium(11). Accordingly, the Ca2+ released by caffeine in neonates may arise from corbular or longitudinal forms of SR(26, 27).
We have found that, similar to adult myocytes, neonatal myocytes respond to caffeine by releasing intracellular Ca2+ stores that are sufficient to elicit brisk, supernormal contractions. However, using the same myocytes, we found little evidence of SR function in immature myocytes when contractions were induced during an action potential. Mature myocytes recovered normal function by the third to the fifth stimulation after caffeine-induced SR Ca2+ depletion (Fig. 5). In contrast, replenishing the SR Ca2+ stores had little effect on the amplitude or time course of contractions in immature myocytes. The minor (10-20%) increase in contraction amplitude associated with SR reloading in neonatal and 10-d-old cells (Fig. 5) may reflect a small contribution of the SR to contraction in developing heart. Alternatively, this may represent competition between the contractile proteins and the SR Ca2+ pump for the exogenous Ca2+ entering the cytoplasm. Thus, after caffeine exposure, the unloaded SR may serve as a sink for Ca2+ without having a significant role in Ca2+ release.
These results complement those of Chin et al.(20) who used perfusion with Ca2+-free solutions to deplete the SR Ca2+ stores. When Ca2+ was added back to the bathing solution, they observed a small diminution of the initial contractions and hypothesized that there is a small but measurable contribution of the SR to neonatal contractions. However, this approach may deplete all intracellular Ca2+ stores as well as cytoplasmic Ca2+ binding sites. These sites would also compete with the contractile proteins for Ca2+ entering the cell on the first few stimulations. Recent reports using human atrial heart cells isolated at the time of cardiac surgery have not found evidence of postnatal changes in the role of the SR in myocyte contraction(30, 31). The difference between the human atrial preparation and other preparations of developing heart may reflect differences between species, tissues (atrial versus ventricular myocytes), physiologic states (surgical candidates with chronic cyanosis or atrial stretch), or developmental stages.
Previous reports have suggested that deficiencies in SR storage and release mechanisms in immature heart may explain the minor role of the SR in tension generation in the developing heart. However, the results from the present study suggest that the absence of a significant role for SR Ca2+ release in immature heart results from an inability of the Ca2+ influx during an action potential to stimulate Ca2+ release from the SR.
The inability to couple transsarcolemmal Ca2+ influx with SR Ca2+ release may result from ultrastructural differences between immature and mature myocytes. Possible candidates include: 1) a paucity of t-tubules and junctional SR; 2) physical separation of the sarcolemmal Ca2+ channels and the SR(26, 27); 3) absence of physical coupling (or colocalization) between the sarcolemmal Ca2+ channels and the SR calcium release channels(ryanodine receptors) in the dyadic cleft space(28, 29); or 4) an inadequate rate of change of the local intracellular [Ca2+] near the Ca2+-sensor of the ryanodine receptor. The age-related change in the role of SR Ca2+ release, demonstrated in Figure 5, occurs over a surprisingly brief period. However, during this same period, rabbit myocytes undergo a dramatic development of the t-tubule system(11). The correlation between these two observations suggests that the observed age-related changes in contractile function are the result of development of the t-tubule system as a means to trigger the release of SR Ca2+ stores.
In summary, our results indicate that, despite the evidence of age-related impairments in SR function described by other investigators, the SR in immature heart is capable of loading and releasing significant stores of calcium. Yet, neonatal cells do not use their SR under physiologic conditions. We speculate that the minor role of the SR in the developing rabbit heart is not a result of immaturity of the SR, but rather from an inadequate mechanism to trigger calcium release from the SR. Thus, attempts to improve cardiac function by increasing intracellular SR Ca2+ stores may be ineffectual. However, further elucidation of the age-related changes that enable coupling of transsarcolemmal Ca2+ influx to SR Ca2+ release will provide important clues to the basic mechanisms underlying Ca2+-induced Ca2+ release in mature heart.
Abbreviations
- SR:
-
sarcoplasmic reticulum
References
Fabiato A 1989 Appraisal of the physiological relevance of two hypothesis for the mechanism of calcium release from the mammalian cardiac sarcoplasmic reticulum: calcium-induced release versus charge-coupled release. Mol Cell Biochem 89: 135–140.
Cleeman L, Martin M 1989 Role of Ca2+ channel in cardiac excitation-contraction coupling in the rat: evidence from Ca2+ transients and contraction. J Physiol 432: 283–312.
Sham JS, Cleemann L, Morad M 1995 Functional coupling of Ca2+ channels and ryanodine receptors in cardiac myocytes. Proc Natl Acad Sci USA 92: 121–125.
Santana LF, Cheng H, Gomez AM, Cannell MB, Lederer WJ 1996 Relation between the sarcolemmal Ca2+ current and Ca2+ sparks and local control theories for cardiac excitation-contraction coupling. Circ Res 78: 166–171.
Lopez-Lopez JR, Shacklock PS, Balke CW, Wier WG 1995 Local calcium transients triggered by single L-type calcium channel currents in cardiac cells. Science 268: 1042–1045.
Wier WG 1990 Cytoplasmic [Ca2+] in mammalian ventricle: dynamic control by cellular processes. Annu Rev Physiol 52: 467–485.
Bers DM, Bassani JW, Bassani RA 1996 Na+-Ca2+ exchange and Ca fluxes during contraction and relaxation in mammalian ventricular muscle. Ann NY Acad Sci 779: 430–442.
Balke CW, Egan TM, Wier WG 1994 Processes that remove calcium from the cytoplasm during excitation-contraction coupling in intact rat heart cells. J Physiol 474: 447–462.
Anderson PA 1989 Maturation and cardiac contractility. Cardiol Clin 7: 209–255.
Nassar R, Reedy MC, Anderson PA 1987 Developmental changes in the ultrastructure and sarcomere shortening of the isolated rabbit ventricular myocyte. Circ Res 61: 465–483.
Chen F, Mottino T, Klitzner TS, Philipson KD, Frank JS 1995 Distribution of Na+-Ca2+ exchange protein in developing rabbit myocytes. Am J Physiol 268:C1126–C1132.
Mahony L, Jones LR 1986 Developmental changes in cardiac sarcoplasmic reticulum in sheep. J Biol Chem 261: 15257–15265.
Kaufman TM, Horton JW, White DJ, Mahony L 1990 Age-related changes in myocardial relaxation and sarcoplasmic reticulum function. Am J Physiol 259:H309–H316.
Brillantes AM, Bezprozvannaya S, Marks AR 1994 Developmental and tissue-specific regulation of rabbit skeletal and cardiac muscle calcium channels involved in excitation-contraction coupling. Circ Res 75: 503–510.
Tanaka H, Takagi N, Shigenobu K 1993 Inotropic effects of ryanodine and calcium antagonists on embryonic and hatched chick myocardium. J Dev Physiol 19: 235–240.
Vetter R, Kemsies C, Schulze W 1987 Sarcolemmal Na+-Ca2+ exchange and sarcoplasmic reticulum Ca2+ uptake in several cardiac preparations. Biomed Biochim Acta 46:S375–S81.
Wibo M, Bravo G, Godfraind T 1991 Postnatal maturation of excitation-contraction coupling in rat ventricle in relation to the subcellular localization and surface density of 1,4-dihydropyridine and ryanodine receptors. Circ Res 68: 662–273.
Klitzner T, Friedman WF 1988 Excitation-contraction coupling in developing mammalian myocardium: evidence from voltage clamp studies. Pediatr Res 23: 428–432.
Wetzel GT, Chen F, Klitzner TS 1995 Na+/Ca2+ exchange and cell contraction in isolated neonatal and adult rabbit cardiac myocytes. Am J Physiol 268:H1723–H1733.
Chin TK, Friedman WF, Klitzner TS 1990 Developmental changes in cardiac myocyte calcium regulation. Circ Res 67: 574–579.
Klitzner T 1991 Maturational changes in excitation-contraction coupling in mammalian myocardium. J Am Coll Cardiol 17: 218–255.
Nakanishi T, Seguchi M, Takao A 1988 Development of the myocardial contractile system. Experientia 44: 936–944.
Bassani RA, Bassani JW, Bers DM 1992 Mitochondrial and sarcolemmal Ca2+ transport reduce [Ca2+] during caffeine contractures in rabbit cardiac myocytes. J Physiol 453: 591–608.
Rousseau E, Meissner G 1989 Single cardiac sarcoplasmic reticulum Ca2+-release channel: activation by caffeine. Am J Physiol 256: H328–H333.
Balaguru D, Haddock P, Coetzee W, Artman M 1996 Cardiac sarcoplasmic reticulum in neonates can release calcium comparable to adult myocytes. Circ Res 941: 482
Dolber PC, Sommer JR 1984 Corbular sarcoplasmic reticulum of rabbit cardiac muscle. J Ultrastruct Res 87: 190–196.
Jorgensen AO, Shen AC, Arnold W, McPherson PS, Campbell KP 1993 The Ca2+-release channel/ryanodine receptor is localized in junctional and corbular sarcoplasmic reticulum in cardiac muscle. J Cell Biol 120: 969–980.
Ioshii SO, Imanaka-Yoshida K, Yoshida T 1994 Organization of calsequestrin-positive sarcoplasmic reticulum in rat cardiomyocytes in culture. J Cell Physiol 158: 87–96.
Langer GA, Peskoff A 1996 Calcium concentration and movement in the diadic cleft space of the cardiac ventricular cell. Biophys J 70: 1169–1182.
Hatem S, Sweeten T, Vetter V, Morad M 1995 Evidence for presence of Ca2+ stores in neonatal human atrial myocytes. Am J Physiol 268:H1195–H1201.
Hatem S, Benardeau A, Ruecker-Martin C, Marty I, deChamisso P, Villex M, Mercadier J 1997 Different compartments of sarcoplasmic reticulum in the excitation-contraction coupling process in human atrial myocytes. Circ Res 80: 345–353.
Acknowledgements
The authors thank Michael Bransby for his excellent technical assistance and Tania Helgren for help in the preparation of this manuscript.
Author information
Authors and Affiliations
Additional information
Supported in part by funds from the National Institutes of Health(HL02723), the American Heart Association (93006170), the American Heart Association, Greater Los Angeles Affiliate (981-CS1), the Laubisch Fund, and the J. H. Nicholson Endowment.
Rights and permissions
About this article
Cite this article
Miller, M., Friedman, W. & Wetzel, G. Caffeine-Induced Contractions in Developing Rabbit Heart. Pediatr Res 42, 287–292 (1997). https://doi.org/10.1203/00006450-199709000-00007
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199709000-00007
